
DMAS 7a
DMAS 7a
You might also like
- Food Recall Plan Template FinalDocument19 pagesFood Recall Plan Template Finalsridharan100% (1)
- John Hancock Functional and Cognitive Screening Clinical Review Form v.12/23Document4 pagesJohn Hancock Functional and Cognitive Screening Clinical Review Form v.12/23michaelNo ratings yet
- ASAL Business Worksheet AnswersDocument53 pagesASAL Business Worksheet Answersdesrescott100% (1)
- IV-3 Assigmt - Module 2 Safety & MobilityDocument7 pagesIV-3 Assigmt - Module 2 Safety & MobilityKuldeep SinghNo ratings yet
- Dmas 99Document7 pagesDmas 99Billie_anderson2473No ratings yet
- Hss 1020 - Section 1Document20 pagesHss 1020 - Section 1api-266460789100% (1)
- SOW Dedicated TeamDocument6 pagesSOW Dedicated TeamНаталия ТкаченкоNo ratings yet
- Satellogic Albania Government Master Servicdes AgreementDocument33 pagesSatellogic Albania Government Master Servicdes AgreementTettsNo ratings yet
- Module IV: MUS Sampling - Factory Equipment Additions: RequirementsDocument2 pagesModule IV: MUS Sampling - Factory Equipment Additions: RequirementsMukh UbaidillahNo ratings yet
- Dmas 7Document1 pageDmas 7Billie_anderson2473No ratings yet
- Individual Vehicle Approval in EuropeDocument25 pagesIndividual Vehicle Approval in EuropeAmerican Import Agents AssociationNo ratings yet
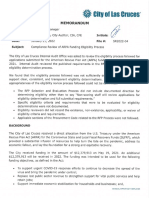
- Compliance Review of ARPA Eligibility ProcessDocument9 pagesCompliance Review of ARPA Eligibility ProcessMichael MNo ratings yet
- Sop On Cap - Dap - Edp Policy2Document14 pagesSop On Cap - Dap - Edp Policy2Namita Asthana100% (1)
- PHM Medisavers 2015 Insurance Policy SampleDocument24 pagesPHM Medisavers 2015 Insurance Policy SampleNazim Saleh100% (1)
- TrendCare User GuidelinesDocument11 pagesTrendCare User GuidelinesRidha SyahputraNo ratings yet
- Capital One - TemplateDocument6 pagesCapital One - TemplateClaire Marie ThomasNo ratings yet
- Indion Indro 401Document36 pagesIndion Indro 401maksudur4No ratings yet
- Document: Change Control Plan Owner: CIO Services Project OfficeDocument4 pagesDocument: Change Control Plan Owner: CIO Services Project OfficePhil WolfeNo ratings yet
- A Reply To Can Marxism Make Sense of CrimeDocument7 pagesA Reply To Can Marxism Make Sense of CrimeYakir SagalNo ratings yet
- Golden TamarawDocument1 pageGolden TamarawAdeza C. PlatonNo ratings yet
- Bill of LandingDocument2 pagesBill of LandingAndrés Mora EstevezNo ratings yet
- Harris 1958 Labor and Education in MozambiqueDocument28 pagesHarris 1958 Labor and Education in MozambiquejmmcvNo ratings yet
- Final Evaluation Report of AIDETDocument35 pagesFinal Evaluation Report of AIDETDianne Johnson Wojnicki100% (1)
- Agency-Level Controls Checklist: Agency/Project: Name Audit Period: January 1 To December 31, 20xxDocument15 pagesAgency-Level Controls Checklist: Agency/Project: Name Audit Period: January 1 To December 31, 20xxMJ BajaNo ratings yet
- CHCCOM003 - Application Learner.v8.3Document31 pagesCHCCOM003 - Application Learner.v8.3archerbray25No ratings yet
- Product and Service Quality DimensionsDocument19 pagesProduct and Service Quality DimensionsRavi Satyapal100% (1)
