Download as pdf or txt
You might also like
- Health Teaching Plan For Dengue Hemorrhagic FeverDocument3 pagesHealth Teaching Plan For Dengue Hemorrhagic Fevershiramu100% (5)
- FentanylDocument2 pagesFentanylKatie McPeek63% (8)
- Diabetes Mellitus Nursing Care PlanDocument7 pagesDiabetes Mellitus Nursing Care PlanjamieboyRN91% (32)
- Drug Study-PsychDocument5 pagesDrug Study-Psychrc_lacampuinganyahooNo ratings yet
- Marjorie ncp8Document2 pagesMarjorie ncp8Jovel CortezNo ratings yet
- Drug TBDocument1 pageDrug TBjpmNo ratings yet
- FGFKSJHGFKHSFGKJHSDGLDocument11 pagesFGFKSJHGFKHSFGKJHSDGLyannajsdhfjskdhfjkshjfhNo ratings yet
- KUSAIN - NCP IN NCM 112 RLE ConstipationDocument2 pagesKUSAIN - NCP IN NCM 112 RLE Constipationjay kusainNo ratings yet
- Myasthenia GravisDocument2 pagesMyasthenia GravispsyNo ratings yet
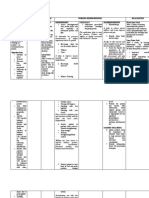
- College of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationDocument2 pagesCollege of Nursing: Assessment Diagnosis Analysis Planning Implementation Rationale EvaluationjoanneNo ratings yet
- Cardaic Emergency Drugs.Document13 pagesCardaic Emergency Drugs.Alma SusanNo ratings yet
- Myasthenia GravisDocument18 pagesMyasthenia GravismarthanyalangluonyNo ratings yet
- Acute Polymorphic Psychotic Disorder With Symptoms of SchizophreniaDocument4 pagesAcute Polymorphic Psychotic Disorder With Symptoms of SchizophreniadysphileNo ratings yet
- HTP Tonic Clonic Seizure NeuroWardDocument5 pagesHTP Tonic Clonic Seizure NeuroWardMeryville JacildoNo ratings yet
- Drug Study - DiazepamDocument2 pagesDrug Study - DiazepamCerie Anne Olay40% (5)
- DexamethasoneDocument1 pageDexamethasoneACOB, Jamil C.No ratings yet
- Nursing Care Plan Assessment Diagnosis and Inference Objectives Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Assessment Diagnosis and Inference Objectives Nursing Intervention Rationale Evaluationjay kusainNo ratings yet
- NCPDocument9 pagesNCPHendy Hency YunusNo ratings yet
- Geria NCP, Dela CruzDocument7 pagesGeria NCP, Dela CruzStephany Dela CruzNo ratings yet
- NCP ConstipationDocument3 pagesNCP ConstipationKingJayson Pacman06No ratings yet
- NURSING CARE PLAN (For Case Study)Document2 pagesNURSING CARE PLAN (For Case Study)Kathleen Martinez100% (1)
- Medicamentos Antagonistas OpioidesDocument1 pageMedicamentos Antagonistas OpioidescamargotyuNo ratings yet
- Drug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesDocument1 pageDrug Mechanism of Action/side Effects Indication/ Contraindication Nursing ResponsibilitiesSheryhan Tahir BayleNo ratings yet
- NURSING CARE PLAN-Impired Physical MobilityDocument5 pagesNURSING CARE PLAN-Impired Physical MobilityKathleen Leana Viray JeanjaquetNo ratings yet
- Man Aging Diz Ziness: Following Concus Sion/mild Traumatic Brain Injur yDocument2 pagesMan Aging Diz Ziness: Following Concus Sion/mild Traumatic Brain Injur ychhayasawang4No ratings yet
- M&N MGMTDocument3 pagesM&N MGMTMark Jefferson LunaNo ratings yet
- Extrapyramidal Symptom AssessmentDocument6 pagesExtrapyramidal Symptom AssessmentJNo ratings yet
- InsomniaDocument32 pagesInsomniaemanmohamed3444No ratings yet
- Delirium Screening PRISMEDocument1 pageDelirium Screening PRISMEWardah Fauziah El SofwanNo ratings yet
- Name: Grace AGE: 28 Gender: Female Assessment Nursing Diagnosis Objectives Nursing Intervention Rationale Evaluation Subjective: GeneralDocument2 pagesName: Grace AGE: 28 Gender: Female Assessment Nursing Diagnosis Objectives Nursing Intervention Rationale Evaluation Subjective: GeneralRainier IbarretaNo ratings yet
