
Jurnal
Jurnal
You might also like
- Chat GPTDocument13 pagesChat GPTsuly maniyahNo ratings yet
- Oral Notes Rupesh PillaiDocument172 pagesOral Notes Rupesh PillaiRachit100% (4)
- CribMaster 11 Features - User GuideDocument22 pagesCribMaster 11 Features - User GuidesalurkarNo ratings yet
- 1516-3180-spmj-133-04-00383 Azka PDFDocument1 page1516-3180-spmj-133-04-00383 Azka PDFagustiawan28No ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Aticulo EfficacyofRituximabvsTacrolimusinPediatric Corticosteroid-DependentNephroticSyndromeDocument8 pagesAticulo EfficacyofRituximabvsTacrolimusinPediatric Corticosteroid-DependentNephroticSyndromeJorge Luis Ramirez ImanNo ratings yet
- Capstone 2Document11 pagesCapstone 2mauriciosagredoNo ratings yet
- 2013 Burmester (TOFA Vs PLA)Document10 pages2013 Burmester (TOFA Vs PLA)Marcel JinihNo ratings yet
- Corticoides en NiñosDocument2 pagesCorticoides en NiñosDaniel Enrique Muro CabrejosNo ratings yet
- Treatment Outcomes in Patients Treated With Galcalizumab Vs Placebo - Headache 2020Document11 pagesTreatment Outcomes in Patients Treated With Galcalizumab Vs Placebo - Headache 2020Tiago Gomes de PaulaNo ratings yet
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDocument2 pagesProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNo ratings yet
- Ni 2016 (2) (CRE)Document10 pagesNi 2016 (2) (CRE)Nattawat TeerawattanapongNo ratings yet
- Efficacy and Safety of Medications For Antihistamie RefractoryDocument10 pagesEfficacy and Safety of Medications For Antihistamie Refractoryfatima amaliaNo ratings yet
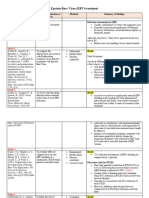
- Epstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of FindingsDocument3 pagesEpstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of Findingsapi-719803017No ratings yet
- Comment: Lancet Infect Dis 2014Document2 pagesComment: Lancet Infect Dis 2014Tony TuestaNo ratings yet
- Critically Appraised Topic Prophylactic Oral Antibiotics For Low-Risk Dog Bite WoundsDocument2 pagesCritically Appraised Topic Prophylactic Oral Antibiotics For Low-Risk Dog Bite Woundsyulei daiNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Tuberculosis Update Appendix d92Document11 pagesTuberculosis Update Appendix d92wosen wondNo ratings yet
- 1 s2.0 S0140673623020330 Main 2Document12 pages1 s2.0 S0140673623020330 Main 2Uriel EnriquezNo ratings yet
- Vietnamese J Eujim 2020 101060Document7 pagesVietnamese J Eujim 2020 101060Diah AlyaNo ratings yet
- Belayneh, 2017Document1 pageBelayneh, 2017Soraya Eugenia Morales LópezNo ratings yet
- Khan 2004Document8 pagesKhan 2004BENNY MAHENDRANo ratings yet
- Guselkumab in Patients With Active PsA Who Were Biologic-naive or Had Previously Received TNFα DISCOVER-1Document11 pagesGuselkumab in Patients With Active PsA Who Were Biologic-naive or Had Previously Received TNFα DISCOVER-1Edmundo RomanoNo ratings yet
- Methods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesDocument2 pagesMethods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesabbbabbbNo ratings yet
- ShingrixDocument6 pagesShingrixMarcus YoonNo ratings yet
- Keynote 048Document14 pagesKeynote 048brenomendespNo ratings yet
- Background: ISRCTN34716921Document5 pagesBackground: ISRCTN34716921Sav GaNo ratings yet
- 4-On 3-Off Journal Handout 3Document2 pages4-On 3-Off Journal Handout 3api-594366475No ratings yet