- Year Gap CertificateDocument2 pagesYear Gap CertificateTarikul IslamNo ratings yet
- IV-12 Assigmt - Module 12 Health ConditionsDocument11 pagesIV-12 Assigmt - Module 12 Health ConditionsDonnefya BravoNo ratings yet
- Controller Audit On LAFD Response TimesDocument46 pagesController Audit On LAFD Response TimesSouthern California Public RadioNo ratings yet
- BOG PPT Final Without Notes REVISEDDocument9 pagesBOG PPT Final Without Notes REVISEDWTXL ABC27No ratings yet
- ChildrenEduFacility TO GdsDocument9 pagesChildrenEduFacility TO GdsRenuka SalapakaNo ratings yet
- National Cadet Corps: Appendix A' (Revised 2013) Form IDocument8 pagesNational Cadet Corps: Appendix A' (Revised 2013) Form IAnkit AnandNo ratings yet
- RHWE REVISED Manual 10.07 PDFDocument168 pagesRHWE REVISED Manual 10.07 PDFShriram CollegeNo ratings yet
- ADN-I-033 Key Cost Management Principles Every Executive Must KnowDocument4 pagesADN-I-033 Key Cost Management Principles Every Executive Must Knowjamesdj88914No ratings yet
- Budget Worksheet 2Document6 pagesBudget Worksheet 2Ansh MaldeNo ratings yet
- What Is The Banquet?Document6 pagesWhat Is The Banquet?Johnson Macayan Fernández100% (1)
- Competency-Based Curriculum For HVAC TechnicansDocument3 pagesCompetency-Based Curriculum For HVAC Technicansfrederick beausoleilNo ratings yet
- Okd Form ADocument4 pagesOkd Form AAirene Mariel MagbanuaNo ratings yet
- Total Procurement and MBE/WBE Accomplishments This Reporting PeriodDocument5 pagesTotal Procurement and MBE/WBE Accomplishments This Reporting Periodanon-326932No ratings yet
- Job Description: Position: Position #: Title: Title Code: Reports To: Category: Classification: Status: QualificationsDocument5 pagesJob Description: Position: Position #: Title: Title Code: Reports To: Category: Classification: Status: Qualificationsarcmercer2012No ratings yet
- DMAS FormDocument3 pagesDMAS FormagalaboNo ratings yet
- Improved Family Friendly Measures PDFDocument37 pagesImproved Family Friendly Measures PDFgtecmaltaNo ratings yet
- Inspection Report: Care Home For Younger AdultsDocument39 pagesInspection Report: Care Home For Younger Adultsbhimrao_09No ratings yet
- Ok Sa Deped Form ADocument3 pagesOk Sa Deped Form APhoebe Sudweste Quitaneg100% (1)
- Subhash Kumar: Profile SummaryDocument3 pagesSubhash Kumar: Profile SummaryBigBoysChoice ShowNo ratings yet
- In-Service Education VirginiaDocument25 pagesIn-Service Education Virginiaapi-234162801No ratings yet
- 2984.May10.Care Officer (Higher).JD&PSDocument7 pages2984.May10.Care Officer (Higher).JD&PSJoyce AysonNo ratings yet
- Worker & Plan Details: C729 Home Health Care Services Personal Care PlanDocument5 pagesWorker & Plan Details: C729 Home Health Care Services Personal Care PlanDawn CasuncadNo ratings yet
- Daily Clinic Briefing MeetingDocument1 pageDaily Clinic Briefing MeetingTogu MarpaungNo ratings yet
- Vcm. Cdpap Agreement English 7.2022Document4 pagesVcm. Cdpap Agreement English 7.2022TayzonRamírezNo ratings yet
- Business Continuity Plan: UCLA HealthDocument28 pagesBusiness Continuity Plan: UCLA Healthmanar thaniNo ratings yet
- Eop 6Document4 pagesEop 6Wave TransportationNo ratings yet
- 4 - Unit Contingency PlansDocument25 pages4 - Unit Contingency PlansliviuNo ratings yet
