
Poshan SBCC Policy Brief PDF
Poshan SBCC Policy Brief PDF
You might also like
- MKA HHA Competency TestDocument14 pagesMKA HHA Competency TestMuhammad TaqwaNo ratings yet
- OLP CFPP The Contingency PlanDocument70 pagesOLP CFPP The Contingency PlanHerle Lobrino Barrios100% (2)
- 1.the Masala MarketDocument17 pages1.the Masala MarketShubham DeshmukhNo ratings yet
- Infidelity Treatment Patterns A Practice - Based Evidence Approach PDFDocument16 pagesInfidelity Treatment Patterns A Practice - Based Evidence Approach PDFJulián Alberto MatulevichNo ratings yet
- Chem 353 Pyruvate Dehydrogenase DeficiencyDocument24 pagesChem 353 Pyruvate Dehydrogenase Deficiencyapi-308400395No ratings yet
- Data Quality Management ModelDocument11 pagesData Quality Management ModelHanum PutericNo ratings yet
- Covid Pulse PH:: A Better Normal For The PoorDocument16 pagesCovid Pulse PH:: A Better Normal For The PoorngcnghgNo ratings yet
- "Working On What Matters": How USAID/LINKAGES Supports Indonesia's HIV ResponseDocument31 pages"Working On What Matters": How USAID/LINKAGES Supports Indonesia's HIV ResponseBlandina ReginaNo ratings yet
- IPPF Report 2017Document32 pagesIPPF Report 2017Justicia, Comunicación e IdentidadNo ratings yet
- Monitoring Equity in Access To Aids Treatment Programmes: A Review of Concepts, Models, Methods and IndicatorsDocument98 pagesMonitoring Equity in Access To Aids Treatment Programmes: A Review of Concepts, Models, Methods and IndicatorsCésar López GodoyNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding National Nutrition Mission (POSHAN ABHIYAAN) Among Mothers in Selected Community Area of Greater Noida, Uttar PradeshDocument5 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding National Nutrition Mission (POSHAN ABHIYAAN) Among Mothers in Selected Community Area of Greater Noida, Uttar PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Demistifying Community Mobilisation - A Strategy To Improving Maternal and Newborn HealthDocument0 pagesDemistifying Community Mobilisation - A Strategy To Improving Maternal and Newborn HealthGail HoadNo ratings yet
- NHSRC - Operational Guidelines On Maternal and Newborn HealthDocument46 pagesNHSRC - Operational Guidelines On Maternal and Newborn HealthNational Child Health Resource Centre (NCHRC)No ratings yet
- Assessing The Potential of Self Help Group Women.6Document8 pagesAssessing The Potential of Self Help Group Women.6Iris N MNo ratings yet
- Evidence Building SNEHA Dissemination 15th Nov. 2019Document2 pagesEvidence Building SNEHA Dissemination 15th Nov. 2019manali.9054No ratings yet
- EthiopiaDocument13 pagesEthiopiaabduse midwifNo ratings yet
- PIVOT 2019-2020 Impact ReportDocument29 pagesPIVOT 2019-2020 Impact ReportPivot100% (1)
- Community Score Card CareDocument4 pagesCommunity Score Card CarechatgptfnfNo ratings yet
- Ippf Annual Performance Report 2022 1Document72 pagesIppf Annual Performance Report 2022 1knowledgecitytogoNo ratings yet
- Good PaperDocument81 pagesGood PaperWoldegebrial ZeweldNo ratings yet
- Promoting Family Planning Uptake Through Enhanced UsapanDocument12 pagesPromoting Family Planning Uptake Through Enhanced UsapanBrgy. Sto. DomingoNo ratings yet
- 2020 Article 1426Document11 pages2020 Article 1426surya rakhmat hidayatNo ratings yet
- SNEHA Dissemination 2021 ReportDocument18 pagesSNEHA Dissemination 2021 Reportmanali.9054No ratings yet
- IEM - Impact Evaluation Matters - Enhanced Learning Through Involving Stakeholders in Oxfam S Impact StudiesDocument6 pagesIEM - Impact Evaluation Matters - Enhanced Learning Through Involving Stakeholders in Oxfam S Impact Studiessec336909No ratings yet
- Capstone Project MAPIT FlowchartDocument9 pagesCapstone Project MAPIT FlowchartSammy ChegeNo ratings yet
