Download as docx, pdf, or txt
You might also like
- Exam Recalls - WordsologyDocument200 pagesExam Recalls - WordsologyShiv Prajapati83% (29)
- BOC 6th EdDocument79 pagesBOC 6th EdJuneyoa50% (10)
- MLS ASCP Exam Recall Questions Flashcards - QuizletDocument8 pagesMLS ASCP Exam Recall Questions Flashcards - Quizletyeliz kurt100% (3)
- Recalls ASCPDocument6 pagesRecalls ASCPAstrud Labrador100% (6)
- 150 Question Labce Quiz PDFDocument55 pages150 Question Labce Quiz PDFSalem Al-Ewaity100% (3)
- Ascp Recalls (File Grabbed)Document3 pagesAscp Recalls (File Grabbed)KL Suazo82% (11)
- Recall Ascp MirobiologyDocument7 pagesRecall Ascp MirobiologyNeal Allen100% (5)
- MLS ASCP Study Guide PDFDocument2 pagesMLS ASCP Study Guide PDFyowubhatori100% (3)
- ASCP BOC Study-Guide 5e ContentsDocument12 pagesASCP BOC Study-Guide 5e ContentsJoe Devola25% (4)
- January 2019 Acspi RecallsDocument2 pagesJanuary 2019 Acspi RecallsMykeeFonelleraTanduyan50% (2)
- ASCP Recalls 2017-2018 Flashcards - Quizlet - AmgadDocument80 pagesASCP Recalls 2017-2018 Flashcards - Quizlet - AmgadShiv Prajapati100% (17)
- TH ST NDDocument3 pagesTH ST NDDarlene Evangelista100% (2)
- Recalls. 2019 AscpDocument2 pagesRecalls. 2019 AscpJoanna Carel Lopez50% (2)
- ASCP ExamDocument10 pagesASCP Examnoone100% (4)
- ASCPi - Recall 4.Document287 pagesASCPi - Recall 4.Joan Ruvia Cabiscuelas AnisNo ratings yet
- Invalid Prolonged Results May Result When The Hematocrit Exceeds 55%Document15 pagesInvalid Prolonged Results May Result When The Hematocrit Exceeds 55%asma100% (3)
- Compre ASCP Part 2Document20 pagesCompre ASCP Part 2Deanna Lepon67% (3)
- Urinalysis and Body Fluids for Cls & MltFrom EverandUrinalysis and Body Fluids for Cls & MltNo ratings yet
- Ascp PointersDocument78 pagesAscp PointersNIMKY EMBER B. CLAMOHOY100% (14)
- Ascp PointersDocument78 pagesAscp Pointersbaihern2467% (3)
- ASCPDocument5 pagesASCPDjdjjd Siisus100% (3)
- ASCP ReviewerDocument8 pagesASCP Reviewergillian102290100% (7)
- As CP RecallDocument15 pagesAs CP RecallJoanna Carel Lopez100% (4)
- Ascp Boc QuestionsDocument5 pagesAscp Boc QuestionsZylene Betanio Gabriel100% (4)
- ASCP Recall (June 21 2017)Document8 pagesASCP Recall (June 21 2017)Joanna Carel Lopez100% (3)
- MLS-ASCPi-Recalls REVISEDDocument11 pagesMLS-ASCPi-Recalls REVISEDAstrud Labrador100% (3)
- MLS ASCPi Exam Content Guidlines 2019Document12 pagesMLS ASCPi Exam Content Guidlines 2019Islam100% (2)
- ASCP RecallsDocument4 pagesASCP RecallsKaren SantiagoNo ratings yet
- Medical Laboratory Technician: Passbooks Study GuideFrom EverandMedical Laboratory Technician: Passbooks Study GuideNo ratings yet
- R6218017 Kushvitha 131119222310 PDFDocument7 pagesR6218017 Kushvitha 131119222310 PDFRohini BathulaNo ratings yet
- PallorDocument16 pagesPallorManal AlQuaimi100% (1)
- Recalls WordsologyDocument25 pagesRecalls WordsologyJie Fuentes91% (11)
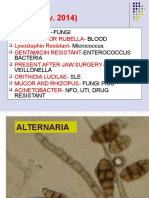