- CaseNo.1 - NewCenturyHealthClinicDocument15 pagesCaseNo.1 - NewCenturyHealthClinicj0logz100% (2)
- 10adm 1 PDFDocument11 pages10adm 1 PDFHenry Jacob Baker JrNo ratings yet
- 10 0103 FillDocument2 pages10 0103 FillAlfazone360No ratings yet
- FTT QuestionsDocument7 pagesFTT QuestionsMavisNo ratings yet
- Ib 28Document24 pagesIb 28SunnyNo ratings yet
- 2020 Disability Services Metadata1 PDFDocument67 pages2020 Disability Services Metadata1 PDFmanuelNo ratings yet
- Cansas: Adaptation of CANSAS From 2005 The Royal College of PsychiatristsDocument2 pagesCansas: Adaptation of CANSAS From 2005 The Royal College of PsychiatristsJonayNo ratings yet
- Manulife Benefit SummaryDocument35 pagesManulife Benefit SummaryLDaggersonNo ratings yet
- RSP Form2 Subordinate Peer EvaluationDocument5 pagesRSP Form2 Subordinate Peer EvaluationXander 4thNo ratings yet
- Toolbox Talks: Weekly Tailgate Topic 12-26Document3 pagesToolbox Talks: Weekly Tailgate Topic 12-26Gersonn TaueliaNo ratings yet
- Guidelines For Setting Up ORM ServiceDocument15 pagesGuidelines For Setting Up ORM ServiceJohn Michael BantolinoNo ratings yet
- DUMALNEG Assessment Tool For PCFDocument17 pagesDUMALNEG Assessment Tool For PCFdumalneghrh 2017No ratings yet
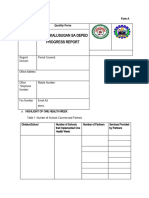
- Progress Report: Plan Alusugan Sa DepedDocument3 pagesProgress Report: Plan Alusugan Sa DepedRosalie Dela CruzNo ratings yet
- Neon Proc 004 v1Document11 pagesNeon Proc 004 v1SusieNo ratings yet
- EPSDT and The ID Waiver: Changes in Preauthorization of Children's ServicesDocument31 pagesEPSDT and The ID Waiver: Changes in Preauthorization of Children's ServicesBillie_anderson2473No ratings yet
- ISAR TheraConsult - 10-2010Document1 pageISAR TheraConsult - 10-2010Billie_anderson2473No ratings yet
- Cd-Pa Isar - 10-2010Document2 pagesCd-Pa Isar - 10-2010Billie_anderson2473No ratings yet
- VILLARTA V. CA (May 29, 1987) : FactsDocument28 pagesVILLARTA V. CA (May 29, 1987) : FactsDiorVelasquezNo ratings yet
- PWSI Customer Info Sheet - UpdatedDocument2 pagesPWSI Customer Info Sheet - UpdatedAbseiling BMSNo ratings yet
- Social CapitalismDocument2 pagesSocial CapitalismTestor AccountierNo ratings yet
- Project Report - FIM - SEY BANK FinalDocument11 pagesProject Report - FIM - SEY BANK Finalsethi.yogesh31No ratings yet
- Title Vii - Commercial Contracts For TransportationDocument4 pagesTitle Vii - Commercial Contracts For TransportationRubz JeanNo ratings yet
- M.B. Sanghi Vs HCP SynopsisDocument3 pagesM.B. Sanghi Vs HCP SynopsisArshaNo ratings yet
- Pleading - Exemption of PAO From Docket and Filing FeesDocument2 pagesPleading - Exemption of PAO From Docket and Filing FeesDon SalaNo ratings yet
- Banwa: Types of Social OrganizationDocument43 pagesBanwa: Types of Social OrganizationSamson Ebenga100% (1)
- Leverage Buyout Project2Document22 pagesLeverage Buyout Project2arnab_b87No ratings yet
- Rodrigo F. Gacos: BLK 14 Lot 21 Southville 5-A, Brgy. Langkiwa, City of Biñan, LagunaDocument4 pagesRodrigo F. Gacos: BLK 14 Lot 21 Southville 5-A, Brgy. Langkiwa, City of Biñan, LagunaRey ColomaNo ratings yet
