Download as pdf or txt
You might also like
- Learning To Use The Presbyopia Reduction ChartDocument3 pagesLearning To Use The Presbyopia Reduction Chart王唯任No ratings yet
- Moles Skin Cancer Aad-Body-Mole-Map PDFDocument2 pagesMoles Skin Cancer Aad-Body-Mole-Map PDFlunainisideNo ratings yet
- Life Science Grade 12 NSC November 2021 P1 and MemoDocument25 pagesLife Science Grade 12 NSC November 2021 P1 and Memo19nm9059No ratings yet
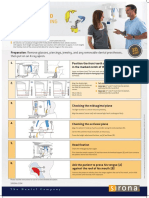
- Op XG 3D Patient PositioningDocument1 pageOp XG 3D Patient PositioningROGERQUIROZNo ratings yet
- 007-Limitations of PADocument18 pages007-Limitations of PAAyesha GeNo ratings yet
- Medical Report - Visual Disability: Section I - Report of ExaminationDocument4 pagesMedical Report - Visual Disability: Section I - Report of ExaminationNoel BrhaneNo ratings yet
- Module 5Document33 pagesModule 5Yeng LopezNo ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument23 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNo ratings yet
- Chapter 2 Mechanic PropDocument31 pagesChapter 2 Mechanic PropLuyến Phạm ThịNo ratings yet
- BlankDocument2 pagesBlankHafiz AzmiNo ratings yet
- Chapter 3 (MEC681) - MHI PDFDocument71 pagesChapter 3 (MEC681) - MHI PDFمحمد فائزNo ratings yet
- Ilovepdf Merged (2)Document116 pagesIlovepdf Merged (2)marvin.sorilla-18No ratings yet
- Mechanical Properties:: Issues To Address..Document32 pagesMechanical Properties:: Issues To Address..Anonymous 4fJtYPpvYuNo ratings yet
- Mechanical PropertiesDocument33 pagesMechanical PropertiesAstra BeckettNo ratings yet
- 5130 w06 QP 1Document16 pages5130 w06 QP 1rodel.verzosaNo ratings yet
- Service Manual: 8R11B ChassisDocument39 pagesService Manual: 8R11B ChassisC C I y T V G BNo ratings yet
- CH 06Document34 pagesCH 06Azoz BubiNo ratings yet
- Physics Experiment 1Document4 pagesPhysics Experiment 1aesthetic lyricsNo ratings yet
- Cr1 Re Severe Corneal UlcerDocument33 pagesCr1 Re Severe Corneal UlcerMeta An NazzilaNo ratings yet
- Lec4 PDFDocument3 pagesLec4 PDFteacher389No ratings yet
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocument22 pagesSurgeon Should Learn Not Just How To Operate But How To Create System of CareIrfanHadiWijayaNo ratings yet
- WK 5 Mechanical PropertiesDocument33 pagesWK 5 Mechanical Propertieszaid-ulau-806No ratings yet
- RMC1 - Metalliferous - Oct 2014 (F)Document10 pagesRMC1 - Metalliferous - Oct 2014 (F)Jaco RademeyerNo ratings yet
- 786 FullDocument2 pages786 Fullmicipsa AhwaouiNo ratings yet
- Diodes and Their Properties: Experiment 7Document2 pagesDiodes and Their Properties: Experiment 7Navaraj BaniyaNo ratings yet
- Chapter 6 CallisterDocument38 pagesChapter 6 CallisterJamaica VelascoNo ratings yet
- DE-13 - Quiz 17Document2 pagesDE-13 - Quiz 17Amit Kr GodaraNo ratings yet
- Fundamentals of Recording & Mounting Workshop Instructions April 21, 2016Document54 pagesFundamentals of Recording & Mounting Workshop Instructions April 21, 2016Syrk12No ratings yet
- 3rdqa Math8Document2 pages3rdqa Math8Cristy Jean Alimeos AlibangoNo ratings yet
- Mahadev IDocument22 pagesMahadev Ikabita basakNo ratings yet
- Skill Lab 1 Visual Acuity and Color Blind Test RevDocument4 pagesSkill Lab 1 Visual Acuity and Color Blind Test RevKaka MaulanaNo ratings yet
- 12Document1 page12دومبا فولسNo ratings yet