- Nsaids For Chronic Low Back Pain: Jama Clinical Evidence SynopsisDocument2 pagesNsaids For Chronic Low Back Pain: Jama Clinical Evidence SynopsistanyasisNo ratings yet
- Probiotics For The Prevention of Pediatric Antibiotic-Associated DiarrheaDocument7 pagesProbiotics For The Prevention of Pediatric Antibiotic-Associated DiarrheaJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- Corticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisDocument7 pagesCorticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisshiloinNo ratings yet
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaNo ratings yet
- Uptodate 2019 Nov 5 Ronthal MDocument15 pagesUptodate 2019 Nov 5 Ronthal MFernando SousaNo ratings yet
- Baloxavir Marboxil for Uncomplicated Influenza CAPSTONE 1 NEJM 2018Document11 pagesBaloxavir Marboxil for Uncomplicated Influenza CAPSTONE 1 NEJM 2018jotrembaNo ratings yet
- Qureshi 2005Document4 pagesQureshi 2005Susana BetancourtNo ratings yet
- Ahmad 2018Document14 pagesAhmad 2018Cristopher OchoaNo ratings yet
- PIIS0190962221020739Document2 pagesPIIS0190962221020739Roxanne KapNo ratings yet
- Evidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusDocument8 pagesEvidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusCharly EscobarNo ratings yet
- Bmjopen 2016 015233Document7 pagesBmjopen 2016 015233SEPTIANA SAPUTRINo ratings yet
- The Safety of Viscum Album L. in A Murine Model: A Reproductive Toxicity StudyDocument19 pagesThe Safety of Viscum Album L. in A Murine Model: A Reproductive Toxicity StudyCan BaldanNo ratings yet
- Efficacy of Rituximab Vs Tacrolimus in Pediatric Corticosteroid-Dependent Nephrotic Syndrome A Randomized Clinical TrialDocument16 pagesEfficacy of Rituximab Vs Tacrolimus in Pediatric Corticosteroid-Dependent Nephrotic Syndrome A Randomized Clinical Trialalicia keyNo ratings yet
- Nejm200103153441101 SLAMONDocument10 pagesNejm200103153441101 SLAMONFaiez LehyaniNo ratings yet
- CH 9.benefits of Resistance Testing - Antiretroviral Resistance in Clinical Practice - NCBI BookshelfDocument6 pagesCH 9.benefits of Resistance Testing - Antiretroviral Resistance in Clinical Practice - NCBI BookshelfntnquynhproNo ratings yet
- EsteroidesDocument10 pagesEsteroidesArturo Vargas AguilarNo ratings yet
- Dacosta JAMA 2016Document2 pagesDacosta JAMA 2016gck85fj8pnNo ratings yet
- Jamaoncology Vinayak 2019 Oi 190028Document9 pagesJamaoncology Vinayak 2019 Oi 190028Noema AmorochoNo ratings yet
- Parálisis de Bell - Tratamiento y Pronóstico en Adultos - UpToDateDocument13 pagesParálisis de Bell - Tratamiento y Pronóstico en Adultos - UpToDatejosebejarano12No ratings yet
- Inotozumab OzogamicinDocument14 pagesInotozumab OzogamicinTaraNo ratings yet
- BMJ j3887 FullDocument10 pagesBMJ j3887 FullRiri Maisytoh PutriNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaNo ratings yet
- 2015 Do Over The Counter Remedies Relieve Cough in Acute Upper Respiratory InfectionsDocument2 pages2015 Do Over The Counter Remedies Relieve Cough in Acute Upper Respiratory InfectionsDaniela Güiza ArgüelloNo ratings yet
- Monaleesa 2 - 2016Document11 pagesMonaleesa 2 - 2016Susanto SalimNo ratings yet
- 360-Article Text-1516-1-10-20211019Document4 pages360-Article Text-1516-1-10-20211019Ottofianus Alvedo Hewick KalangiNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- A Systematic Overview of Chemotherapy Effects inDocument22 pagesA Systematic Overview of Chemotherapy Effects inRutuja KuhikarNo ratings yet