- OD126068202277136000Document1 pageOD126068202277136000Amey BoradeNo ratings yet
- Mahatma Gandhi National Rural Employment Guarantee ActDocument16 pagesMahatma Gandhi National Rural Employment Guarantee ActVinod Thomas EfiNo ratings yet
- Sick Format-1-1 - PDFDocument7 pagesSick Format-1-1 - PDFNoah Esho100% (3)
- Cybercrime Prelim LecDocument5 pagesCybercrime Prelim LecGara Cap SorNo ratings yet
- 3-Admin Block Lighting LayoutDocument1 page3-Admin Block Lighting LayoutTafadzwa MurwiraNo ratings yet
- Telangana Eprocurement Portal - 3Document1 pageTelangana Eprocurement Portal - 3Mahesh GounikadiNo ratings yet
- RA 1405 Law On Bank Secrecy of Bank DepositsDocument24 pagesRA 1405 Law On Bank Secrecy of Bank DepositsJetJuárezNo ratings yet
- HCM in Islamic PerspectiveDocument16 pagesHCM in Islamic PerspectiveFendi RsvNo ratings yet
- Pierre Bourdieu, Religion, and Cultural ProductionDocument19 pagesPierre Bourdieu, Religion, and Cultural Productionmary20149No ratings yet
- Missoula Gas Tax Request LetterDocument2 pagesMissoula Gas Tax Request LetterOlivia IversonNo ratings yet
- 07 - Stability and ChangeDocument23 pages07 - Stability and ChangeFrancois Leann EvangelistaNo ratings yet
- Philippines TextDocument20 pagesPhilippines TextFrank OmarNo ratings yet
- Inequality and Poverty - A Short Critical Introduction PDFDocument92 pagesInequality and Poverty - A Short Critical Introduction PDFDrMladNo ratings yet
- 03AP Physics C - Gauss LawDocument14 pages03AP Physics C - Gauss LawrajeshNo ratings yet
- Israel and Palestine ConflictDocument44 pagesIsrael and Palestine ConflictJyoti Singh100% (1)





























































































Download as pdf or txt
You might also like
- Food Recall Plan Template FinalDocument19 pagesFood Recall Plan Template Finalsridharan100% (1)
- John Hancock Functional and Cognitive Screening Clinical Review Form v.12/23Document4 pagesJohn Hancock Functional and Cognitive Screening Clinical Review Form v.12/23michaelNo ratings yet
- ASAL Business Worksheet AnswersDocument53 pagesASAL Business Worksheet Answersdesrescott100% (1)
- IV-3 Assigmt - Module 2 Safety & MobilityDocument7 pagesIV-3 Assigmt - Module 2 Safety & MobilityKuldeep SinghNo ratings yet
- Dmas 99Document7 pagesDmas 99Billie_anderson2473No ratings yet
- Hss 1020 - Section 1Document20 pagesHss 1020 - Section 1api-266460789100% (1)
- SOW Dedicated TeamDocument6 pagesSOW Dedicated TeamНаталия ТкаченкоNo ratings yet
- Satellogic Albania Government Master Servicdes AgreementDocument33 pagesSatellogic Albania Government Master Servicdes AgreementTettsNo ratings yet
- Module IV: MUS Sampling - Factory Equipment Additions: RequirementsDocument2 pagesModule IV: MUS Sampling - Factory Equipment Additions: RequirementsMukh UbaidillahNo ratings yet
- Dmas 7Document1 pageDmas 7Billie_anderson2473No ratings yet
- Individual Vehicle Approval in EuropeDocument25 pagesIndividual Vehicle Approval in EuropeAmerican Import Agents AssociationNo ratings yet
- Compliance Review of ARPA Eligibility ProcessDocument9 pagesCompliance Review of ARPA Eligibility ProcessMichael MNo ratings yet
- Sop On Cap - Dap - Edp Policy2Document14 pagesSop On Cap - Dap - Edp Policy2Namita Asthana100% (1)
