Download as pdf or txt
You might also like
- Wifi Jammer: Winter Semester 2020-21 Analog Circuits Ece 2028Document10 pagesWifi Jammer: Winter Semester 2020-21 Analog Circuits Ece 2028Sathwik YadalamNo ratings yet
- European Journal of Medicinal Chemistry: Research PaperDocument14 pagesEuropean Journal of Medicinal Chemistry: Research PaperWalid Ebid ElgammalNo ratings yet
- Novel Targeted Therapies For Chronic Lymphocytic Leukemia in Elderly Patients: A Systematic ReviewDocument13 pagesNovel Targeted Therapies For Chronic Lymphocytic Leukemia in Elderly Patients: A Systematic ReviewVishal BondeNo ratings yet
- Jurnal AntibodimonoklonalDocument11 pagesJurnal AntibodimonoklonalKartika PuspitaningrumNo ratings yet
- New Drugs For Peripheral T-Cell Lymphomas: Gallium NitrateDocument4 pagesNew Drugs For Peripheral T-Cell Lymphomas: Gallium Nitrateassam1No ratings yet
- Cancers: Advances in Acute Myeloid Leukemia: Recently Approved Therapies and Drugs in DevelopmentDocument32 pagesCancers: Advances in Acute Myeloid Leukemia: Recently Approved Therapies and Drugs in DevelopmentDanyal SiddiquiNo ratings yet
- 2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolDocument113 pages2018 CML Updates and Case Presentations: Washington University in ST Louis Medical SchoolIris GzlzNo ratings yet
- Leukemia Research: Nurgül Özgür Yurttaş, Ahmet Emre Eşkazan TDocument8 pagesLeukemia Research: Nurgül Özgür Yurttaş, Ahmet Emre Eşkazan Tsugi9namliNo ratings yet
- Brown 2014Document9 pagesBrown 2014Rafaela Queiroz MascarenhasNo ratings yet
- Chronic Myeloid Leukemia in 2020Document11 pagesChronic Myeloid Leukemia in 2020ErnestoSalazarNo ratings yet
- The Dual Cell Cycle Kinase Inhibitor JNJ-7706621 Reverses Resistance To CD37-Targeted Radioimmunotherapy in Activated B Cell Like Diffuse Large B Cell Lymphoma Cell LinesDocument17 pagesThe Dual Cell Cycle Kinase Inhibitor JNJ-7706621 Reverses Resistance To CD37-Targeted Radioimmunotherapy in Activated B Cell Like Diffuse Large B Cell Lymphoma Cell Lines2512505993No ratings yet
- In Vitro: Wu-Chou Su, Shu-Ling Chang, Tsai-Yun Chen, Jiann-Shiuh Chen and Chao-Jung TsaoDocument6 pagesIn Vitro: Wu-Chou Su, Shu-Ling Chang, Tsai-Yun Chen, Jiann-Shiuh Chen and Chao-Jung TsaoJohn GuerreroNo ratings yet
- Factors Affecting The Pharmacology of ADCDocument28 pagesFactors Affecting The Pharmacology of ADCCher IshNo ratings yet
- CML EsmoDocument3 pagesCML EsmowidweedNo ratings yet
- Pharmacological Research: Invited ReviewDocument15 pagesPharmacological Research: Invited ReviewFajar NugrahantoNo ratings yet
- A Comparison of Physicochemical Property Profiles of Marketed Oral Drugs and Orally Bioavailable Anti-Cancer Protein Kinase Inhibitors in Clinical DevelopmentDocument16 pagesA Comparison of Physicochemical Property Profiles of Marketed Oral Drugs and Orally Bioavailable Anti-Cancer Protein Kinase Inhibitors in Clinical DevelopmentArturo T. Sánchez-MoraNo ratings yet
- fonc-11-737943Document20 pagesfonc-11-737943popdianamadalinaNo ratings yet
- 4Q19 and Year ReviewDocument7 pages4Q19 and Year ReviewShambavaNo ratings yet
- Clopidogrel PharmacogeneticsDocument11 pagesClopidogrel PharmacogeneticsGisela GloryNo ratings yet
- Cyclin-Dependent KinaseDocument8 pagesCyclin-Dependent KinasetonnyNo ratings yet
- Clopidogrel PharmacogeneticsDocument11 pagesClopidogrel PharmacogeneticsYaxkin NikNo ratings yet
- Phase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.Document10 pagesPhase II Trial of Curcumin in Patients With Advanced Pancreatic Cancer.João FrancoNo ratings yet
