Download as docx, pdf, or txt
You might also like
- Cathlab Manual Coronary AngiographyDocument28 pagesCathlab Manual Coronary AngiographyNavojit Chowdhury100% (5)
- Basics of CathlabDocument39 pagesBasics of CathlabMemon RazakNo ratings yet
- Cardiac Catheterization ProcedureDocument10 pagesCardiac Catheterization ProcedureDimpal Choudhary100% (5)
- Basic Objectives of Color and Spectral DopplerDocument5 pagesBasic Objectives of Color and Spectral DopplerAsaad Baloch100% (2)
- Pacemaker ImplantDocument62 pagesPacemaker Implantadins100% (2)
- Topic 2 ExercisesDocument6 pagesTopic 2 ExercisesRaniel Pamatmat0% (1)
- AR& Inventory Management AR& Inventory ManagementDocument11 pagesAR& Inventory Management AR& Inventory Managementchesca marie penarandaNo ratings yet
- Unit Plan-Chapter 12-Antebellum Culture and ReformDocument39 pagesUnit Plan-Chapter 12-Antebellum Culture and Reformapi-237585847No ratings yet
- Saturn and Mars in Marital DisharmonyDocument20 pagesSaturn and Mars in Marital DisharmonyTej K Zadoo100% (1)
- Angiography: Study of Blood Vessels, by The Use of Contrast To Make TheDocument21 pagesAngiography: Study of Blood Vessels, by The Use of Contrast To Make TheFarhanNo ratings yet
- Angiographic ProceduresDocument26 pagesAngiographic ProceduresJane Garcia100% (1)
- Unit 6 Cardiac Catheterization and AngiographyDocument28 pagesUnit 6 Cardiac Catheterization and AngiographyJack Tomar100% (1)
- Angiographic ThoracalisDocument22 pagesAngiographic ThoracalisermaendahNo ratings yet
- Coronary AngiogramDocument58 pagesCoronary AngiogramEllaine Jennel100% (3)
- Practice Guidelines For Juniors 01 June 2016Document3 pagesPractice Guidelines For Juniors 01 June 2016ElaineNo ratings yet
- Intravascular Ultrasound Technique: An Alternate To Coronary Angiography (Super Simplified Edition)Document13 pagesIntravascular Ultrasound Technique: An Alternate To Coronary Angiography (Super Simplified Edition)Taanish Kumaar100% (1)
- ScriptDocument5 pagesScriptKelly SisonNo ratings yet
- Cerebral AngiographyDocument3 pagesCerebral AngiographyBiway RegalaNo ratings yet
- Word - TEVARDocument6 pagesWord - TEVARPutra AchmadNo ratings yet
- Invasive Cardiology LectureDocument49 pagesInvasive Cardiology LectureJibran Jones GarciaNo ratings yet
- Percutaneous Transluminal Coronary AngioplastyDocument22 pagesPercutaneous Transluminal Coronary AngioplastyArya Gaunker100% (1)
- Imaging in Subarachnoid Hemorrhage - Overview, Radiography, Computed TomographyDocument13 pagesImaging in Subarachnoid Hemorrhage - Overview, Radiography, Computed TomographySaraNo ratings yet
- Spinal DsaDocument15 pagesSpinal DsaanuroxxxNo ratings yet
- Interventional Radiology & AngiographyDocument45 pagesInterventional Radiology & AngiographyRyBone95No ratings yet
- Cannulation of The Internal Jugular Vein: Robert Cambria, MDDocument9 pagesCannulation of The Internal Jugular Vein: Robert Cambria, MDAndres BernalNo ratings yet
- Distal Transradial Access As Default Approach For Coronary Angiography and Interventions CDT 2019Document7 pagesDistal Transradial Access As Default Approach For Coronary Angiography and Interventions CDT 2019marcos.danilloNo ratings yet
- Cardiac CathDocument39 pagesCardiac CathMark M. AlipioNo ratings yet
- 480 FullDocument6 pages480 FullStamenko S. SusakNo ratings yet
- PERICARDIOCENTESISDocument25 pagesPERICARDIOCENTESISrastaNo ratings yet
- Up To Date. GasometryDocument46 pagesUp To Date. GasometryGuardito PequeñoNo ratings yet
- Final Versionof Vascular Chaptersfor OHOSFigueiredo BhattacharyaDocument44 pagesFinal Versionof Vascular Chaptersfor OHOSFigueiredo BhattacharyaKing ThiyagaNo ratings yet
- Vascular Imaging EquipmentsDocument50 pagesVascular Imaging EquipmentsRohit nikam0% (1)
- IrcerebralDocument30 pagesIrcerebralJamel MacasNo ratings yet