- Dennis Slamon Ribociclib Plus Endocrine Therapy inDocument12 pagesDennis Slamon Ribociclib Plus Endocrine Therapy inandre.manzanoqNo ratings yet
- HPV Vaccine Programmes - Current Scenario and Recommendations in IndiaDocument3 pagesHPV Vaccine Programmes - Current Scenario and Recommendations in Indiash19782001No ratings yet
- 11-Year Study BRVDocument11 pages11-Year Study BRVAnshu RoyNo ratings yet
- Selected Topics: ToxicologyDocument9 pagesSelected Topics: Toxicologyzhin AristantiaNo ratings yet
- Intrathecal Ziconotide in The Treatment of Refractory Pain in Patients With Cancer or AIDSDocument8 pagesIntrathecal Ziconotide in The Treatment of Refractory Pain in Patients With Cancer or AIDSSérgio TavaresNo ratings yet
- LSHTM Research Online: Usage GuidlinesDocument11 pagesLSHTM Research Online: Usage GuidlinesnomdeplumNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Vertigo MeniereDocument5 pagesVertigo MeniereHamba AllahNo ratings yet
- Basic Life Support: DR - Dr. Zafrullah Khany Jasa, Span - KnaDocument47 pagesBasic Life Support: DR - Dr. Zafrullah Khany Jasa, Span - KnaHamba AllahNo ratings yet
- Assessing Stroke - Scores & Scales: DisclosuresDocument23 pagesAssessing Stroke - Scores & Scales: DisclosuresHamba AllahNo ratings yet
- Imsakiyah1440h - NADDocument1 pageImsakiyah1440h - NADHamba AllahNo ratings yet
- Kuliah Pakar Anemia in Pregnancy Dr. Ima IndirayaniDocument74 pagesKuliah Pakar Anemia in Pregnancy Dr. Ima IndirayaniHamba AllahNo ratings yet
- Essentials of Marketing Research 4th Edition Hair Test Bank DownloadDocument22 pagesEssentials of Marketing Research 4th Edition Hair Test Bank Downloademmanuelmabelnjt7nn100% (35)
- Visual IdentityDocument38 pagesVisual IdentityyannaNo ratings yet
- Lec04.UDP LinhdtDocument16 pagesLec04.UDP LinhdtHọc Sinh Nghiêm TúcNo ratings yet
- Criteria For Master Teacher: (With Additional Proposed Documents and The Specific Points As Support To Other Criteria)Document19 pagesCriteria For Master Teacher: (With Additional Proposed Documents and The Specific Points As Support To Other Criteria)Dennis ReyesNo ratings yet
- IOSA Guidance For Safety Monitoring Under COVID-19: Edition 5 - 05 May 2021Document18 pagesIOSA Guidance For Safety Monitoring Under COVID-19: Edition 5 - 05 May 2021Pilot Pilot380No ratings yet
- Anaesthetic Considerations in Polytrauma PatientsDocument8 pagesAnaesthetic Considerations in Polytrauma PatientsMileidys LopezNo ratings yet
- Q PapersDocument53 pagesQ PapersTanu RdNo ratings yet
- Silica & SilicatesDocument242 pagesSilica & SilicatesbabithyNo ratings yet
- BiodiversityR PDFDocument128 pagesBiodiversityR PDFEsteban VegaNo ratings yet
- Sheik Md. Maadul Hoque (ID 150201010035)Document49 pagesSheik Md. Maadul Hoque (ID 150201010035)Mizanur RahmanNo ratings yet
- Radio MirchiDocument7 pagesRadio MirchiRahul KasliwalNo ratings yet
- Development of The Chatbot As A Tool To Help The Service in The School SecretariatDocument7 pagesDevelopment of The Chatbot As A Tool To Help The Service in The School SecretariatIJAR JOURNALNo ratings yet
- Kirch GroupDocument13 pagesKirch GroupStacy ChackoNo ratings yet
- 01.1. RPS MSDM MM 2021Document10 pages01.1. RPS MSDM MM 2021anang setiawanNo ratings yet
- MatchmakerDocument43 pagesMatchmakerMatthew MckayNo ratings yet