- NG Acute PoisoningDocument7 pagesNG Acute Poisoningshaker al baharNo ratings yet
- Prenatal Care Common Discomforts During PregnancyDocument5 pagesPrenatal Care Common Discomforts During PregnancyKarina MadriagaNo ratings yet
- Cushing'S Syndrome Female Ward Staff NAFH ProgrammeDocument23 pagesCushing'S Syndrome Female Ward Staff NAFH ProgrammeJaron JarsNo ratings yet
- Drug Study - Ketorolac, Tromethamine, OmeprazoleDocument4 pagesDrug Study - Ketorolac, Tromethamine, OmeprazolemikErlhNo ratings yet
- Material, Vincent M. (NCP Seizure, Head Trauma, CVA)Document33 pagesMaterial, Vincent M. (NCP Seizure, Head Trauma, CVA)vincent materialNo ratings yet
- Gordons Finalize After 10yrsDocument4 pagesGordons Finalize After 10yrsShanelli GaviolaNo ratings yet
- Impaired Swallowing Related To Dysphagia Secondary To Dry Oral MucosaDocument3 pagesImpaired Swallowing Related To Dysphagia Secondary To Dry Oral MucosaJUN JUN PALISOC100% (1)
- Drug Study Sugaton Week 1 2ND SemDocument3 pagesDrug Study Sugaton Week 1 2ND SemPrincess Faniega SugatonNo ratings yet
- Discharge Planning and NCP SDocument8 pagesDischarge Planning and NCP SRainier RamosNo ratings yet
- HTPDocument4 pagesHTPAlyssa Jade SandovalNo ratings yet
- Case AnalysisDocument10 pagesCase AnalysisJuvida, Clarissa A.No ratings yet
- OmeprazoleDocument2 pagesOmeprazoleIvan Matthew SuperioNo ratings yet
- DS ParatramDocument1 pageDS ParatramLarr SumalpongNo ratings yet
- Haloperidol Drug StudyDocument2 pagesHaloperidol Drug StudyLanzen DragneelNo ratings yet
- Textbook of Pediatric Dentistry-3rd EditionDocument18 pagesTextbook of Pediatric Dentistry-3rd EditionAnna NgNo ratings yet
- Submitted By: Swati Markandey Ashish Arya: Department of Pedodontics Govt. College of Dentistry, IndoreDocument40 pagesSubmitted By: Swati Markandey Ashish Arya: Department of Pedodontics Govt. College of Dentistry, Indorepriti adsulNo ratings yet
- CP-Rheumatic Heart Disease LandscapeDocument13 pagesCP-Rheumatic Heart Disease Landscapedecebelle alabaNo ratings yet
- CPG 150008Document1 pageCPG 150008jaime villanazulNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care Plankehyrie100% (2)
- HeatstrokeDocument16 pagesHeatstrokejimwelluismNo ratings yet
- Ob NCP and Drug StudyDocument3 pagesOb NCP and Drug StudyRomhea MatmyrNo ratings yet
- Levetiracetam Drug StudyDocument2 pagesLevetiracetam Drug Studykaycelyn jimenez50% (2)
- Headache SummaryDocument3 pagesHeadache Summaryhameedsabah36No ratings yet
- Management of Seizures in Palliative Care: Journal ClubDocument63 pagesManagement of Seizures in Palliative Care: Journal ClubleungsukhingNo ratings yet
- Reactive - Arthritis - TextDocument2 pagesReactive - Arthritis - TextSathvika BNo ratings yet
- NSG Man BulimiaDocument21 pagesNSG Man BulimiaMelodia Turqueza GandezaNo ratings yet
- Temazepam (Restoril)Document1 pageTemazepam (Restoril)E100% (2)
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- Discharge PlanDocument4 pagesDischarge PlanVillanueva NiñaNo ratings yet
- Generic Name 2Document2 pagesGeneric Name 2A 로마노 귀여운No ratings yet
- Case Report: Hirschsprung Disease: Aprilia Silambi, Tri Setyawati, Alfreth LangitanDocument5 pagesCase Report: Hirschsprung Disease: Aprilia Silambi, Tri Setyawati, Alfreth LangitanSabrina brinNo ratings yet
- Guide For The Care and Use of Laboratory Animals, 8th EditionDocument6 pagesGuide For The Care and Use of Laboratory Animals, 8th EditionmariaNo ratings yet
