Download as pdf or txt
You might also like
- Ptosis Types & Clinical Features: Made By:-Amritansh PandeyDocument14 pagesPtosis Types & Clinical Features: Made By:-Amritansh PandeyalexNo ratings yet
- Orginal Healthy Aging Index 2014Document7 pagesOrginal Healthy Aging Index 2014bin linNo ratings yet
- Medicine American Journal of Hospice and PalliativeDocument6 pagesMedicine American Journal of Hospice and Palliativem1k0eNo ratings yet
- KeperawatanDocument8 pagesKeperawatanRyan FaisaldoNo ratings yet
- Cancers 08 00084Document10 pagesCancers 08 00084Benny Chris TantoNo ratings yet
- Autopsia e NeoplasiaDocument7 pagesAutopsia e NeoplasiaAMARO NUNES DUARTE NETONo ratings yet
- Original ArticleDocument7 pagesOriginal ArticleDain 2IronfootNo ratings yet
- Progressive Disease in PatientDocument9 pagesProgressive Disease in PatientDave LiuNo ratings yet
- Incidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorDocument6 pagesIncidence and Risk Factors For Ventilator Associated Pneumon 2007 RespiratorTomasNo ratings yet
- Terminal CancerDocument7 pagesTerminal Cancer김태준No ratings yet
- Cummings Et Al-2014-The Journal of PathologyDocument9 pagesCummings Et Al-2014-The Journal of Pathologyalicia1990No ratings yet
- Cancer Incidence Rate and Mortality Rate in Sickle Cell Disease Patients at Howard University Hospital: 1986-1995Document5 pagesCancer Incidence Rate and Mortality Rate in Sickle Cell Disease Patients at Howard University Hospital: 1986-1995Pengembangan Produk Persada HospitalNo ratings yet
- Probability Theory in The Diagnosis of Cushing's SyndromeDocument7 pagesProbability Theory in The Diagnosis of Cushing's SyndromeMuhammad Rafiq KNo ratings yet
- Cancer y Inmunosupresor en EtcDocument6 pagesCancer y Inmunosupresor en EtcANDONIS30No ratings yet
- (Sici) 1097-0142 (19961201) 78 11 2437 Aid-Cncr23 3.0.co 2-0Document6 pages(Sici) 1097-0142 (19961201) 78 11 2437 Aid-Cncr23 3.0.co 2-0Laura Cecilia Zárraga VargasNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofJoão AugustoNo ratings yet
- MC m6 Cancer+ovario+precozDocument9 pagesMC m6 Cancer+ovario+precozGrecia Castro CNo ratings yet
- Antipyretic Therapy in Critically Ill Septic Patients - A Systematic Review and Meta-AnalysisDocument8 pagesAntipyretic Therapy in Critically Ill Septic Patients - A Systematic Review and Meta-AnalysisKrutarth PatelNo ratings yet
- Research ArticleDocument9 pagesResearch ArticlemahadianismailnstNo ratings yet
- Current Trends in The Epidemiologyof Nosocomial Bloodstream Infectionsin Patients With Hematological Malignanciesand Solid Neoplasms in Hospitalsin The United StatesDocument8 pagesCurrent Trends in The Epidemiologyof Nosocomial Bloodstream Infectionsin Patients With Hematological Malignanciesand Solid Neoplasms in Hospitalsin The United StatespaulaveronicaNo ratings yet
- Comorbidity Profiles and Their Effect On Treatment Selection and Survival Among Patients With Lung CancerDocument10 pagesComorbidity Profiles and Their Effect On Treatment Selection and Survival Among Patients With Lung CancerdavidNo ratings yet
- Puo Paeds EgyptDocument7 pagesPuo Paeds EgyptFairuz binti Abdul RashidNo ratings yet
- Dokumen PDFDocument5 pagesDokumen PDFMacchiatoNo ratings yet
- Jurnal Observasional AnalitikDocument9 pagesJurnal Observasional AnalitikJethro BudimanNo ratings yet
- ARO SOCRE Predictor Mortalidad 2015Document13 pagesARO SOCRE Predictor Mortalidad 2015raul serranoNo ratings yet
- Genetic Risk, Adherence To A Healthy Lifestyle, and Coronary DiseaseDocument10 pagesGenetic Risk, Adherence To A Healthy Lifestyle, and Coronary DiseaseNurul Falah KalokoNo ratings yet