- PHM Medisavers 2015 Insurance Policy SampleDocument24 pagesPHM Medisavers 2015 Insurance Policy SampleNazim Saleh100% (1)
- TrendCare User GuidelinesDocument11 pagesTrendCare User GuidelinesRidha SyahputraNo ratings yet
- Capital One - TemplateDocument6 pagesCapital One - TemplateClaire Marie ThomasNo ratings yet
- Indion Indro 401Document36 pagesIndion Indro 401maksudur4No ratings yet
- Document: Change Control Plan Owner: CIO Services Project OfficeDocument4 pagesDocument: Change Control Plan Owner: CIO Services Project OfficePhil WolfeNo ratings yet
- A Reply To Can Marxism Make Sense of CrimeDocument7 pagesA Reply To Can Marxism Make Sense of CrimeYakir SagalNo ratings yet
- Golden TamarawDocument1 pageGolden TamarawAdeza C. PlatonNo ratings yet
- Bill of LandingDocument2 pagesBill of LandingAndrés Mora EstevezNo ratings yet
- Harris 1958 Labor and Education in MozambiqueDocument28 pagesHarris 1958 Labor and Education in MozambiquejmmcvNo ratings yet
- Final Evaluation Report of AIDETDocument35 pagesFinal Evaluation Report of AIDETDianne Johnson Wojnicki100% (1)
- Agency-Level Controls Checklist: Agency/Project: Name Audit Period: January 1 To December 31, 20xxDocument15 pagesAgency-Level Controls Checklist: Agency/Project: Name Audit Period: January 1 To December 31, 20xxMJ BajaNo ratings yet
- CHCCOM003 - Application Learner.v8.3Document31 pagesCHCCOM003 - Application Learner.v8.3archerbray25No ratings yet
- Product and Service Quality DimensionsDocument19 pagesProduct and Service Quality DimensionsRavi Satyapal100% (1)
- Year Gap CertificateDocument2 pagesYear Gap CertificateTarikul IslamNo ratings yet
- IV-12 Assigmt - Module 12 Health ConditionsDocument11 pagesIV-12 Assigmt - Module 12 Health ConditionsDonnefya BravoNo ratings yet
- Controller Audit On LAFD Response TimesDocument46 pagesController Audit On LAFD Response TimesSouthern California Public RadioNo ratings yet
- BOG PPT Final Without Notes REVISEDDocument9 pagesBOG PPT Final Without Notes REVISEDWTXL ABC27No ratings yet
- ChildrenEduFacility TO GdsDocument9 pagesChildrenEduFacility TO GdsRenuka SalapakaNo ratings yet
- National Cadet Corps: Appendix A' (Revised 2013) Form IDocument8 pagesNational Cadet Corps: Appendix A' (Revised 2013) Form IAnkit AnandNo ratings yet
- RHWE REVISED Manual 10.07 PDFDocument168 pagesRHWE REVISED Manual 10.07 PDFShriram CollegeNo ratings yet
- ADN-I-033 Key Cost Management Principles Every Executive Must KnowDocument4 pagesADN-I-033 Key Cost Management Principles Every Executive Must Knowjamesdj88914No ratings yet
- Budget Worksheet 2Document6 pagesBudget Worksheet 2Ansh MaldeNo ratings yet
- What Is The Banquet?Document6 pagesWhat Is The Banquet?Johnson Macayan Fernández100% (1)
- Competency-Based Curriculum For HVAC TechnicansDocument3 pagesCompetency-Based Curriculum For HVAC Technicansfrederick beausoleilNo ratings yet
- Okd Form ADocument4 pagesOkd Form AAirene Mariel MagbanuaNo ratings yet
- Total Procurement and MBE/WBE Accomplishments This Reporting PeriodDocument5 pagesTotal Procurement and MBE/WBE Accomplishments This Reporting Periodanon-326932No ratings yet
