Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Megacode Testing ScenariosDocument12 pagesMegacode Testing Scenariosmonsalg2502No ratings yet
- Electrophysiological Maneuvers For Arrhythmia Analysis-Cardiotext Publishing (2014)Document211 pagesElectrophysiological Maneuvers For Arrhythmia Analysis-Cardiotext Publishing (2014)Ali Uğur Soysal100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ECG Mastery Improving Your ECG Interpretation SkillsDocument23 pagesECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- Dysrhythmias Cheat SheetDocument2 pagesDysrhythmias Cheat SheetKatie Coughlan100% (2)
- ECG Interpretation Cheat SheetDocument14 pagesECG Interpretation Cheat Sheetrenet_alexandre75% (4)
- Checklist & Algoritma ACLSDocument16 pagesChecklist & Algoritma ACLSNadhif JovaldyNo ratings yet
- Jesse Felts PGY2, Not A CardiologistDocument43 pagesJesse Felts PGY2, Not A Cardiologistイオン天国No ratings yet
- Morning Rain by Jubing KristiantoDocument3 pagesMorning Rain by Jubing KristiantoChristopher Surya SuwitaNo ratings yet
- 2779 12418 1 PBDocument5 pages2779 12418 1 PBChristopher Surya SuwitaNo ratings yet
- APASL Hep B SlideDocument33 pagesAPASL Hep B SlideChristopher Surya SuwitaNo ratings yet
- Graves TXDocument43 pagesGraves TXChristopher Surya SuwitaNo ratings yet
- Nelfinavir As Potential Therapy For Systemic SclerosisDocument30 pagesNelfinavir As Potential Therapy For Systemic SclerosisChristopher Surya SuwitaNo ratings yet
- Dell'arte Schindler's ListDocument3 pagesDell'arte Schindler's ListChristopher Surya SuwitaNo ratings yet
- The Silver RainDocument10 pagesThe Silver RainChristopher Surya SuwitaNo ratings yet
- The Steroid Withdrawal Syndrome: A Review of The Implications, Etiology, and TreatmentsDocument5 pagesThe Steroid Withdrawal Syndrome: A Review of The Implications, Etiology, and TreatmentsChristopher Surya SuwitaNo ratings yet
- Ata 2017 Tiroid - PregnancyDocument75 pagesAta 2017 Tiroid - PregnancyheraniraniNo ratings yet
- Ibert Deux Interludes For Flute, Violin, and PianoDocument22 pagesIbert Deux Interludes For Flute, Violin, and PianoChristopher Surya Suwita100% (1)
- Ibert Deux Interludes For Flute, Violin, and PianoDocument22 pagesIbert Deux Interludes For Flute, Violin, and PianoChristopher Surya Suwita100% (1)
- Death CertificateDocument3 pagesDeath CertificateAllen Peter WeixlerNo ratings yet
- Chapter 125. CardioversionDocument21 pagesChapter 125. CardioversionZoe VelasquezNo ratings yet
- Cardiac MurmursDocument53 pagesCardiac MurmursdrgashokNo ratings yet
- Heartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaDocument31 pagesHeartbeat Disorders: by Aisha Sara Tasnim Physician: Dr. SsebulibaNinaNo ratings yet
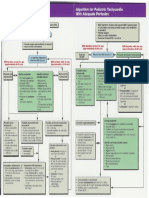
- Pediatric Tachycardia AlgorithmsDocument1 pagePediatric Tachycardia AlgorithmsGalih FatoniNo ratings yet
- Wa0006.Document1,362 pagesWa0006.HimanshuNo ratings yet
- First Semester 2020-2021 ECG Course Study Guide: University of The CordillerasDocument27 pagesFirst Semester 2020-2021 ECG Course Study Guide: University of The CordillerasGlory Anne Joy WillyNo ratings yet
- Textbook Instant Wisdom For Gps Pearls From All The Specialities 1St Edition Keith Hopcroft Ebook All Chapter PDFDocument53 pagesTextbook Instant Wisdom For Gps Pearls From All The Specialities 1St Edition Keith Hopcroft Ebook All Chapter PDFmoira.dunham823100% (13)
- Basics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyDocument206 pagesBasics of ECG: DR Subroto Mandal, MD, DM, DC Associate Professor, CardiologyRavi SharmaNo ratings yet
- Cardio Assignment On Electrocardiography (ECG)Document14 pagesCardio Assignment On Electrocardiography (ECG)s.sheikhh000No ratings yet
- Ocroteala Ionut Lucian Holter Pus Ieri 22.08.2023Document17 pagesOcroteala Ionut Lucian Holter Pus Ieri 22.08.2023Lototheone LotoNo ratings yet
- Comparison of PSD of Normal and Abnormal ECGsDocument5 pagesComparison of PSD of Normal and Abnormal ECGsEduardoHernandezNo ratings yet
- Chapter 34 Emergency Cardiovascular SystemDocument24 pagesChapter 34 Emergency Cardiovascular SystemDharlyn MungcalNo ratings yet
- ACLS Written 2006 Precourse Self AssessmentDocument14 pagesACLS Written 2006 Precourse Self AssessmentmonickamsNo ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet
- ACLS DrugDocument7 pagesACLS DrugPhongsatorn Thunin100% (1)
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Shock An OverviewDocument41 pagesShock An OverviewelaineNo ratings yet
- ECG in Emergency MedicineDocument228 pagesECG in Emergency MedicineBobbyGustafsonNo ratings yet
- Textbook of Anaesthesia For Postgraduates PDFDocument1,218 pagesTextbook of Anaesthesia For Postgraduates PDFMohammad HayajnehNo ratings yet
- Azure Specsheet Model w3dr01Document5 pagesAzure Specsheet Model w3dr01asdasd234234No ratings yet
- ACLS Simplify AlgorithmDocument6 pagesACLS Simplify AlgorithmKristine Monforte Coma UritaNo ratings yet
- Cara Membaca EKG Lengkap PAluDocument214 pagesCara Membaca EKG Lengkap PAluGiriNo ratings yet