Download as docx, pdf, or txt
You might also like
- Z-LAND - The Survival Horror RPG - CorebookDocument262 pagesZ-LAND - The Survival Horror RPG - CorebookCaio Cézar Dinelli100% (6)
- Classification of Traditional African InstrumentsDocument3 pagesClassification of Traditional African InstrumentsQuezon D. Lerog Jr.100% (2)
- Medicomat 39Document10 pagesMedicomat 39Ripro SurgNo ratings yet
- Excellent - MeaningDocument3 pagesExcellent - MeaningEmmanuel MahengeNo ratings yet
- Best Tarot Book 25Document5 pagesBest Tarot Book 25Classic Bobby100% (3)
- Rare Disease DatabaseDocument8 pagesRare Disease DatabaseBlueash BehNo ratings yet
- Mitochondrial MyopathiesDocument20 pagesMitochondrial MyopathiescristobalchsNo ratings yet
- Wernicke EncephalopathyDocument14 pagesWernicke Encephalopathynevelle4667No ratings yet
- Mitochondrial Myopathies - Clinical Features and Diagnosis - UpToDateDocument37 pagesMitochondrial Myopathies - Clinical Features and Diagnosis - UpToDateNana ShkodinaNo ratings yet
- Delirium: EpidemiologyDocument8 pagesDelirium: EpidemiologyNunuNo ratings yet
- Cough Pneumonia TuberculosisDocument5 pagesCough Pneumonia TuberculosisمحمدأميندماجNo ratings yet
- Cancer, Also Known As ADocument4 pagesCancer, Also Known As AMarc Lorenz DucusinNo ratings yet
- The Spectrum of Mitochondrial Disease Ep-3-10Document8 pagesThe Spectrum of Mitochondrial Disease Ep-3-10F4AR100% (1)
- Mitochondrial Encephalomyopathies (MEM)Document66 pagesMitochondrial Encephalomyopathies (MEM)Fatma KaledNo ratings yet
- Chap 135Document6 pagesChap 135Jalajarani AridassNo ratings yet
- Chest Wall Deformities by Atrey GaonkarDocument48 pagesChest Wall Deformities by Atrey GaonkaratreygaonkarNo ratings yet
- Transverse MyelitisDocument7 pagesTransverse MyelitisAmr BashaNo ratings yet
- Drug Design Is The Approach of Finding Drugs by Design, Based On TheirDocument62 pagesDrug Design Is The Approach of Finding Drugs by Design, Based On TheirLokendra TripathiNo ratings yet
- Multiple Sclerosis AssignemntDocument5 pagesMultiple Sclerosis AssignemntWAQARAHMED DVMNo ratings yet
- Severe MalariaDocument15 pagesSevere MalariaSwati Pathak GiriNo ratings yet
- Hypothyroidism MEDSTUDENTS-ENDOCRINOLOGYDocument4 pagesHypothyroidism MEDSTUDENTS-ENDOCRINOLOGYdr,indra SpOGNo ratings yet
- Congenital Myopathies: BackgroundDocument34 pagesCongenital Myopathies: BackgroundHerry GunawanNo ratings yet
- Background: Pheochromocytoma Pheochromocytoma Men 2Document12 pagesBackground: Pheochromocytoma Pheochromocytoma Men 2Marisha Christin TarihoranNo ratings yet
- Lawal Mohammed 1Document7 pagesLawal Mohammed 1Muhammad LawalNo ratings yet
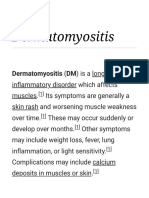
- Dermatomyositis: Dermatomyositis (DM) Is A Long-TermDocument48 pagesDermatomyositis: Dermatomyositis (DM) Is A Long-TermPrihan Fakri PrihanNo ratings yet
- Rapid Pathology Pathology Textbook For Medical StudentsDocument89 pagesRapid Pathology Pathology Textbook For Medical Studentsyennqing100% (1)
- C - The Microwave Syndrome - 13 CategoriesDocument4 pagesC - The Microwave Syndrome - 13 CategoriesEmf RefugeeNo ratings yet
- Copper Trace Element Microorganisms Organs Metabolic HomeostaticDocument26 pagesCopper Trace Element Microorganisms Organs Metabolic HomeostaticinnyNo ratings yet
- SclerodermaDocument17 pagesSclerodermajobinbionicNo ratings yet
- MyelodysplasiaDocument19 pagesMyelodysplasiaJoseph Sibarani EvangelistNo ratings yet
- Presidency School Mangalore: Chromosomal DisordersDocument28 pagesPresidency School Mangalore: Chromosomal DisordersAiman SyedNo ratings yet