- Delivering More: Scaling Up Farm To School ProgramsDocument47 pagesDelivering More: Scaling Up Farm To School ProgramsCommunity Food SecurityNo ratings yet
- ESEAOR's Annual Report 2020Document46 pagesESEAOR's Annual Report 2020Susan HelinNo ratings yet
- IEC On Health InsuranceDocument12 pagesIEC On Health InsuranceJess MontesNo ratings yet
- Measuring Women's Empowerment in Agriculture: A Streamlined ApproachDocument52 pagesMeasuring Women's Empowerment in Agriculture: A Streamlined Approachemmanuel santoyo rioNo ratings yet
- AAP Survey 2021Document11 pagesAAP Survey 2021Hue LeNo ratings yet
- Human Resources For HealthDocument7 pagesHuman Resources For HealthclaramaharaniNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleFhasya Aditya PutraNo ratings yet
- Linking The National Social Register To The VulnerableDocument15 pagesLinking The National Social Register To The Vulnerablesani shituNo ratings yet
- Psychological Impact of Society On The Choice of Family Planning Method Used by Women in Fort Portal Regional Referral Hospital Fort Portal DistrDocument14 pagesPsychological Impact of Society On The Choice of Family Planning Method Used by Women in Fort Portal Regional Referral Hospital Fort Portal DistrKIU PUBLICATION AND EXTENSIONNo ratings yet
- Literature Review Ending Violence Against Women and GirlsDocument82 pagesLiterature Review Ending Violence Against Women and GirlsAstig KamaoNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- A Study To Evaluate The Effectiveness of Self Instructional Module SIM On Knowledge Regarding Uterine Prolapse Among ASHA Workers in Selected Health Centres of Sri Muktsar Sahib, PunjabDocument7 pagesA Study To Evaluate The Effectiveness of Self Instructional Module SIM On Knowledge Regarding Uterine Prolapse Among ASHA Workers in Selected Health Centres of Sri Muktsar Sahib, PunjabEditor IJTSRDNo ratings yet
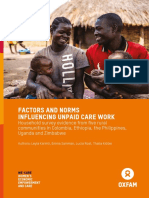
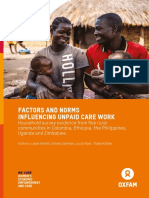
- Factors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweDocument64 pagesFactors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweDocument64 pagesFactors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweOxfam100% (1)
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Assessment of Knowledge Among ASHAs in The DeliverDocument7 pagesAssessment of Knowledge Among ASHAs in The DeliverShilpu RtwNo ratings yet
- Food and Nutrition ProgrammesDocument56 pagesFood and Nutrition ProgrammesDipesh UpadhyayNo ratings yet
- Cox's Bazar: at A GlanceDocument2 pagesCox's Bazar: at A GlanceSumon SwiftNo ratings yet
- Tools and Resources For Task TeamsDocument69 pagesTools and Resources For Task TeamsInayat KhanNo ratings yet
- Case Studies From NGO Community Across AsiaDocument131 pagesCase Studies From NGO Community Across AsiaAmmar100% (2)
- Case Study: Effects of A Media Campaign On Breastfeeding Behaviours in Sindh Province, PakistanDocument7 pagesCase Study: Effects of A Media Campaign On Breastfeeding Behaviours in Sindh Province, PakistanUmer NaseemNo ratings yet
- Actual Challenges of Mental Health in Indonesia: Urgency, UHS, Humanity, and Government CommitmentDocument3 pagesActual Challenges of Mental Health in Indonesia: Urgency, UHS, Humanity, and Government CommitmentSindy LarasatiNo ratings yet
- Stakeholder Analysis QuestionnaireDocument9 pagesStakeholder Analysis QuestionnaireTayyab AwanNo ratings yet
- Sanitary Project OverviewDocument21 pagesSanitary Project OverviewSharbeshexim InternationalNo ratings yet
- Community Based Maternal & Child Health Nutrition (MCHN) ProjectDocument104 pagesCommunity Based Maternal & Child Health Nutrition (MCHN) ProjectAshish GuptaNo ratings yet
- Assessing Child Nutrient Intakes Using A Tablet-Based 24-Hour Recall Tool in Rural ZambiaDocument14 pagesAssessing Child Nutrient Intakes Using A Tablet-Based 24-Hour Recall Tool in Rural Zambiashashi GourNo ratings yet