- A Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated With SurvivalDocument8 pagesA Prospective Study of Tuberculosis and Human Immunodeficiency Virus Infection Clinical Manifestations and Factors Associated With SurvivalAbrahamKatimeNo ratings yet
- Adults Hospitalized With Pneumonia in The United States: Incidence, Epidemiology, and MortalityDocument7 pagesAdults Hospitalized With Pneumonia in The United States: Incidence, Epidemiology, and Mortality6p5v5dvpffNo ratings yet
- Acr2 3 209Document12 pagesAcr2 3 209mirandanasution1209No ratings yet
- Validation of A Combined Comorbidity IndexDocument7 pagesValidation of A Combined Comorbidity IndexmarliivitorinoNo ratings yet
- Pi Is 0140673620326568Document12 pagesPi Is 0140673620326568Mada Dwi HariNo ratings yet
- Neuro-Oncology: Pregnancy and Glial Brain TumorsDocument6 pagesNeuro-Oncology: Pregnancy and Glial Brain Tumorsppds ui jan2017No ratings yet
- Glycemic Control and Radiographic Manifestations of Tuberculosis in Diabetic PatientsDocument17 pagesGlycemic Control and Radiographic Manifestations of Tuberculosis in Diabetic PatientsGlenda B AjilaNo ratings yet
- Survival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorDocument10 pagesSurvival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorGetachew GemedaNo ratings yet
- Influenza Vaccination and Mortality Differentiating Vaccine Effects From BiasDocument8 pagesInfluenza Vaccination and Mortality Differentiating Vaccine Effects From BiasadrianaNo ratings yet
- American Journal of EpidemiologyDocument9 pagesAmerican Journal of Epidemiologyselva awandariNo ratings yet
- The Clinical Outcomes and Predictive Factors For.24Document5 pagesThe Clinical Outcomes and Predictive Factors For.24KeziaNo ratings yet
- Idiopathic First Seizure in Adult Life: Who Be Treated?: ShouldDocument4 pagesIdiopathic First Seizure in Adult Life: Who Be Treated?: ShouldJessica HueichiNo ratings yet
- Prieto6 Roleofdepression Jco2005Document9 pagesPrieto6 Roleofdepression Jco2005jesusprietusNo ratings yet
- Melanoma Incidence, Recurrence, and Mortality in An Integrated Healthcare System: A Retrospective Cohort StudyDocument9 pagesMelanoma Incidence, Recurrence, and Mortality in An Integrated Healthcare System: A Retrospective Cohort StudyPande Agung MahariskiNo ratings yet
- Allison Clin G Hepatol 2008Document5 pagesAllison Clin G Hepatol 2008Paco MsnroNo ratings yet
- Prognostic Study Following: of Disease-Free and Survival Enucleation For Uveal MelanomaDocument6 pagesPrognostic Study Following: of Disease-Free and Survival Enucleation For Uveal Melanomadhavalb20No ratings yet
- Eli SpotDocument20 pagesEli SpotAdel HamadaNo ratings yet
- Detrano 1989Document7 pagesDetrano 1989Lilims LilithNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofDias PradikaNo ratings yet
- GN Kidney InternationalDocument8 pagesGN Kidney InternationalJessica Victoria SudanawidjajaNo ratings yet
- 429 FullDocument9 pages429 Fullgrum jawNo ratings yet
- Riesgo de EpilepsiaDocument6 pagesRiesgo de EpilepsiaAlfredo Luis Arana MaqueraNo ratings yet
- FARLAND 2021 A Prospective Study of Endometriosis and Risk of Type 2 DiabetesDocument9 pagesFARLAND 2021 A Prospective Study of Endometriosis and Risk of Type 2 DiabetesCristiane HermesNo ratings yet
- Suicidal Death Within A Year of A Cancer Diagnosis A Population Based StudyDocument8 pagesSuicidal Death Within A Year of A Cancer Diagnosis A Population Based StudyLeonardo CarvalhoNo ratings yet
- Impact of Smoking On Multiple Primary Cancers Survival: A Retrospective AnalysisDocument7 pagesImpact of Smoking On Multiple Primary Cancers Survival: A Retrospective Analysisdayu lestariNo ratings yet