- Display CAT PDFDocument2 pagesDisplay CAT PDFAndres130No ratings yet
- Chase: Eventhough This Case Shows How Campany Hires and Layoffs Strategy Would Work Best Due To Unstable Demand ForcestDocument3 pagesChase: Eventhough This Case Shows How Campany Hires and Layoffs Strategy Would Work Best Due To Unstable Demand ForcestCristhian ValverdeNo ratings yet
- Accounting Q&ADocument6 pagesAccounting Q&AIftikharNo ratings yet
- Topic 6:sustainability & Green EngineeringDocument5 pagesTopic 6:sustainability & Green EngineeringyanNo ratings yet
- Gyrator - Wikipedia PDFDocument44 pagesGyrator - Wikipedia PDFRishabh MishraNo ratings yet
- Vol.11 Issue 46 March 23-29, 2019Document32 pagesVol.11 Issue 46 March 23-29, 2019Thesouthasian TimesNo ratings yet
- Amendment of Information, Formal Vs SubstantialDocument2 pagesAmendment of Information, Formal Vs SubstantialNikkoCataquiz100% (3)
- Brochure Siemens Mobilett XP Digital Xray EBA AG2Document8 pagesBrochure Siemens Mobilett XP Digital Xray EBA AG2Alhasn AlmerabyNo ratings yet
- Intro To Molecular BioengineeringDocument12 pagesIntro To Molecular BioengineeringjoyeesufNo ratings yet
- Cummins ActuatorDocument4 pagesCummins ActuatorLaiq Zaman100% (1)
- Gender Informality and PovertyDocument15 pagesGender Informality and Povertygauravparmar1No ratings yet
- AdvertisingDocument16 pagesAdvertisingSun KambojNo ratings yet





























































































Download as pdf or txt
You might also like
- Chat GPTDocument13 pagesChat GPTsuly maniyahNo ratings yet
- Oral Notes Rupesh PillaiDocument172 pagesOral Notes Rupesh PillaiRachit100% (4)
- CribMaster 11 Features - User GuideDocument22 pagesCribMaster 11 Features - User GuidesalurkarNo ratings yet
- 1516-3180-spmj-133-04-00383 Azka PDFDocument1 page1516-3180-spmj-133-04-00383 Azka PDFagustiawan28No ratings yet
- Volume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1Document8 pagesVolume Probiotic Adjuvant Therapy Chronic Urticaria 4842allasp1fatima amaliaNo ratings yet
- Aticulo EfficacyofRituximabvsTacrolimusinPediatric Corticosteroid-DependentNephroticSyndromeDocument8 pagesAticulo EfficacyofRituximabvsTacrolimusinPediatric Corticosteroid-DependentNephroticSyndromeJorge Luis Ramirez ImanNo ratings yet
- Capstone 2Document11 pagesCapstone 2mauriciosagredoNo ratings yet
- 2013 Burmester (TOFA Vs PLA)Document10 pages2013 Burmester (TOFA Vs PLA)Marcel JinihNo ratings yet
- Corticoides en NiñosDocument2 pagesCorticoides en NiñosDaniel Enrique Muro CabrejosNo ratings yet
- Treatment Outcomes in Patients Treated With Galcalizumab Vs Placebo - Headache 2020Document11 pagesTreatment Outcomes in Patients Treated With Galcalizumab Vs Placebo - Headache 2020Tiago Gomes de PaulaNo ratings yet
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsDocument2 pagesProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LNo ratings yet
- Ni 2016 (2) (CRE)Document10 pagesNi 2016 (2) (CRE)Nattawat TeerawattanapongNo ratings yet
- Efficacy and Safety of Medications For Antihistamie RefractoryDocument10 pagesEfficacy and Safety of Medications For Antihistamie Refractoryfatima amaliaNo ratings yet
- Epstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of FindingsDocument3 pagesEpstein-Barr Virus (EBV) Treatment: Study - Authors & Date Purpose of Evaluation or Research Methods Summary of Findingsapi-719803017No ratings yet