- Uganda Case Study FINALDocument85 pagesUganda Case Study FINALArka DasNo ratings yet
- Edited Research ProposalDocument20 pagesEdited Research ProposalNestoryNo ratings yet
- Livestock Production Extension: Issues, Case Studies and Policy OptionsDocument54 pagesLivestock Production Extension: Issues, Case Studies and Policy OptionsFalak Sher KhanNo ratings yet
- 08 SCOPE - Newsletter October 2018Document4 pages08 SCOPE - Newsletter October 2018Walney ManjateNo ratings yet
- Pnaec 421Document35 pagesPnaec 421Hamza MohamedNo ratings yet
- A Practical Guide For Network Managers: Linking Private Primary Health Care Networks To Sustainable Domestic FinancingDocument52 pagesA Practical Guide For Network Managers: Linking Private Primary Health Care Networks To Sustainable Domestic FinancingSigit SulistyoNo ratings yet
- UNICEF Report of Rapid Essential Health Service AssessmentDocument8 pagesUNICEF Report of Rapid Essential Health Service AssessmentputrilgNo ratings yet
- Introduction to Gender-Sensitive Social Protection Programming to Combat Rural Poverty: Why Is It Important and What Does It Mean? – Fao Technical Guide 1From EverandIntroduction to Gender-Sensitive Social Protection Programming to Combat Rural Poverty: Why Is It Important and What Does It Mean? – Fao Technical Guide 1No ratings yet
- Developing Gender-Sensitive Value Chains: A Guiding FrameworkFrom EverandDeveloping Gender-Sensitive Value Chains: A Guiding FrameworkNo ratings yet
- Grow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionDocument6 pagesGrow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionShubham DeshmukhNo ratings yet
- Grow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionDocument6 pagesGrow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionShubham DeshmukhNo ratings yet
- DM MICA+Brochure+tools+20210330Document18 pagesDM MICA+Brochure+tools+20210330Shubham DeshmukhNo ratings yet
- Are Farmer Producer Organizations A Boon To Farmers? The Evidence From Bihar, IndiaDocument16 pagesAre Farmer Producer Organizations A Boon To Farmers? The Evidence From Bihar, IndiaShubham DeshmukhNo ratings yet
- ET Medialabs-Sample-Insight - CardsDocument18 pagesET Medialabs-Sample-Insight - CardsShubham DeshmukhNo ratings yet
- Mapping Agriculture Investing in Africa: by Owens Otieno and Adedana AshebirDocument53 pagesMapping Agriculture Investing in Africa: by Owens Otieno and Adedana AshebirShubham DeshmukhNo ratings yet
- Forrester Total Economic Impact of Marketo EngageDocument21 pagesForrester Total Economic Impact of Marketo EngageShubham DeshmukhNo ratings yet
- Water and Women On A Tea Estate in Sri Lanka: Case 1Document10 pagesWater and Women On A Tea Estate in Sri Lanka: Case 1Shubham DeshmukhNo ratings yet
- Airbnb Book Review - Shubham Deshmukh - P38048Document12 pagesAirbnb Book Review - Shubham Deshmukh - P38048Shubham DeshmukhNo ratings yet
- Legal Environment of Business: Submitted To: Prof. Hardik Parikh Prof. Nishant SharmaDocument10 pagesLegal Environment of Business: Submitted To: Prof. Hardik Parikh Prof. Nishant SharmaShubham DeshmukhNo ratings yet
- Smart VillageDocument24 pagesSmart VillageDhruv100% (1)
- Anthropometry: Figure 01. Image of Vitruvian ManDocument3 pagesAnthropometry: Figure 01. Image of Vitruvian ManAlexandra HerreraNo ratings yet
- Cna Resume Template FreeDocument4 pagesCna Resume Template Freeafmrhbpxtgrdme100% (1)
- Reino FungiDocument1 pageReino FungiRuben Choquicota MaquitoNo ratings yet
- Intro To Virology ReviewerDocument14 pagesIntro To Virology ReviewerJilianne Sablot100% (2)
- Section I: Error Recognition: Choose The Word or Phrase Which Best Completes Each Blank Space in The Text!Document8 pagesSection I: Error Recognition: Choose The Word or Phrase Which Best Completes Each Blank Space in The Text!Levi KickermanNo ratings yet