- Name: - LRNDocument2 pagesName: - LRNjrose fay amatNo ratings yet
- Laser Wavelength PracticalDocument4 pagesLaser Wavelength PracticalSekh AsifNo ratings yet
- Principles of Electronic Materials and Devices 4Th Edition Kasap Solutions Manual Full Chapter PDFDocument67 pagesPrinciples of Electronic Materials and Devices 4Th Edition Kasap Solutions Manual Full Chapter PDFreumetampoeqnb100% (13)
- L4 Mechanical PropertiesDocument41 pagesL4 Mechanical PropertiesHeamenth KumarNo ratings yet
- Double SlitDocument3 pagesDouble SlitVAIBHAV PRATAP SINGHNo ratings yet
- Lecture 5Document51 pagesLecture 5Abdul AhadNo ratings yet
- Chapter 1.4Document18 pagesChapter 1.4Chong Hou YINo ratings yet
- 10th Quiz Chap 14Document3 pages10th Quiz Chap 14Sherry DkNo ratings yet
- Chapter 2 Tension MembersDocument22 pagesChapter 2 Tension MembersMuayad AlzbediNo ratings yet
- Opthal Case StudyDocument8 pagesOpthal Case Studyyoutube contentNo ratings yet
- Inequality in Triangles ReportDocument54 pagesInequality in Triangles ReportLory Mae AlcosabaNo ratings yet
- Edited Session 3Document21 pagesEdited Session 3Chalerette MagaoayNo ratings yet
- LE40SMART04Document50 pagesLE40SMART04nanden.fer6973No ratings yet
- MGU Skill SheetDocument1 pageMGU Skill SheetMuhammed ElgasimNo ratings yet
- Grade 7 Activity 7Document2 pagesGrade 7 Activity 7Arian May MarcosNo ratings yet
- Electrowetting: Drop Profile Wetting Defects Wetting TransitionsDocument39 pagesElectrowetting: Drop Profile Wetting Defects Wetting TransitionsKarthik ManiNo ratings yet
- Service Manual: 6M61S ChassisDocument50 pagesService Manual: 6M61S Chassisroto44No ratings yet
- Cenmeccdb Activity 06 - Gulifardo Ezekiel A.Document5 pagesCenmeccdb Activity 06 - Gulifardo Ezekiel A.EzeKiel GulifardoNo ratings yet
- Torsion Part 1Document39 pagesTorsion Part 1Likha MontenegroNo ratings yet
- On Diode ApplicationsDocument13 pagesOn Diode ApplicationsBelen SeptianNo ratings yet
- Class Xi Practical (Slide Callipers)Document11 pagesClass Xi Practical (Slide Callipers)Spandan NandaNo ratings yet
- Section3 3modeling The Diode Foward Characteristic PackageDocument82 pagesSection3 3modeling The Diode Foward Characteristic Packageshubham ojhaNo ratings yet
- SMD ResistorsDocument13 pagesSMD ResistorsFodil ZouziNo ratings yet
- Induction Triaxial or 3D Tools: DefinitionsDocument28 pagesInduction Triaxial or 3D Tools: Definitionsved vyasNo ratings yet
- Optometry-to-the-Extreme-3.19.2024Document58 pagesOptometry-to-the-Extreme-3.19.2024Sadaf RahmanNo ratings yet
- Triangle Congruence M2Document29 pagesTriangle Congruence M2Joel BulawanNo ratings yet
- Vernier CalliperDocument23 pagesVernier CalliperminecrafygameNo ratings yet
- Technical Clarification (003) KOCDocument1 pageTechnical Clarification (003) KOCSubhajit BhattacharyaNo ratings yet
- Optimal Integration of GPS With Inertial SensorsDocument161 pagesOptimal Integration of GPS With Inertial Sensorsgabroo4No ratings yet
- Quick Reference CardDocument2 pagesQuick Reference Cardgabroo4100% (1)
- Ez LogbookDocument88 pagesEz Logbookgabroo4No ratings yet
- Mutual Fund Tracker IndiaDocument979 pagesMutual Fund Tracker Indiagabroo4No ratings yet
- Chapter 2-Minimum System, Software & Personal RequirementsDocument45 pagesChapter 2-Minimum System, Software & Personal Requirementsgabroo4No ratings yet