- Comment: Lancet Infect Dis 2014Document2 pagesComment: Lancet Infect Dis 2014Tony TuestaNo ratings yet
- Critically Appraised Topic Prophylactic Oral Antibiotics For Low-Risk Dog Bite WoundsDocument2 pagesCritically Appraised Topic Prophylactic Oral Antibiotics For Low-Risk Dog Bite Woundsyulei daiNo ratings yet
- Colistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM EvidenceDocument27 pagesColistin Monotherapy Versus Combination Therapy For Carbapenem-Resistant Organisms NEJM Evidencerac.oncologyNo ratings yet
- Tuberculosis Update Appendix d92Document11 pagesTuberculosis Update Appendix d92wosen wondNo ratings yet
- 1 s2.0 S0140673623020330 Main 2Document12 pages1 s2.0 S0140673623020330 Main 2Uriel EnriquezNo ratings yet
- Vietnamese J Eujim 2020 101060Document7 pagesVietnamese J Eujim 2020 101060Diah AlyaNo ratings yet
- Belayneh, 2017Document1 pageBelayneh, 2017Soraya Eugenia Morales LópezNo ratings yet
- Khan 2004Document8 pagesKhan 2004BENNY MAHENDRANo ratings yet
- Guselkumab in Patients With Active PsA Who Were Biologic-naive or Had Previously Received TNFα DISCOVER-1Document11 pagesGuselkumab in Patients With Active PsA Who Were Biologic-naive or Had Previously Received TNFα DISCOVER-1Edmundo RomanoNo ratings yet
- Methods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesDocument2 pagesMethods: Jeremy M. Hernandez, MD, PHD Jonathan Sherbino, MD, Med Data SourcesabbbabbbNo ratings yet
- ShingrixDocument6 pagesShingrixMarcus YoonNo ratings yet
- Keynote 048Document14 pagesKeynote 048brenomendespNo ratings yet
- Background: ISRCTN34716921Document5 pagesBackground: ISRCTN34716921Sav GaNo ratings yet
- 4-On 3-Off Journal Handout 3Document2 pages4-On 3-Off Journal Handout 3api-594366475No ratings yet
- Nsaids For Chronic Low Back Pain: Jama Clinical Evidence SynopsisDocument2 pagesNsaids For Chronic Low Back Pain: Jama Clinical Evidence SynopsistanyasisNo ratings yet
- Probiotics For The Prevention of Pediatric Antibiotic-Associated DiarrheaDocument7 pagesProbiotics For The Prevention of Pediatric Antibiotic-Associated DiarrheaJUAN SEBASTIAN AVELLANEDA MARTINEZNo ratings yet
- Corticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisDocument7 pagesCorticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisshiloinNo ratings yet
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaNo ratings yet
- Uptodate 2019 Nov 5 Ronthal MDocument15 pagesUptodate 2019 Nov 5 Ronthal MFernando SousaNo ratings yet
- Baloxavir Marboxil for Uncomplicated Influenza CAPSTONE 1 NEJM 2018Document11 pagesBaloxavir Marboxil for Uncomplicated Influenza CAPSTONE 1 NEJM 2018jotrembaNo ratings yet
- Qureshi 2005Document4 pagesQureshi 2005Susana BetancourtNo ratings yet
- Ahmad 2018Document14 pagesAhmad 2018Cristopher OchoaNo ratings yet
- PIIS0190962221020739Document2 pagesPIIS0190962221020739Roxanne KapNo ratings yet
- Evidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusDocument8 pagesEvidence-Based Treatmentsin Pemphigusvulgaris Andpemphigus FoliaceusCharly EscobarNo ratings yet
- Bmjopen 2016 015233Document7 pagesBmjopen 2016 015233SEPTIANA SAPUTRINo ratings yet
- The Safety of Viscum Album L. in A Murine Model: A Reproductive Toxicity StudyDocument19 pagesThe Safety of Viscum Album L. in A Murine Model: A Reproductive Toxicity StudyCan BaldanNo ratings yet