- 06 She Sop Consultation and Participation of WorkersDocument7 pages06 She Sop Consultation and Participation of WorkersHADWAN YUSOFNo ratings yet
- Occupational SafetyDocument29 pagesOccupational SafetyJoseph Nathan MarquezNo ratings yet
- Planning Theory-2008-Pløger-51-70 PDFDocument21 pagesPlanning Theory-2008-Pløger-51-70 PDFkhurshidqNo ratings yet
- DiverticulitisDocument27 pagesDiverticulitisMeri LismayantiNo ratings yet
- Basic Life Support CPR and First AidDocument112 pagesBasic Life Support CPR and First AidArthur LimNo ratings yet
- ESC May 2017Document16 pagesESC May 2017Gina DunnNo ratings yet
- Immune Thrombocytopenia (ITP) : Signs and SymptomsDocument35 pagesImmune Thrombocytopenia (ITP) : Signs and SymptomsRachmad SammuliaNo ratings yet
- Single-Knot Versus Multiple-Knot Technique of Perineal Repair - A Randomised Controlled TrialDocument8 pagesSingle-Knot Versus Multiple-Knot Technique of Perineal Repair - A Randomised Controlled TrialDR RISKA WAHYUNo ratings yet
- 03 - KAMBO Guidelines & PreparationDocument2 pages03 - KAMBO Guidelines & PreparationDaša KuderNo ratings yet
- Laporan Aldp Tahun 2011 EnglishDocument24 pagesLaporan Aldp Tahun 2011 Englishaldp_jayapura071No ratings yet
- A Clinical Study On The Inguinal Hernia and Its Management in The General Surgical Practice at Tertiary Care HospitalDocument4 pagesA Clinical Study On The Inguinal Hernia and Its Management in The General Surgical Practice at Tertiary Care Hospitalmelon segerNo ratings yet
- IV TherapyDocument39 pagesIV TherapyRichard SiahaanNo ratings yet
- Fitrawati Arifuddin - How To Give An Oral Report To An RNDocument9 pagesFitrawati Arifuddin - How To Give An Oral Report To An RNfitrawatiarifuddinNo ratings yet
- BSS Igc I Notes FinalDocument82 pagesBSS Igc I Notes FinalAzad pravesh khanNo ratings yet
- Clinical JudgementDocument6 pagesClinical Judgementapi-664535132No ratings yet
- Medici Aromatic Plant in World PDFDocument459 pagesMedici Aromatic Plant in World PDFAbdelkader Mekhaldi100% (16)
- Barangay Annual Gender and Development PlanDocument8 pagesBarangay Annual Gender and Development PlanSam Lino DangpaNo ratings yet
- 2001 AnnualDocument78 pages2001 Annualrizaldi rahmatullahNo ratings yet
- Teen Sleep NeedsDocument10 pagesTeen Sleep Needsapi-533871700No ratings yet
- Basic Life Support QuestionsDocument3 pagesBasic Life Support QuestionsCee Sanchez100% (11)
- Reducing Teen Pregnancy PDFDocument10 pagesReducing Teen Pregnancy PDFnorjumawatonshahruddNo ratings yet
- Principles of Continuous Renal Replacement Therapy For AkiDocument43 pagesPrinciples of Continuous Renal Replacement Therapy For AkiFelicia Risca RyandiniNo ratings yet
- Shs-Als Module Pe-11Document7 pagesShs-Als Module Pe-11JA SonNo ratings yet
- Medical Clinics Accreditation StandardsDocument22 pagesMedical Clinics Accreditation Standardsshannel128No ratings yet
- Tittle of Proposal: An Assessment of Factors Contributing To Medicines and Pharmaceuticals Expiries at Zambia Medicines and Medical Supplies AgencyDocument23 pagesTittle of Proposal: An Assessment of Factors Contributing To Medicines and Pharmaceuticals Expiries at Zambia Medicines and Medical Supplies Agencyoliver Ng'andweNo ratings yet
- UTI (Urinary Tract Infection)Document9 pagesUTI (Urinary Tract Infection)Carson BirthNo ratings yet
- BARRETT, C. B. Measuring Food InsecurityDocument6 pagesBARRETT, C. B. Measuring Food InsecurityRodrigo Torres AlmeidaNo ratings yet