- Job Description: Position: Position #: Title: Title Code: Reports To: Category: Classification: Status: QualificationsDocument5 pagesJob Description: Position: Position #: Title: Title Code: Reports To: Category: Classification: Status: Qualificationsarcmercer2012No ratings yet
- DMAS FormDocument3 pagesDMAS FormagalaboNo ratings yet
- Improved Family Friendly Measures PDFDocument37 pagesImproved Family Friendly Measures PDFgtecmaltaNo ratings yet
- Inspection Report: Care Home For Younger AdultsDocument39 pagesInspection Report: Care Home For Younger Adultsbhimrao_09No ratings yet
- Ok Sa Deped Form ADocument3 pagesOk Sa Deped Form APhoebe Sudweste Quitaneg100% (1)
- Subhash Kumar: Profile SummaryDocument3 pagesSubhash Kumar: Profile SummaryBigBoysChoice ShowNo ratings yet
- In-Service Education VirginiaDocument25 pagesIn-Service Education Virginiaapi-234162801No ratings yet
- 2984.May10.Care Officer (Higher).JD&PSDocument7 pages2984.May10.Care Officer (Higher).JD&PSJoyce AysonNo ratings yet
- Worker & Plan Details: C729 Home Health Care Services Personal Care PlanDocument5 pagesWorker & Plan Details: C729 Home Health Care Services Personal Care PlanDawn CasuncadNo ratings yet
- Daily Clinic Briefing MeetingDocument1 pageDaily Clinic Briefing MeetingTogu MarpaungNo ratings yet
- Vcm. Cdpap Agreement English 7.2022Document4 pagesVcm. Cdpap Agreement English 7.2022TayzonRamírezNo ratings yet
- Business Continuity Plan: UCLA HealthDocument28 pagesBusiness Continuity Plan: UCLA Healthmanar thaniNo ratings yet
- Eop 6Document4 pagesEop 6Wave TransportationNo ratings yet
- 4 - Unit Contingency PlansDocument25 pages4 - Unit Contingency PlansliviuNo ratings yet
- CaseNo.1 - NewCenturyHealthClinicDocument15 pagesCaseNo.1 - NewCenturyHealthClinicj0logz100% (2)
- 10adm 1 PDFDocument11 pages10adm 1 PDFHenry Jacob Baker JrNo ratings yet
- 10 0103 FillDocument2 pages10 0103 FillAlfazone360No ratings yet
- FTT QuestionsDocument7 pagesFTT QuestionsMavisNo ratings yet
- Ib 28Document24 pagesIb 28SunnyNo ratings yet
- 2020 Disability Services Metadata1 PDFDocument67 pages2020 Disability Services Metadata1 PDFmanuelNo ratings yet
- Cansas: Adaptation of CANSAS From 2005 The Royal College of PsychiatristsDocument2 pagesCansas: Adaptation of CANSAS From 2005 The Royal College of PsychiatristsJonayNo ratings yet
- Manulife Benefit SummaryDocument35 pagesManulife Benefit SummaryLDaggersonNo ratings yet
- RSP Form2 Subordinate Peer EvaluationDocument5 pagesRSP Form2 Subordinate Peer EvaluationXander 4thNo ratings yet
- Toolbox Talks: Weekly Tailgate Topic 12-26Document3 pagesToolbox Talks: Weekly Tailgate Topic 12-26Gersonn TaueliaNo ratings yet
- Guidelines For Setting Up ORM ServiceDocument15 pagesGuidelines For Setting Up ORM ServiceJohn Michael BantolinoNo ratings yet
- DUMALNEG Assessment Tool For PCFDocument17 pagesDUMALNEG Assessment Tool For PCFdumalneghrh 2017No ratings yet
- Progress Report: Plan Alusugan Sa DepedDocument3 pagesProgress Report: Plan Alusugan Sa DepedRosalie Dela CruzNo ratings yet
- Neon Proc 004 v1Document11 pagesNeon Proc 004 v1SusieNo ratings yet