- Charles Barker Patent: Copper I Vto Heal Lyme's Disease - Video, PatentsDocument20 pagesCharles Barker Patent: Copper I Vto Heal Lyme's Disease - Video, Patentssmart_chrisNo ratings yet
- Inflammatory Myopathies-1Document39 pagesInflammatory Myopathies-1adamu mohammadNo ratings yet
- Síndrome Parry-RombergDocument5 pagesSíndrome Parry-RombergLuckeinsNo ratings yet
- Nephrotic Syndrome Children PDFDocument11 pagesNephrotic Syndrome Children PDFesdl86No ratings yet
- DERMATOMYOSITISDocument62 pagesDERMATOMYOSITISkhola aijazNo ratings yet
- An Overview of DermatomyositisDocument6 pagesAn Overview of DermatomyositisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Supplementary Information To Chapter 32: Inborn Errors of Metabolism General ConsiderationsDocument24 pagesSupplementary Information To Chapter 32: Inborn Errors of Metabolism General ConsiderationsAaron JoseNo ratings yet
- Recent Update in The Management of Childhood Nephr PDFDocument8 pagesRecent Update in The Management of Childhood Nephr PDFREHNUMA URMINo ratings yet
- PokhrelDocument9 pagesPokhrelsaifulmangopo123No ratings yet
- RebamipideDocument5 pagesRebamipidejunerubinNo ratings yet
- Applied Therapeutics Lec 8Document18 pagesApplied Therapeutics Lec 8human.44697No ratings yet
- Fast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseFrom EverandFast Facts: Familial Chylomicronemia Syndrome: Raising awareness of a rare genetic diseaseNo ratings yet
- Diabetes MellitusDocument43 pagesDiabetes MellitusRobi HSNo ratings yet
- 0002 Rheumatology Notes 2015.... 49Document58 pages0002 Rheumatology Notes 2015.... 49Abdul QuyyumNo ratings yet
- Acute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsDocument44 pagesAcute Myeloblastic Leukaemia: BY DR Halima Talba Consultant Haematologist Department of Haematology and BtsMuhammad Modu BulamaNo ratings yet
- VEM5384 Clincial Neurology DisordersDocument62 pagesVEM5384 Clincial Neurology DisordersdeadnarwhalNo ratings yet
- Biochemical Pharmacology: Joseph George TDocument9 pagesBiochemical Pharmacology: Joseph George TNiarti Ulan SariNo ratings yet
- SarcoidosisDocument12 pagesSarcoidosisSatish Kumar DashNo ratings yet
- Lupus ErythematosusDocument5 pagesLupus ErythematosusAditya DarmawanNo ratings yet
- Non Communicable Disease Grade 7Document4 pagesNon Communicable Disease Grade 7Joshua RamirezNo ratings yet
- Dr. Naveen G Nadig Associate Professor Dept. of Paediatrics Ssims & RC DavanagereDocument48 pagesDr. Naveen G Nadig Associate Professor Dept. of Paediatrics Ssims & RC DavanagereVeerabhadra RadhakrishnaNo ratings yet
- Multiple TeksDocument21 pagesMultiple TeksPampirBolongNo ratings yet
- Pellagra - WikipediaDocument64 pagesPellagra - WikipediaFOOD SCIENCE FOOD TECHNOLOGYNo ratings yet
- Marasmus and PneumoniaDocument8 pagesMarasmus and Pneumoniaதிவ்யாஷ்வினி குமாரன்No ratings yet
- SSM MM20505 Nephrotic SyndromeDocument13 pagesSSM MM20505 Nephrotic SyndromeMUHAMMAD LOKMAN HAKIM BIN MOHD BASRI -No ratings yet
- Medical GeneticsDocument17 pagesMedical Geneticsapi-19641337No ratings yet
- 1) Tay-Sachs Disease & Lysosomes: Elizabeth Jade Vicera 3bio1Document2 pages1) Tay-Sachs Disease & Lysosomes: Elizabeth Jade Vicera 3bio1Beatrix MedinaNo ratings yet
- Clinical AnatomyDocument4 pagesClinical Anatomydrsamia27No ratings yet
- Nephrotic SyndromeDocument21 pagesNephrotic Syndromepreetie8750% (4)
- Multiple Sclerosis PPT 060904Document24 pagesMultiple Sclerosis PPT 060904Isabel HernandezNo ratings yet