- Guptautkarsh@dsnlu Ac inDocument2 pagesGuptautkarsh@dsnlu Ac inUTKARSH GUPTANo ratings yet
- Pharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientDocument8 pagesPharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientIndah PrihandiniNo ratings yet
- House Tree PersonDocument77 pagesHouse Tree PersonizyaNo ratings yet
- NCM 109 Pedia PreschoolDocument11 pagesNCM 109 Pedia PreschoolMantilla, Kristina Cassandra A.No ratings yet
- Vegan CompaniesDocument32 pagesVegan CompaniesLaura MelendezNo ratings yet
- Compliance Checklist For Garment IndustryDocument9 pagesCompliance Checklist For Garment Industryprasadbpotdar100% (1)
- TuberculosisDocument41 pagesTuberculosisMeena Devi100% (1)
- Combining CareersDocument1 pageCombining CareersManoj PurohitNo ratings yet
- MyocarditisDocument29 pagesMyocarditishastonniiNo ratings yet
- Aluminum Flux PasteDocument10 pagesAluminum Flux PasteMark Evan SalutinNo ratings yet
- Approved InstDocument368 pagesApproved InstSatish VermaNo ratings yet
- Malnutrition NCPDocument4 pagesMalnutrition NCPDenise Espinosa100% (3)
- Health Economic GrowthDocument25 pagesHealth Economic GrowthCarmen Ulloa MéndezNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- Provider Type Network Name Card Governorate CityDocument2,256 pagesProvider Type Network Name Card Governorate CityOsama Os OsNo ratings yet
- World Rankings ReportDocument5 pagesWorld Rankings Reporto3596989No ratings yet
- Personal Hygiene: Tve-ExploratoryDocument3 pagesPersonal Hygiene: Tve-ExploratoryPoseidon NipNo ratings yet
- SpecificationDocument56 pagesSpecificationIwan Herawan100% (1)
- DHA Part B Renal DialysisDocument28 pagesDHA Part B Renal DialysisKiran MauryaNo ratings yet





























































































Download as pdf or txt
You might also like
- MKA HHA Competency TestDocument14 pagesMKA HHA Competency TestMuhammad TaqwaNo ratings yet
- OLP CFPP The Contingency PlanDocument70 pagesOLP CFPP The Contingency PlanHerle Lobrino Barrios100% (2)
- 1.the Masala MarketDocument17 pages1.the Masala MarketShubham DeshmukhNo ratings yet
- Infidelity Treatment Patterns A Practice - Based Evidence Approach PDFDocument16 pagesInfidelity Treatment Patterns A Practice - Based Evidence Approach PDFJulián Alberto MatulevichNo ratings yet
- Chem 353 Pyruvate Dehydrogenase DeficiencyDocument24 pagesChem 353 Pyruvate Dehydrogenase Deficiencyapi-308400395No ratings yet
- Data Quality Management ModelDocument11 pagesData Quality Management ModelHanum PutericNo ratings yet
- Covid Pulse PH:: A Better Normal For The PoorDocument16 pagesCovid Pulse PH:: A Better Normal For The PoorngcnghgNo ratings yet
- "Working On What Matters": How USAID/LINKAGES Supports Indonesia's HIV ResponseDocument31 pages"Working On What Matters": How USAID/LINKAGES Supports Indonesia's HIV ResponseBlandina ReginaNo ratings yet
- IPPF Report 2017Document32 pagesIPPF Report 2017Justicia, Comunicación e IdentidadNo ratings yet
- Monitoring Equity in Access To Aids Treatment Programmes: A Review of Concepts, Models, Methods and IndicatorsDocument98 pagesMonitoring Equity in Access To Aids Treatment Programmes: A Review of Concepts, Models, Methods and IndicatorsCésar López GodoyNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding National Nutrition Mission (POSHAN ABHIYAAN) Among Mothers in Selected Community Area of Greater Noida, Uttar PradeshDocument5 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding National Nutrition Mission (POSHAN ABHIYAAN) Among Mothers in Selected Community Area of Greater Noida, Uttar PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Demistifying Community Mobilisation - A Strategy To Improving Maternal and Newborn HealthDocument0 pagesDemistifying Community Mobilisation - A Strategy To Improving Maternal and Newborn HealthGail HoadNo ratings yet