- Heart CareDocument14 pagesHeart CareArman CareNo ratings yet
- 42nd Issue-Article 136Document2 pages42nd Issue-Article 136Sohil ElfarNo ratings yet
- Askep Ps DGN Tindakan Invasif & INB KD 2021Document91 pagesAskep Ps DGN Tindakan Invasif & INB KD 2021gayuspatarru123No ratings yet
- AVF NewDocument81 pagesAVF NewBasit AliNo ratings yet
- Coronary Angiography and Left VentriculographyDocument2 pagesCoronary Angiography and Left Ventriculographyrrpandey4854No ratings yet
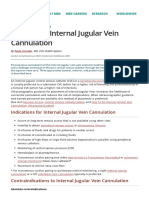
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDocument9 pagesHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenNo ratings yet
- A Combined Epi-And Subdural Direct Approach To Carotid-Ophthalmic Artery AneurysmsDocument6 pagesA Combined Epi-And Subdural Direct Approach To Carotid-Ophthalmic Artery AneurysmsСергей НайманNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasDharlyn MungcalNo ratings yet
- Date 12 Oct 2023Document6 pagesDate 12 Oct 2023mughallaiba901No ratings yet
- Redo CabgDocument36 pagesRedo CabgSantanico De CVT deozaNo ratings yet
- Arterial Blood Gases - UpToDateDocument41 pagesArterial Blood Gases - UpToDateMelanny Perez GonzalesNo ratings yet
- Endovascular Coiling - UCNIDocument6 pagesEndovascular Coiling - UCNIKasturi SriramNo ratings yet
- Cath Lab Optimal - Angiographic - Views - For - Invasive - Coronary - Angiography - A - Guide 2Document23 pagesCath Lab Optimal - Angiographic - Views - For - Invasive - Coronary - Angiography - A - Guide 2蘇柏霖No ratings yet
- CT - Cardiac Tamponade 2013Document5 pagesCT - Cardiac Tamponade 2013floNo ratings yet
- 209 FullDocument15 pages209 FullWilson Fransiskus Chia GirsangNo ratings yet
- Cardiac CatheterizationDocument9 pagesCardiac CatheterizationAnurag Gupta100% (2)
- A Dual (Brachial and Ipsytralateral Femoral)Document11 pagesA Dual (Brachial and Ipsytralateral Femoral)drstojanmitreskiNo ratings yet
- Sop of Doing Inavsive Line (Ijv) in IcuDocument12 pagesSop of Doing Inavsive Line (Ijv) in Icuqc.carcinovaNo ratings yet
- Ulnar Acces 2006Document10 pagesUlnar Acces 2006Rodrigo MartinNo ratings yet
- How To Do Aorta InterventionDocument80 pagesHow To Do Aorta InterventionMohamad ZulfikarNo ratings yet
- CVP Line CareDocument37 pagesCVP Line CareArvindJoshiNo ratings yet
- Intervetional Radiology PresentationDocument24 pagesIntervetional Radiology Presentationmalueth jacobNo ratings yet
- O o o o o o o o o o o oDocument9 pagesO o o o o o o o o o o oAshish PandeyNo ratings yet
- Basics of Microvascular SurgeryDocument33 pagesBasics of Microvascular SurgeryPratikshya KothiaNo ratings yet
- Paramedian Suboccipital Mini-Craniectomy For Evacuation of Spontaneous Cerebellar HemorrhageDocument6 pagesParamedian Suboccipital Mini-Craniectomy For Evacuation of Spontaneous Cerebellar HemorrhagemarceloNo ratings yet
- Paramedian Suboccipital Mini-Craniectomy For Evacuation of Spontaneous Cerebellar HemorrhageDocument6 pagesParamedian Suboccipital Mini-Craniectomy For Evacuation of Spontaneous Cerebellar HemorrhagemarceloNo ratings yet
- Catheter Ablation of Intramural Outflow Tract Premature Ventricular Complexes - A Multicentre StudyDocument9 pagesCatheter Ablation of Intramural Outflow Tract Premature Ventricular Complexes - A Multicentre Studyahmed mostafaNo ratings yet
- Peripheral Intervention: Ardhiana KasabaDocument36 pagesPeripheral Intervention: Ardhiana KasabaFitri ShabrinaNo ratings yet
- CT Head AnatomyDocument57 pagesCT Head AnatomyMaajid Mohi Ud Din MalikNo ratings yet
- Emergency Procedures: - Defibrillation in CPRDocument20 pagesEmergency Procedures: - Defibrillation in CPRDuy Phương NguyễnNo ratings yet
- Cardiac Surgical Operative AtlasFrom EverandCardiac Surgical Operative AtlasThorsten WahlersNo ratings yet