- Recall (Nov. 2014) : - Fungi Blood Micrococcus - Enterococcus Bacteria Veillonella SLE Fungi Pics Nfo, Uti, Drug ResistantDocument79 pagesRecall (Nov. 2014) : - Fungi Blood Micrococcus - Enterococcus Bacteria Veillonella SLE Fungi Pics Nfo, Uti, Drug Resistantpcyeol75% (4)
- Ascpi (MLS) Study Guide: Cushing's DiseaseDocument2 pagesAscpi (MLS) Study Guide: Cushing's DiseaseCatherine Nicolas100% (5)
- Ascp Pointers MicroDocument73 pagesAscp Pointers Microraica56_362842087100% (6)
- ASCP Recalls 5Document9 pagesASCP Recalls 5Cristina Vergel De DiosNo ratings yet
- RecallsDocument1 pageRecallsTinay100% (1)
- ASCP Recall 30-08-2018 Sujan BarmanDocument1 pageASCP Recall 30-08-2018 Sujan BarmanLou Joseff Milan BaluyotNo ratings yet
- Recall Ascp MirobiologyDocument7 pagesRecall Ascp MirobiologyJie Fuentes80% (5)
- Recall 3Document22 pagesRecall 3Christine Rodriguez-Guerrero100% (4)
- Immuno For ASCP ReviewDocument25 pagesImmuno For ASCP ReviewWl SorianoNo ratings yet
- ASCP Questions (Autosaved) - 1Document56 pagesASCP Questions (Autosaved) - 1Glenn Perez100% (16)
- ASCPi Recall Questions Gio 1Document7 pagesASCPi Recall Questions Gio 1Joanna Carel Lopez100% (4)
- Ascp Boc QuestionsDocument4 pagesAscp Boc QuestionsRose jane Tambasen100% (1)
- AscpDocument1 pageAscpGerald John Paz0% (5)
- Your BOC Exam: What You Need To Know To Be ReadyDocument35 pagesYour BOC Exam: What You Need To Know To Be ReadyDeanne Lamban100% (3)
- August 03 2017 Recalls Mls (Ascpi)Document6 pagesAugust 03 2017 Recalls Mls (Ascpi)Joanna Carel Lopez100% (3)
- ASCP Recalls As of August' 2013: Ionized CalciumDocument22 pagesASCP Recalls As of August' 2013: Ionized Calciumbaihern24No ratings yet
- Ascpi Recalls 2016Document9 pagesAscpi Recalls 2016Zylene Gabriel100% (1)
- Haematology Ascp RecallDocument7 pagesHaematology Ascp RecallMona AliNo ratings yet
- Hema PointrDocument4 pagesHema PointrLeonida DalugdogNo ratings yet
- Study Stack - M (ASCP) EXAM Table Review PDFDocument9 pagesStudy Stack - M (ASCP) EXAM Table Review PDF장주연100% (2)
- Virology ASCPDocument24 pagesVirology ASCP2131443No ratings yet
- Study Stack - MLT Table ReviewDocument3 pagesStudy Stack - MLT Table Review장주연100% (1)
- FEB 2017 RecallsDocument2 pagesFEB 2017 RecallsLucid LynxNo ratings yet
- Final Coaching Powerpoint Presentation by Ms. PiconesDocument458 pagesFinal Coaching Powerpoint Presentation by Ms. PiconesMark Justin Ocampo100% (2)
- Immunohematology HandoutDocument9 pagesImmunohematology Handoutmarkylopez2383% (6)
- Simulated No.1 General Rule:: ExceptDocument29 pagesSimulated No.1 General Rule:: ExceptJie FuentesNo ratings yet
- Blood Banking and Serology and Immunology - Refresher Exam With AnswersDocument8 pagesBlood Banking and Serology and Immunology - Refresher Exam With AnswersPaul Espinosa88% (26)
- March MTLE 2018 RecallsDocument6 pagesMarch MTLE 2018 RecallsJoan CañeteNo ratings yet
- 75 FullDocument8 pages75 FullFede0No ratings yet