- EPSDT and The ID Waiver: Changes in Preauthorization of Children's ServicesDocument31 pagesEPSDT and The ID Waiver: Changes in Preauthorization of Children's ServicesBillie_anderson2473No ratings yet
- ISAR TheraConsult - 10-2010Document1 pageISAR TheraConsult - 10-2010Billie_anderson2473No ratings yet
- Cd-Pa Isar - 10-2010Document2 pagesCd-Pa Isar - 10-2010Billie_anderson2473No ratings yet
- VILLARTA V. CA (May 29, 1987) : FactsDocument28 pagesVILLARTA V. CA (May 29, 1987) : FactsDiorVelasquezNo ratings yet
- PWSI Customer Info Sheet - UpdatedDocument2 pagesPWSI Customer Info Sheet - UpdatedAbseiling BMSNo ratings yet
- Social CapitalismDocument2 pagesSocial CapitalismTestor AccountierNo ratings yet
- Project Report - FIM - SEY BANK FinalDocument11 pagesProject Report - FIM - SEY BANK Finalsethi.yogesh31No ratings yet
- Title Vii - Commercial Contracts For TransportationDocument4 pagesTitle Vii - Commercial Contracts For TransportationRubz JeanNo ratings yet
- M.B. Sanghi Vs HCP SynopsisDocument3 pagesM.B. Sanghi Vs HCP SynopsisArshaNo ratings yet
- Pleading - Exemption of PAO From Docket and Filing FeesDocument2 pagesPleading - Exemption of PAO From Docket and Filing FeesDon SalaNo ratings yet
- Banwa: Types of Social OrganizationDocument43 pagesBanwa: Types of Social OrganizationSamson Ebenga100% (1)
- Leverage Buyout Project2Document22 pagesLeverage Buyout Project2arnab_b87No ratings yet
- Rodrigo F. Gacos: BLK 14 Lot 21 Southville 5-A, Brgy. Langkiwa, City of Biñan, LagunaDocument4 pagesRodrigo F. Gacos: BLK 14 Lot 21 Southville 5-A, Brgy. Langkiwa, City of Biñan, LagunaRey ColomaNo ratings yet
- OD126068202277136000Document1 pageOD126068202277136000Amey BoradeNo ratings yet
- Mahatma Gandhi National Rural Employment Guarantee ActDocument16 pagesMahatma Gandhi National Rural Employment Guarantee ActVinod Thomas EfiNo ratings yet
- Sick Format-1-1 - PDFDocument7 pagesSick Format-1-1 - PDFNoah Esho100% (3)
- Cybercrime Prelim LecDocument5 pagesCybercrime Prelim LecGara Cap SorNo ratings yet
- 3-Admin Block Lighting LayoutDocument1 page3-Admin Block Lighting LayoutTafadzwa MurwiraNo ratings yet
- Telangana Eprocurement Portal - 3Document1 pageTelangana Eprocurement Portal - 3Mahesh GounikadiNo ratings yet
- RA 1405 Law On Bank Secrecy of Bank DepositsDocument24 pagesRA 1405 Law On Bank Secrecy of Bank DepositsJetJuárezNo ratings yet
- HCM in Islamic PerspectiveDocument16 pagesHCM in Islamic PerspectiveFendi RsvNo ratings yet
- Pierre Bourdieu, Religion, and Cultural ProductionDocument19 pagesPierre Bourdieu, Religion, and Cultural Productionmary20149No ratings yet
- Missoula Gas Tax Request LetterDocument2 pagesMissoula Gas Tax Request LetterOlivia IversonNo ratings yet
- 07 - Stability and ChangeDocument23 pages07 - Stability and ChangeFrancois Leann EvangelistaNo ratings yet
- Philippines TextDocument20 pagesPhilippines TextFrank OmarNo ratings yet
- Inequality and Poverty - A Short Critical Introduction PDFDocument92 pagesInequality and Poverty - A Short Critical Introduction PDFDrMladNo ratings yet
- 03AP Physics C - Gauss LawDocument14 pages03AP Physics C - Gauss LawrajeshNo ratings yet
- Israel and Palestine ConflictDocument44 pagesIsrael and Palestine ConflictJyoti Singh100% (1)