- Cushing DiagnosticoDocument2 pagesCushing DiagnosticosiralkNo ratings yet
- Adults Hospitalized With Pneumonia in The United States, Incidence, Epidemiologi, Mortality, 2017Document7 pagesAdults Hospitalized With Pneumonia in The United States, Incidence, Epidemiologi, Mortality, 2017Debi SusantiNo ratings yet
- Farez2011 PDFDocument10 pagesFarez2011 PDFAdindhya Saraswati SuryaNo ratings yet
- Iarjmsr 1 (3) 100-105Document7 pagesIarjmsr 1 (3) 100-105jinuNo ratings yet
- HHS Public Access: Readmission Diagnoses After Severe Sepsis and Other Acute Medical ConditionsDocument5 pagesHHS Public Access: Readmission Diagnoses After Severe Sepsis and Other Acute Medical ConditionsRodrigoSachiFreitasNo ratings yet
- Jurnal PenelitianDocument6 pagesJurnal PenelitianRuli MaulanaNo ratings yet
- Pneumonia in Patients With Diabetes Mellitus: A Single-Center ExperienceDocument5 pagesPneumonia in Patients With Diabetes Mellitus: A Single-Center ExperienceNoer Sidqi MNo ratings yet
- Prevalence of Chronic WoundDocument15 pagesPrevalence of Chronic WoundAnonymous 1nMTZWmzNo ratings yet
- Original Research: Patient and Physician Explanatory Models For Acute BronchitisDocument6 pagesOriginal Research: Patient and Physician Explanatory Models For Acute BronchitisJumria Tandi PanggaloNo ratings yet
- Precision in Pulmonary, Critical Care, and Sleep Medicine: A Clinical and Research GuideFrom EverandPrecision in Pulmonary, Critical Care, and Sleep Medicine: A Clinical and Research GuideJose L. GomezNo ratings yet
- Removal of Uremic Toxins by Renal Replacement Therapies: A Review of Current Progress and Future PerspectivesDocument8 pagesRemoval of Uremic Toxins by Renal Replacement Therapies: A Review of Current Progress and Future PerspectivesindriNo ratings yet
- Pneumothorax: Identification & StabilizationDocument35 pagesPneumothorax: Identification & StabilizationindriNo ratings yet
- ArchRheumatol 32 21Document5 pagesArchRheumatol 32 21indriNo ratings yet
- Generated by Cyberlink U ScannerDocument37 pagesGenerated by Cyberlink U ScannerindriNo ratings yet
- Ultrasound in Management: Gunapriya Rsup Sanglah Oktober 2019Document80 pagesUltrasound in Management: Gunapriya Rsup Sanglah Oktober 2019indriNo ratings yet
- FHDGFGKDocument2 pagesFHDGFGKindriNo ratings yet
- For Older People, Medications Are Common AGS Beers Criteria Aims To Make Them Appropriate, TooDocument3 pagesFor Older People, Medications Are Common AGS Beers Criteria Aims To Make Them Appropriate, TooindriNo ratings yet
- 1.1. Imunologi Sepsis ADW Okt 2019 PKB Paru Surabaya 2019Document54 pages1.1. Imunologi Sepsis ADW Okt 2019 PKB Paru Surabaya 2019indriNo ratings yet
- Older Surgical Patients: Anesthesiologist'S Point of View: Annemarie Chrysantia MelatiDocument35 pagesOlder Surgical Patients: Anesthesiologist'S Point of View: Annemarie Chrysantia MelatiindriNo ratings yet
- Imaging Radiology in Tropical DiseasesDocument78 pagesImaging Radiology in Tropical DiseasesindriNo ratings yet
- Arianti Homeostasis ControlDocument29 pagesArianti Homeostasis ControlindriNo ratings yet
- 1.3. Biomarker Resti 19102019 Revisi 2Document33 pages1.3. Biomarker Resti 19102019 Revisi 2indriNo ratings yet
- Injuries in The Genitourinary Tract: DR H R Danarto - SPB, SpuDocument39 pagesInjuries in The Genitourinary Tract: DR H R Danarto - SPB, SpuindriNo ratings yet
- Belajar Responsi 1Document4 pagesBelajar Responsi 1indriNo ratings yet
- Wa0001Document1 pageWa0001indriNo ratings yet
- Injuries in The Genitourinary Tract: DR H R Danarto - SPB, SpuDocument39 pagesInjuries in The Genitourinary Tract: DR H R Danarto - SPB, SpuindriNo ratings yet