- Efficacy of Rituximab Vs Tacrolimus in Pediatric Corticosteroid-Dependent Nephrotic Syndrome A Randomized Clinical TrialDocument16 pagesEfficacy of Rituximab Vs Tacrolimus in Pediatric Corticosteroid-Dependent Nephrotic Syndrome A Randomized Clinical Trialalicia keyNo ratings yet
- Nejm200103153441101 SLAMONDocument10 pagesNejm200103153441101 SLAMONFaiez LehyaniNo ratings yet
- CH 9.benefits of Resistance Testing - Antiretroviral Resistance in Clinical Practice - NCBI BookshelfDocument6 pagesCH 9.benefits of Resistance Testing - Antiretroviral Resistance in Clinical Practice - NCBI BookshelfntnquynhproNo ratings yet
- EsteroidesDocument10 pagesEsteroidesArturo Vargas AguilarNo ratings yet
- Dacosta JAMA 2016Document2 pagesDacosta JAMA 2016gck85fj8pnNo ratings yet
- Jamaoncology Vinayak 2019 Oi 190028Document9 pagesJamaoncology Vinayak 2019 Oi 190028Noema AmorochoNo ratings yet
- Parálisis de Bell - Tratamiento y Pronóstico en Adultos - UpToDateDocument13 pagesParálisis de Bell - Tratamiento y Pronóstico en Adultos - UpToDatejosebejarano12No ratings yet
- Inotozumab OzogamicinDocument14 pagesInotozumab OzogamicinTaraNo ratings yet
- BMJ j3887 FullDocument10 pagesBMJ j3887 FullRiri Maisytoh PutriNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaNo ratings yet
- 2015 Do Over The Counter Remedies Relieve Cough in Acute Upper Respiratory InfectionsDocument2 pages2015 Do Over The Counter Remedies Relieve Cough in Acute Upper Respiratory InfectionsDaniela Güiza ArgüelloNo ratings yet
- Monaleesa 2 - 2016Document11 pagesMonaleesa 2 - 2016Susanto SalimNo ratings yet
- 360-Article Text-1516-1-10-20211019Document4 pages360-Article Text-1516-1-10-20211019Ottofianus Alvedo Hewick KalangiNo ratings yet
- Tugas RCT SenaDocument10 pagesTugas RCT SenaArfad El HabibieNo ratings yet
- A Systematic Overview of Chemotherapy Effects inDocument22 pagesA Systematic Overview of Chemotherapy Effects inRutuja KuhikarNo ratings yet
- Dennis Slamon Ribociclib Plus Endocrine Therapy inDocument12 pagesDennis Slamon Ribociclib Plus Endocrine Therapy inandre.manzanoqNo ratings yet
- HPV Vaccine Programmes - Current Scenario and Recommendations in IndiaDocument3 pagesHPV Vaccine Programmes - Current Scenario and Recommendations in Indiash19782001No ratings yet
- 11-Year Study BRVDocument11 pages11-Year Study BRVAnshu RoyNo ratings yet
- Selected Topics: ToxicologyDocument9 pagesSelected Topics: Toxicologyzhin AristantiaNo ratings yet
- Intrathecal Ziconotide in The Treatment of Refractory Pain in Patients With Cancer or AIDSDocument8 pagesIntrathecal Ziconotide in The Treatment of Refractory Pain in Patients With Cancer or AIDSSérgio TavaresNo ratings yet
- LSHTM Research Online: Usage GuidlinesDocument11 pagesLSHTM Research Online: Usage GuidlinesnomdeplumNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Top Trials in Gastroenterology & HepatologyFrom EverandTop Trials in Gastroenterology & HepatologyRating: 4.5 out of 5 stars4.5/5 (7)
- Vertigo MeniereDocument5 pagesVertigo MeniereHamba AllahNo ratings yet
- Basic Life Support: DR - Dr. Zafrullah Khany Jasa, Span - KnaDocument47 pagesBasic Life Support: DR - Dr. Zafrullah Khany Jasa, Span - KnaHamba AllahNo ratings yet
- Assessing Stroke - Scores & Scales: DisclosuresDocument23 pagesAssessing Stroke - Scores & Scales: DisclosuresHamba AllahNo ratings yet