- NHSRC - Operational Guidelines On Maternal and Newborn HealthDocument46 pagesNHSRC - Operational Guidelines On Maternal and Newborn HealthNational Child Health Resource Centre (NCHRC)No ratings yet
- Assessing The Potential of Self Help Group Women.6Document8 pagesAssessing The Potential of Self Help Group Women.6Iris N MNo ratings yet
- Evidence Building SNEHA Dissemination 15th Nov. 2019Document2 pagesEvidence Building SNEHA Dissemination 15th Nov. 2019manali.9054No ratings yet
- EthiopiaDocument13 pagesEthiopiaabduse midwifNo ratings yet
- PIVOT 2019-2020 Impact ReportDocument29 pagesPIVOT 2019-2020 Impact ReportPivot100% (1)
- Community Score Card CareDocument4 pagesCommunity Score Card CarechatgptfnfNo ratings yet
- Ippf Annual Performance Report 2022 1Document72 pagesIppf Annual Performance Report 2022 1knowledgecitytogoNo ratings yet
- Good PaperDocument81 pagesGood PaperWoldegebrial ZeweldNo ratings yet
- Promoting Family Planning Uptake Through Enhanced UsapanDocument12 pagesPromoting Family Planning Uptake Through Enhanced UsapanBrgy. Sto. DomingoNo ratings yet
- 2020 Article 1426Document11 pages2020 Article 1426surya rakhmat hidayatNo ratings yet
- SNEHA Dissemination 2021 ReportDocument18 pagesSNEHA Dissemination 2021 Reportmanali.9054No ratings yet
- IEM - Impact Evaluation Matters - Enhanced Learning Through Involving Stakeholders in Oxfam S Impact StudiesDocument6 pagesIEM - Impact Evaluation Matters - Enhanced Learning Through Involving Stakeholders in Oxfam S Impact Studiessec336909No ratings yet
- Capstone Project MAPIT FlowchartDocument9 pagesCapstone Project MAPIT FlowchartSammy ChegeNo ratings yet
- Delivering More: Scaling Up Farm To School ProgramsDocument47 pagesDelivering More: Scaling Up Farm To School ProgramsCommunity Food SecurityNo ratings yet
- ESEAOR's Annual Report 2020Document46 pagesESEAOR's Annual Report 2020Susan HelinNo ratings yet
- IEC On Health InsuranceDocument12 pagesIEC On Health InsuranceJess MontesNo ratings yet
- Measuring Women's Empowerment in Agriculture: A Streamlined ApproachDocument52 pagesMeasuring Women's Empowerment in Agriculture: A Streamlined Approachemmanuel santoyo rioNo ratings yet
- AAP Survey 2021Document11 pagesAAP Survey 2021Hue LeNo ratings yet
- Human Resources For HealthDocument7 pagesHuman Resources For HealthclaramaharaniNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleFhasya Aditya PutraNo ratings yet
- Linking The National Social Register To The VulnerableDocument15 pagesLinking The National Social Register To The Vulnerablesani shituNo ratings yet
- Psychological Impact of Society On The Choice of Family Planning Method Used by Women in Fort Portal Regional Referral Hospital Fort Portal DistrDocument14 pagesPsychological Impact of Society On The Choice of Family Planning Method Used by Women in Fort Portal Regional Referral Hospital Fort Portal DistrKIU PUBLICATION AND EXTENSIONNo ratings yet
- Literature Review Ending Violence Against Women and GirlsDocument82 pagesLiterature Review Ending Violence Against Women and GirlsAstig KamaoNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- A Study To Evaluate The Effectiveness of Self Instructional Module SIM On Knowledge Regarding Uterine Prolapse Among ASHA Workers in Selected Health Centres of Sri Muktsar Sahib, PunjabDocument7 pagesA Study To Evaluate The Effectiveness of Self Instructional Module SIM On Knowledge Regarding Uterine Prolapse Among ASHA Workers in Selected Health Centres of Sri Muktsar Sahib, PunjabEditor IJTSRDNo ratings yet