- Assignment (Individual)Document3 pagesAssignment (Individual)wan hanisaNo ratings yet
- Radiology Name: Nuramalina Binti Halim Sex: F MRN No.: 00191403 Room No.: IC No.: 971108305060Document3 pagesRadiology Name: Nuramalina Binti Halim Sex: F MRN No.: 00191403 Room No.: IC No.: 971108305060wan hanisaNo ratings yet
- Health Technology Assessment Section Medical Development Division Ministry of Health Malaysia 016/2009Document15 pagesHealth Technology Assessment Section Medical Development Division Ministry of Health Malaysia 016/2009wan hanisaNo ratings yet
- Dis Team - CT VS Mri - LatestDocument32 pagesDis Team - CT VS Mri - Latestwan hanisaNo ratings yet
- 249 FullDocument7 pages249 Fullwan hanisaNo ratings yet
- Please Rate Our Service: Thank You Have A Nice Day!Document3 pagesPlease Rate Our Service: Thank You Have A Nice Day!wan hanisaNo ratings yet
- Acceleration Claim 1-KMDocument6 pagesAcceleration Claim 1-KMskmNo ratings yet
- SDN PCo 03Document23 pagesSDN PCo 03UwedaNo ratings yet
- PE10 Lesson5-Hiphop v2Document19 pagesPE10 Lesson5-Hiphop v2OSMAN LUMBOSNo ratings yet
- Job Interview Questions For A Tour GuideDocument4 pagesJob Interview Questions For A Tour GuidetemiNo ratings yet
- MT800A Quick Installation GuideDocument2,110 pagesMT800A Quick Installation Guideneo_4dNo ratings yet
- Control M em MigrationDocument76 pagesControl M em Migrationis3khar0% (1)
- Heat Transfer Class Project: Powerpoint Presentation File Name It: Project2014-# in Class Roll-#In Class RollDocument3 pagesHeat Transfer Class Project: Powerpoint Presentation File Name It: Project2014-# in Class Roll-#In Class RollSwapnil BhattacharyaNo ratings yet
- PMP Test Paper 101 Questions For 2hours PDFDocument21 pagesPMP Test Paper 101 Questions For 2hours PDFAnonymous 6pfaIAh8100% (1)
- Mahalakshmi Ashtakam Stotra in HindiDocument3 pagesMahalakshmi Ashtakam Stotra in HindiAnuja BakareNo ratings yet
- Comprehensive RubricDocument1 pageComprehensive Rubricartifactsmu4698No ratings yet
- MentalismDocument3 pagesMentalismDiệp Thuận100% (1)
- SULIT 4551/3 Biologi Kertas 3 Sept 2007 SeptemberDocument13 pagesSULIT 4551/3 Biologi Kertas 3 Sept 2007 SeptemberhasimahazitNo ratings yet
- Few Good Men AssignmentDocument3 pagesFew Good Men AssignmentBellaNo ratings yet
- Bard NoteDocument20 pagesBard NoteAmulya Kumar SahuNo ratings yet
- Browder's First Deposition - April 15th, 2015Document137 pagesBrowder's First Deposition - April 15th, 2015Lee StranahanNo ratings yet
- Stoichiometric Tables: Batch System Stoichiometric TableDocument4 pagesStoichiometric Tables: Batch System Stoichiometric TableSKRNo ratings yet
- Law Individual Assignment by JustinDocument5 pagesLaw Individual Assignment by JustinJustin JJNo ratings yet
- ProvRem - DM WenceslaoDocument3 pagesProvRem - DM WenceslaoKath LimNo ratings yet
- OB AbilityDocument21 pagesOB Abilityrimshahkiyani1234100% (2)
- Mine Seismology: Data Analysis and Interpretation: S.N. GlazerDocument421 pagesMine Seismology: Data Analysis and Interpretation: S.N. GlazerFrancisco Villaseca100% (1)
- Antepartum, Intrapartum & Postpartum: Mild PreeclampsiaDocument4 pagesAntepartum, Intrapartum & Postpartum: Mild PreeclampsiaA. P.No ratings yet
- Caribbean Internet CafeDocument3 pagesCaribbean Internet Cafem.h.n.g67% (3)
- AbakadaDocument1 pageAbakadaChery-Ann Gorospe100% (1)
- 2017 - Orientalism and The Qur Ān A ProlegomenonDocument8 pages2017 - Orientalism and The Qur Ān A ProlegomenonMohammad -No ratings yet
- Would See Every Cloud of Doubt: Instrument Record Claim Encumbrance ProceedingDocument4 pagesWould See Every Cloud of Doubt: Instrument Record Claim Encumbrance ProceedingdaryllNo ratings yet
- Screen Time Final EssayDocument5 pagesScreen Time Final EssayAlisha PowellNo ratings yet