- Imsakiyah1440h - NADDocument1 pageImsakiyah1440h - NADHamba AllahNo ratings yet
- Kuliah Pakar Anemia in Pregnancy Dr. Ima IndirayaniDocument74 pagesKuliah Pakar Anemia in Pregnancy Dr. Ima IndirayaniHamba AllahNo ratings yet
- Essentials of Marketing Research 4th Edition Hair Test Bank DownloadDocument22 pagesEssentials of Marketing Research 4th Edition Hair Test Bank Downloademmanuelmabelnjt7nn100% (35)
- Visual IdentityDocument38 pagesVisual IdentityyannaNo ratings yet
- Lec04.UDP LinhdtDocument16 pagesLec04.UDP LinhdtHọc Sinh Nghiêm TúcNo ratings yet
- Criteria For Master Teacher: (With Additional Proposed Documents and The Specific Points As Support To Other Criteria)Document19 pagesCriteria For Master Teacher: (With Additional Proposed Documents and The Specific Points As Support To Other Criteria)Dennis ReyesNo ratings yet
- IOSA Guidance For Safety Monitoring Under COVID-19: Edition 5 - 05 May 2021Document18 pagesIOSA Guidance For Safety Monitoring Under COVID-19: Edition 5 - 05 May 2021Pilot Pilot380No ratings yet
- Anaesthetic Considerations in Polytrauma PatientsDocument8 pagesAnaesthetic Considerations in Polytrauma PatientsMileidys LopezNo ratings yet
- Q PapersDocument53 pagesQ PapersTanu RdNo ratings yet
- Silica & SilicatesDocument242 pagesSilica & SilicatesbabithyNo ratings yet
- BiodiversityR PDFDocument128 pagesBiodiversityR PDFEsteban VegaNo ratings yet
- Sheik Md. Maadul Hoque (ID 150201010035)Document49 pagesSheik Md. Maadul Hoque (ID 150201010035)Mizanur RahmanNo ratings yet
- Radio MirchiDocument7 pagesRadio MirchiRahul KasliwalNo ratings yet
- Development of The Chatbot As A Tool To Help The Service in The School SecretariatDocument7 pagesDevelopment of The Chatbot As A Tool To Help The Service in The School SecretariatIJAR JOURNALNo ratings yet
- Kirch GroupDocument13 pagesKirch GroupStacy ChackoNo ratings yet
- 01.1. RPS MSDM MM 2021Document10 pages01.1. RPS MSDM MM 2021anang setiawanNo ratings yet
- MatchmakerDocument43 pagesMatchmakerMatthew MckayNo ratings yet
- Display CAT PDFDocument2 pagesDisplay CAT PDFAndres130No ratings yet
- Chase: Eventhough This Case Shows How Campany Hires and Layoffs Strategy Would Work Best Due To Unstable Demand ForcestDocument3 pagesChase: Eventhough This Case Shows How Campany Hires and Layoffs Strategy Would Work Best Due To Unstable Demand ForcestCristhian ValverdeNo ratings yet
- Accounting Q&ADocument6 pagesAccounting Q&AIftikharNo ratings yet
- Topic 6:sustainability & Green EngineeringDocument5 pagesTopic 6:sustainability & Green EngineeringyanNo ratings yet
- Gyrator - Wikipedia PDFDocument44 pagesGyrator - Wikipedia PDFRishabh MishraNo ratings yet
- Vol.11 Issue 46 March 23-29, 2019Document32 pagesVol.11 Issue 46 March 23-29, 2019Thesouthasian TimesNo ratings yet
- Amendment of Information, Formal Vs SubstantialDocument2 pagesAmendment of Information, Formal Vs SubstantialNikkoCataquiz100% (3)
- Brochure Siemens Mobilett XP Digital Xray EBA AG2Document8 pagesBrochure Siemens Mobilett XP Digital Xray EBA AG2Alhasn AlmerabyNo ratings yet
- Intro To Molecular BioengineeringDocument12 pagesIntro To Molecular BioengineeringjoyeesufNo ratings yet
- Cummins ActuatorDocument4 pagesCummins ActuatorLaiq Zaman100% (1)
- Gender Informality and PovertyDocument15 pagesGender Informality and Povertygauravparmar1No ratings yet
- AdvertisingDocument16 pagesAdvertisingSun KambojNo ratings yet