- Factors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweDocument64 pagesFactors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweDocument64 pagesFactors and Norms Influencing Unpaid Care Work: Household Survey Evidence From Five Rural Communities in Colombia, Ethiopia, The Philippines, Uganda and ZimbabweOxfam100% (1)
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Factors and Norms Influencing Unpaid Care WorkDocument64 pagesFactors and Norms Influencing Unpaid Care WorkOxfamNo ratings yet
- Assessment of Knowledge Among ASHAs in The DeliverDocument7 pagesAssessment of Knowledge Among ASHAs in The DeliverShilpu RtwNo ratings yet
- Food and Nutrition ProgrammesDocument56 pagesFood and Nutrition ProgrammesDipesh UpadhyayNo ratings yet
- Cox's Bazar: at A GlanceDocument2 pagesCox's Bazar: at A GlanceSumon SwiftNo ratings yet
- Tools and Resources For Task TeamsDocument69 pagesTools and Resources For Task TeamsInayat KhanNo ratings yet
- Case Studies From NGO Community Across AsiaDocument131 pagesCase Studies From NGO Community Across AsiaAmmar100% (2)
- Case Study: Effects of A Media Campaign On Breastfeeding Behaviours in Sindh Province, PakistanDocument7 pagesCase Study: Effects of A Media Campaign On Breastfeeding Behaviours in Sindh Province, PakistanUmer NaseemNo ratings yet
- Actual Challenges of Mental Health in Indonesia: Urgency, UHS, Humanity, and Government CommitmentDocument3 pagesActual Challenges of Mental Health in Indonesia: Urgency, UHS, Humanity, and Government CommitmentSindy LarasatiNo ratings yet
- Stakeholder Analysis QuestionnaireDocument9 pagesStakeholder Analysis QuestionnaireTayyab AwanNo ratings yet
- Sanitary Project OverviewDocument21 pagesSanitary Project OverviewSharbeshexim InternationalNo ratings yet
- Community Based Maternal & Child Health Nutrition (MCHN) ProjectDocument104 pagesCommunity Based Maternal & Child Health Nutrition (MCHN) ProjectAshish GuptaNo ratings yet
- Assessing Child Nutrient Intakes Using A Tablet-Based 24-Hour Recall Tool in Rural ZambiaDocument14 pagesAssessing Child Nutrient Intakes Using A Tablet-Based 24-Hour Recall Tool in Rural Zambiashashi GourNo ratings yet
- Uganda Case Study FINALDocument85 pagesUganda Case Study FINALArka DasNo ratings yet
- Edited Research ProposalDocument20 pagesEdited Research ProposalNestoryNo ratings yet
- Livestock Production Extension: Issues, Case Studies and Policy OptionsDocument54 pagesLivestock Production Extension: Issues, Case Studies and Policy OptionsFalak Sher KhanNo ratings yet
- 08 SCOPE - Newsletter October 2018Document4 pages08 SCOPE - Newsletter October 2018Walney ManjateNo ratings yet
- Pnaec 421Document35 pagesPnaec 421Hamza MohamedNo ratings yet
- A Practical Guide For Network Managers: Linking Private Primary Health Care Networks To Sustainable Domestic FinancingDocument52 pagesA Practical Guide For Network Managers: Linking Private Primary Health Care Networks To Sustainable Domestic FinancingSigit SulistyoNo ratings yet
- UNICEF Report of Rapid Essential Health Service AssessmentDocument8 pagesUNICEF Report of Rapid Essential Health Service AssessmentputrilgNo ratings yet
- Introduction to Gender-Sensitive Social Protection Programming to Combat Rural Poverty: Why Is It Important and What Does It Mean? – Fao Technical Guide 1From EverandIntroduction to Gender-Sensitive Social Protection Programming to Combat Rural Poverty: Why Is It Important and What Does It Mean? – Fao Technical Guide 1No ratings yet
- Developing Gender-Sensitive Value Chains: A Guiding FrameworkFrom EverandDeveloping Gender-Sensitive Value Chains: A Guiding FrameworkNo ratings yet
- Grow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionDocument6 pagesGrow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionShubham DeshmukhNo ratings yet
- Grow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionDocument6 pagesGrow More, Grow Better.: Owner: Date of Applicability Scope Expected Next RevisionShubham DeshmukhNo ratings yet