- Luis Rodrigo - Iron Deficiency Anemia (2019)Document114 pagesLuis Rodrigo - Iron Deficiency Anemia (2019)Leng BunthaiNo ratings yet
- Erros Inatos Do MetabolismoDocument33 pagesErros Inatos Do MetabolismosurtosedeliriosNo ratings yet
- PolymyositisDocument5 pagesPolymyositisdeea03No ratings yet
- Sindrom HunterDocument9 pagesSindrom HunterhenniwtNo ratings yet
- TBDocument5 pagesTBQuezon D. Lerog Jr.No ratings yet
- St. Jaeger-Lecoultre Patek Philippe Medical Center: Area: Ortho Ward For The Month Of: June 2019Document2 pagesSt. Jaeger-Lecoultre Patek Philippe Medical Center: Area: Ortho Ward For The Month Of: June 2019Quezon D. Lerog Jr.No ratings yet
- Marian Psychia 2Document4 pagesMarian Psychia 2Quezon D. Lerog Jr.No ratings yet
- Sex Differences in Risk and Resilience: Stress Effects On The Neural Substrates of Emotion and MotivationDocument1 pageSex Differences in Risk and Resilience: Stress Effects On The Neural Substrates of Emotion and MotivationQuezon D. Lerog Jr.No ratings yet
- Q2 - Lesson 1 - Worksheet 3 - Card CatalogDocument3 pagesQ2 - Lesson 1 - Worksheet 3 - Card CatalogTine DayotNo ratings yet
- Ind AS 115Document36 pagesInd AS 115yashNo ratings yet
- Ragunan Zoo FileDocument3 pagesRagunan Zoo FileMuhammad FauziNo ratings yet
- Equipment Reliability AnalysisDocument1 pageEquipment Reliability AnalysisnukkeNo ratings yet
- Release Technique News Letter Dec 2015Document59 pagesRelease Technique News Letter Dec 2015hanako1192100% (1)
- Teaching and Learning Supervision Teachers AttituDocument15 pagesTeaching and Learning Supervision Teachers AttituRevathi KanasanNo ratings yet
- Definition of Good GovernanceDocument3 pagesDefinition of Good GovernanceHaziq KhanNo ratings yet
- ReplicationDocument11 pagesReplicationUgur EksiNo ratings yet
- Lecture 13 - LADocument9 pagesLecture 13 - LAHafiza Iqra MaqboolNo ratings yet
- Pawel Safuryn CVDocument1 pagePawel Safuryn CVapi-296200553No ratings yet
- Nurse Entrepreneur: Name: Alex Kate C. Dela Year & Section: BSN 3-ADocument6 pagesNurse Entrepreneur: Name: Alex Kate C. Dela Year & Section: BSN 3-Akassy yeonNo ratings yet
- Biology ProjectDocument19 pagesBiology ProjectJaya mohanNo ratings yet
- Impact of Orthodontic Treatment On Oral Health-Related Quality of Life in The Slovak Republic: A Cross-Sectional StudyDocument10 pagesImpact of Orthodontic Treatment On Oral Health-Related Quality of Life in The Slovak Republic: A Cross-Sectional StudyKornist BufuNo ratings yet
- Dathathreya Stotras and Avadhootha GitaDocument138 pagesDathathreya Stotras and Avadhootha Gitaaditya kalekarNo ratings yet
- Define Applied EconomicsDocument18 pagesDefine Applied EconomicsThalia Rhine AberteNo ratings yet
- SASTRA University-B.tech Mechatronics Syllabus SheetDocument106 pagesSASTRA University-B.tech Mechatronics Syllabus SheetSrikant Gadicherla100% (1)
- Proof by Induction - FactorialsDocument1 pageProof by Induction - FactorialsejlflopNo ratings yet
- Ahavas TorahDocument24 pagesAhavas TorahJose MartinezNo ratings yet
- Ipw WRDocument176 pagesIpw WRMay FaroukNo ratings yet
- Module 3 - Group 2-XYZ CaseletDocument3 pagesModule 3 - Group 2-XYZ CaseletconeshaNo ratings yet
- Lateral ThinkingDocument6 pagesLateral ThinkingKrengy TwiggAlinaNo ratings yet
- PBL NMR 1Document5 pagesPBL NMR 1andiNo ratings yet
- 1Document11 pages1Amjad PiroutiNo ratings yet
- BudgetDocument24 pagesBudgetYoussef MohammedNo ratings yet
- Discrete Prob Practice QsDocument8 pagesDiscrete Prob Practice QsAitzul SchkohNo ratings yet
- Synfocity 632 PDFDocument2 pagesSynfocity 632 PDFMizoram Presbyterian Church SynodNo ratings yet