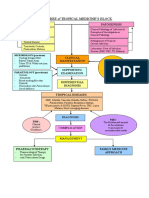
- Topic Tree of Tropical Medicine'S Block: Patogenesis EtiologyDocument1 pageTopic Tree of Tropical Medicine'S Block: Patogenesis EtiologyindriNo ratings yet
- Art:10.1186/1471 2474 15 188Document8 pagesArt:10.1186/1471 2474 15 188indriNo ratings yet
- Word Brochure Template 7 InsideDocument1 pageWord Brochure Template 7 InsideAnonymous ejce48emNo ratings yet
- Alterations With Infectious, Inflammatory and Immunologic ResponsesDocument8 pagesAlterations With Infectious, Inflammatory and Immunologic ResponsesPATRIZJA YSABEL REYESNo ratings yet
- Mid-Term PresentationDocument18 pagesMid-Term Presentationapi-480918653No ratings yet
- Febrile Seizures: Janith ChandrakumaraDocument14 pagesFebrile Seizures: Janith ChandrakumaraJanith ChandrakumaraNo ratings yet
- Childhood Malignancies - Hodgkin's LymphomaDocument6 pagesChildhood Malignancies - Hodgkin's Lymphomavictortayor_26105009No ratings yet
- Concept MapDocument4 pagesConcept Mapdejosep_informaticsNo ratings yet
- Henoch-Schonlein Purpura: An Update: Nutan Kamath, Suchetha RaoDocument7 pagesHenoch-Schonlein Purpura: An Update: Nutan Kamath, Suchetha RaoManjunath VaddambalNo ratings yet
- PDF TextDocument2 pagesPDF TextSATYAM KANNAUJNo ratings yet
- Preventing Pink Eye (Conjunctivitis) - CDCDocument2 pagesPreventing Pink Eye (Conjunctivitis) - CDCShaheer ZahidNo ratings yet
- Biomedical Waste Management MCQDocument3 pagesBiomedical Waste Management MCQSivaNo ratings yet
- Brochure in Health Ed PDFDocument3 pagesBrochure in Health Ed PDFHannalene DolorNo ratings yet
- Bmi 10-AlexandriteDocument1 pageBmi 10-AlexandriteNeth Revelo CastilloNo ratings yet
- Journal of Infection and Public HealthDocument7 pagesJournal of Infection and Public HealthJohnStrowskyNo ratings yet
- Pox Diseases of Animals: Welcome To My Presentation OnDocument36 pagesPox Diseases of Animals: Welcome To My Presentation Onsanchi ranaNo ratings yet
- Nejmcp 1903768Document9 pagesNejmcp 1903768EriC. ChaN.No ratings yet
- Table of Specification Mapeh 10Document4 pagesTable of Specification Mapeh 10Melody Anne Dinoso EvangelistaNo ratings yet
- Rab Flow CHT 3 PeopleDocument2 pagesRab Flow CHT 3 PeopleWDIV/ClickOnDetroitNo ratings yet
- Shock Practice QuestionsDocument4 pagesShock Practice QuestionsSavanna ChambersNo ratings yet
- Cims Case 1 - SGD A4Document16 pagesCims Case 1 - SGD A4SGD A4No ratings yet
- Community Assessment Public Health - 2017Document7 pagesCommunity Assessment Public Health - 2017ardiansyah nochNo ratings yet
- Fluid Volume Deficit R/T Diarrhea & VomitingDocument4 pagesFluid Volume Deficit R/T Diarrhea & Vomitingjisoo100% (3)
- Grade 7 QuestionnaireDocument5 pagesGrade 7 QuestionnaireMarc T Montefalcon100% (2)
- Healy World Certificate of Conformity en EUDocument38 pagesHealy World Certificate of Conformity en EUJOHANNA BJARNERNo ratings yet
- DashBoard Health SampleDocument1 pageDashBoard Health SampleAliChana1No ratings yet
- PMCH March Batch Exams Fully Solved 2020-21Document72 pagesPMCH March Batch Exams Fully Solved 2020-21Priyanka KaranamNo ratings yet
- Assessment Questionnaire GuideDocument7 pagesAssessment Questionnaire GuideKasandra Dawn BerisoNo ratings yet
- DMAC 34 Rev. 1 - Dec 2021 - Guidance For Medical Examiners of Divers Conducting Face-to-FaceDocument6 pagesDMAC 34 Rev. 1 - Dec 2021 - Guidance For Medical Examiners of Divers Conducting Face-to-FaceC. de JongNo ratings yet
- Bingo - ToriDocument2 pagesBingo - Toriapi-541744798No ratings yet
- Hepatitis in Children (Hep A, B, C)Document26 pagesHepatitis in Children (Hep A, B, C)sarNo ratings yet