- Physiology MCQ - BloodDocument4 pagesPhysiology MCQ - BloodMariam QureshiNo ratings yet
- Part 1 CQ HaematologyDocument17 pagesPart 1 CQ Haematologysayenshan0205No ratings yet
- CPG Management of ThalassaemiaDocument100 pagesCPG Management of Thalassaemiamrace_amNo ratings yet
- Who Diagnostic Criteria MyelofibrosisDocument1 pageWho Diagnostic Criteria Myelofibrosispieterinpretoria391No ratings yet
- Hema II Chapter 3 - Anemiarev - ATDocument154 pagesHema II Chapter 3 - Anemiarev - AThannigadah7No ratings yet
- Blood Physiology Lec1Document40 pagesBlood Physiology Lec1Sherwan R ShalNo ratings yet
- Case StudyDocument4 pagesCase StudyJAN MICAH A. CATEDRALNo ratings yet
- Bio-Rad A1C: For Hba, Hba and HBFDocument4 pagesBio-Rad A1C: For Hba, Hba and HBFsalamon2tNo ratings yet
- Alyana Ellaine S. Matias, MDDocument24 pagesAlyana Ellaine S. Matias, MDAlyana MatiasNo ratings yet
- Rabbithematology PDFDocument12 pagesRabbithematology PDFHuda HudaNo ratings yet
- Activity 6 Blood PhysiologyDocument7 pagesActivity 6 Blood PhysiologyRegz Acupanda100% (1)
- LAREPORTbionDocument4 pagesLAREPORTbionmelaniepearlNo ratings yet
- Transfusion in Animals PDFDocument8 pagesTransfusion in Animals PDFNejraNo ratings yet
- Laporan IKM KSM PK FEBRUARI 2022Document28 pagesLaporan IKM KSM PK FEBRUARI 2022Nur iffahNo ratings yet
- Microcytic Hypochromic AnaemiaDocument75 pagesMicrocytic Hypochromic AnaemiaNashita NowshinNo ratings yet
- Practical Hematology ManualDocument48 pagesPractical Hematology ManualHaael88No ratings yet
- Isabel M. BoydDocument4 pagesIsabel M. BoydKiran RagooNo ratings yet
- Hematology (CBC Profile) : MR. No. 21011543546 Lab No. Collection: Name: Gender: Male Age: 66 YearsDocument1 pageHematology (CBC Profile) : MR. No. 21011543546 Lab No. Collection: Name: Gender: Male Age: 66 YearsAsif ShahNo ratings yet
- MTAP ISBB - Sir JJ (Merged)Document9 pagesMTAP ISBB - Sir JJ (Merged)Nathan DrakeNo ratings yet
- Introduction To Hematology: What Is Blood ?Document5 pagesIntroduction To Hematology: What Is Blood ?Missy Vergara FloriaNo ratings yet
- Red Blood Cells/Red Blood Corpuscles (RBC) : ErythrocytesDocument6 pagesRed Blood Cells/Red Blood Corpuscles (RBC) : ErythrocytesDeep RoyNo ratings yet
- CPrecision July 23 PDFDocument6 pagesCPrecision July 23 PDFGeorjalyn Joy Quiachon (Jaja)No ratings yet
- Handbook of Pediatric Hematology and Oncology 3rd Edition 2021Document492 pagesHandbook of Pediatric Hematology and Oncology 3rd Edition 2021pgginecologiahospirioNo ratings yet
- My ThesisDocument10 pagesMy Thesishinduja reddipilliNo ratings yet
- Blood Immunology Module For 1st Year MBBS TT1912Document6 pagesBlood Immunology Module For 1st Year MBBS TT1912sabaNo ratings yet
- Biochemical Basis of AnaemiaDocument23 pagesBiochemical Basis of AnaemiaG M TAMIM CHOWDHURY789No ratings yet
- Jurnal Skripsi Evita OktaviaDocument10 pagesJurnal Skripsi Evita OktaviaandiniNo ratings yet