- Dgca DirectoryDocument3 pagesDgca Directorygabroo4No ratings yet
- 2013 Smart RK11 AutorefraDocument3 pages2013 Smart RK11 Autorefrajulio cesar duque riosNo ratings yet
- Stereoscopy and Stereoscopic ViewingDocument3 pagesStereoscopy and Stereoscopic ViewingEbenezer MatopeNo ratings yet
- ST 1klaDocument2 pagesST 1klaPandu PadmadisastraNo ratings yet
- A Critical Review On Li-Fi Technology and Its FutuDocument10 pagesA Critical Review On Li-Fi Technology and Its Futujsoham778No ratings yet
- Antenna Basics: Frequency Is One of The Most Important Concepts in The Universe and To Antenna Theory, WhichDocument39 pagesAntenna Basics: Frequency Is One of The Most Important Concepts in The Universe and To Antenna Theory, WhichCharbel RahmeNo ratings yet
- Class - 6 Subject: Science Chapter: How We See Things Topic: Why Are Shadows Formed? Differences Between Shadow and ReflectionDocument15 pagesClass - 6 Subject: Science Chapter: How We See Things Topic: Why Are Shadows Formed? Differences Between Shadow and ReflectionAbdullah SaleemNo ratings yet
- Mayas MaithilDocument16 pagesMayas MaithilMaYank VeRmaNo ratings yet
- Part Xxvii - Magnetic Fields & Forces-Set 2Document8 pagesPart Xxvii - Magnetic Fields & Forces-Set 2apostolos efstathiouNo ratings yet
- Chapter 3Document3 pagesChapter 3Vina PardedeNo ratings yet
- ManualDocument2 pagesManualgoma12345100% (1)
- BS8161 Lab Study MaterialDocument26 pagesBS8161 Lab Study MaterialGopi GanesanNo ratings yet
- Cony BioDocument12 pagesCony BioFrancis LoboNo ratings yet
- PDS 24Z2.1W 10X ExsdiDocument1 pagePDS 24Z2.1W 10X ExsdiboisolivierNo ratings yet
- Street LightngDocument4 pagesStreet Lightngasanithanair35No ratings yet
- Effects of Various Radiant Sources On Plant Growth (Part 2) : Shinji TAZAWADocument7 pagesEffects of Various Radiant Sources On Plant Growth (Part 2) : Shinji TAZAWAHammad KhanNo ratings yet
- Light Previous Years Shobhit NirwanDocument12 pagesLight Previous Years Shobhit NirwanPramod ChoudharyNo ratings yet
- CriminalisticDocument83 pagesCriminalisticGerald CauilanNo ratings yet
- Chapter 7Document18 pagesChapter 7roxy8marie8chanNo ratings yet
- Acdc Main Cat 2019 - 20 - Web 2Document1,046 pagesAcdc Main Cat 2019 - 20 - Web 2diewiesNo ratings yet
- Physics Syllabus TrackerDocument2 pagesPhysics Syllabus TrackerNilashri Ganguly IX A 22No ratings yet
- RFID Manual FullDocument57 pagesRFID Manual Fullmanoj yohanNo ratings yet
- Aipmt 2008 WithDocument35 pagesAipmt 2008 Withbhardwajshivam2No ratings yet
- Human Eye Complete - Watermarked PDFDocument13 pagesHuman Eye Complete - Watermarked PDFanandatulNo ratings yet
- Worksheet (Chapter 5)Document9 pagesWorksheet (Chapter 5)Poojal BatraNo ratings yet
- Metamaterials and Negative Refractive IndexDocument6 pagesMetamaterials and Negative Refractive IndexRohan KulkarniNo ratings yet
- Coplanar Waveguide - WikipediaDocument2 pagesCoplanar Waveguide - Wikipediaalvipin001No ratings yet
- Previewpdf Copy 4Document26 pagesPreviewpdf Copy 4TarekAlgamdiNo ratings yet
- 01-Multi Loose Tube CableDocument1 page01-Multi Loose Tube CableChairul Anam PurbaNo ratings yet
- Photography 1 Syllabus-1Document5 pagesPhotography 1 Syllabus-1api-293398131No ratings yet
- Digital Lens ZeissDocument16 pagesDigital Lens ZeissSe Jin KimNo ratings yet