- DM MICA+Brochure+tools+20210330Document18 pagesDM MICA+Brochure+tools+20210330Shubham DeshmukhNo ratings yet
- Are Farmer Producer Organizations A Boon To Farmers? The Evidence From Bihar, IndiaDocument16 pagesAre Farmer Producer Organizations A Boon To Farmers? The Evidence From Bihar, IndiaShubham DeshmukhNo ratings yet
- ET Medialabs-Sample-Insight - CardsDocument18 pagesET Medialabs-Sample-Insight - CardsShubham DeshmukhNo ratings yet
- Mapping Agriculture Investing in Africa: by Owens Otieno and Adedana AshebirDocument53 pagesMapping Agriculture Investing in Africa: by Owens Otieno and Adedana AshebirShubham DeshmukhNo ratings yet
- Forrester Total Economic Impact of Marketo EngageDocument21 pagesForrester Total Economic Impact of Marketo EngageShubham DeshmukhNo ratings yet
- Water and Women On A Tea Estate in Sri Lanka: Case 1Document10 pagesWater and Women On A Tea Estate in Sri Lanka: Case 1Shubham DeshmukhNo ratings yet
- Airbnb Book Review - Shubham Deshmukh - P38048Document12 pagesAirbnb Book Review - Shubham Deshmukh - P38048Shubham DeshmukhNo ratings yet
- Legal Environment of Business: Submitted To: Prof. Hardik Parikh Prof. Nishant SharmaDocument10 pagesLegal Environment of Business: Submitted To: Prof. Hardik Parikh Prof. Nishant SharmaShubham DeshmukhNo ratings yet
- Smart VillageDocument24 pagesSmart VillageDhruv100% (1)
- Anthropometry: Figure 01. Image of Vitruvian ManDocument3 pagesAnthropometry: Figure 01. Image of Vitruvian ManAlexandra HerreraNo ratings yet
- Cna Resume Template FreeDocument4 pagesCna Resume Template Freeafmrhbpxtgrdme100% (1)
- Reino FungiDocument1 pageReino FungiRuben Choquicota MaquitoNo ratings yet
- Intro To Virology ReviewerDocument14 pagesIntro To Virology ReviewerJilianne Sablot100% (2)
- Section I: Error Recognition: Choose The Word or Phrase Which Best Completes Each Blank Space in The Text!Document8 pagesSection I: Error Recognition: Choose The Word or Phrase Which Best Completes Each Blank Space in The Text!Levi KickermanNo ratings yet
- Guptautkarsh@dsnlu Ac inDocument2 pagesGuptautkarsh@dsnlu Ac inUTKARSH GUPTANo ratings yet
- Pharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientDocument8 pagesPharmacokinetic&Pharmacodynamics Mivacurium in Young Adult and Elderly PatientIndah PrihandiniNo ratings yet
- House Tree PersonDocument77 pagesHouse Tree PersonizyaNo ratings yet
- NCM 109 Pedia PreschoolDocument11 pagesNCM 109 Pedia PreschoolMantilla, Kristina Cassandra A.No ratings yet
- Vegan CompaniesDocument32 pagesVegan CompaniesLaura MelendezNo ratings yet
- Compliance Checklist For Garment IndustryDocument9 pagesCompliance Checklist For Garment Industryprasadbpotdar100% (1)
- TuberculosisDocument41 pagesTuberculosisMeena Devi100% (1)
- Combining CareersDocument1 pageCombining CareersManoj PurohitNo ratings yet
- MyocarditisDocument29 pagesMyocarditishastonniiNo ratings yet
- Aluminum Flux PasteDocument10 pagesAluminum Flux PasteMark Evan SalutinNo ratings yet
- Approved InstDocument368 pagesApproved InstSatish VermaNo ratings yet
- Malnutrition NCPDocument4 pagesMalnutrition NCPDenise Espinosa100% (3)
- Health Economic GrowthDocument25 pagesHealth Economic GrowthCarmen Ulloa MéndezNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- Provider Type Network Name Card Governorate CityDocument2,256 pagesProvider Type Network Name Card Governorate CityOsama Os OsNo ratings yet
- World Rankings ReportDocument5 pagesWorld Rankings Reporto3596989No ratings yet
- Personal Hygiene: Tve-ExploratoryDocument3 pagesPersonal Hygiene: Tve-ExploratoryPoseidon NipNo ratings yet
- SpecificationDocument56 pagesSpecificationIwan Herawan100% (1)
- DHA Part B Renal DialysisDocument28 pagesDHA Part B Renal DialysisKiran MauryaNo ratings yet