- TKF 2Document4 pagesTKF 2api-257045584No ratings yet
- Jop 18 00005Document4 pagesJop 18 00005Anonymous 8KN8IR1GTWNo ratings yet
- IO in ReviewDocument8 pagesIO in Reviewfenrisulven2010No ratings yet
- CN 19 1246Document18 pagesCN 19 1246Alexandra MoraesNo ratings yet
- Chronic Myeloid LeukemiaDocument18 pagesChronic Myeloid LeukemiaNour AngriniNo ratings yet
- Mondello Et Al. - 2016 - 90 Y-Ibritumomab Tiuxetan A Nearly Forgotten OpportunityDocument13 pagesMondello Et Al. - 2016 - 90 Y-Ibritumomab Tiuxetan A Nearly Forgotten OpportunityacbgdvNo ratings yet
- Cancer - 2009 - McDermott - Retracted Immunotherapy of Metastatic Renal Cell CarcinomaDocument8 pagesCancer - 2009 - McDermott - Retracted Immunotherapy of Metastatic Renal Cell CarcinomaSubur HantoroNo ratings yet
- Phase I Study of Cladribine (2-Chlorodeoxyadenosine) in Lymphoid Malignancies 1997Document8 pagesPhase I Study of Cladribine (2-Chlorodeoxyadenosine) in Lymphoid Malignancies 1997Koko na kokoNo ratings yet
- Fonc 09 00665Document7 pagesFonc 09 00665desilasarybasriNo ratings yet
- The Role of Biomarkers inDocument16 pagesThe Role of Biomarkers inSoniamartilovaNo ratings yet
- Proliferation Inhibition and Apoptosis Induction of Imatinib-Resistant Chronic Myeloid Leukemia Cells Via PPP2R5C Down-RegulationDocument12 pagesProliferation Inhibition and Apoptosis Induction of Imatinib-Resistant Chronic Myeloid Leukemia Cells Via PPP2R5C Down-RegulationjessicaNo ratings yet
- Li 2013Document9 pagesLi 2013KianaNo ratings yet
- Eur J Immunol - 2021 - Fink - Immunity in Acute Myeloid Leukemia Where The Immune Response and Targeted Therapy MeetDocument10 pagesEur J Immunol - 2021 - Fink - Immunity in Acute Myeloid Leukemia Where The Immune Response and Targeted Therapy MeetSam SonNo ratings yet
- New Biologics in The Treatment of UrticariaDocument7 pagesNew Biologics in The Treatment of UrticariaArezoo JamNo ratings yet
- Cisplatin: Cisplatin Is A Chemotherapy MedicationDocument40 pagesCisplatin: Cisplatin Is A Chemotherapy MedicationSuman KusumNo ratings yet
- Ajcpath123 0879Document7 pagesAjcpath123 0879Isikhuemen MaradonaNo ratings yet
- 2.42016 LeukemiaandCurcuminDocument9 pages2.42016 LeukemiaandCurcuminYudi Gebri FoennaNo ratings yet
- TP53 TP53 TP53 TP53: Therapy Tested Marker Predicted ResponseDocument11 pagesTP53 TP53 TP53 TP53: Therapy Tested Marker Predicted Responsekunal mhetreNo ratings yet
- 722Document7 pages722Cimaie JellyNo ratings yet
- Therapy Tested Marker Predicted Response: Imatinib Sunitinib RegorafenibDocument11 pagesTherapy Tested Marker Predicted Response: Imatinib Sunitinib RegorafenibArif MehmoodNo ratings yet
- Small Molecule Kinase Inhibitors From Lab Bench To ClinicDocument4 pagesSmall Molecule Kinase Inhibitors From Lab Bench To Clinicsatya_chagantiNo ratings yet
- Captopril Inhibits Angiogenesis and Slows The Growth of Experimental Tumors in RatsDocument10 pagesCaptopril Inhibits Angiogenesis and Slows The Growth of Experimental Tumors in RatsnepretipNo ratings yet
- Biochemical and Biophysical Research CommunicationsDocument7 pagesBiochemical and Biophysical Research CommunicationsFrankenstein MelancholyNo ratings yet
- Presentación 13Document19 pagesPresentación 13Felipe RayoNo ratings yet
- CA and BCR Abl Mut in Nilotinib Response PDFDocument7 pagesCA and BCR Abl Mut in Nilotinib Response PDFRyan ViantinoNo ratings yet
- Paper Seccion 2 ViernesDocument5 pagesPaper Seccion 2 Viernesabcd 1234No ratings yet
- Jin Et Al-2023-Cardiotoxicity of Lung Cancer Related Immunotherapy Vs ChemotherapyDocument11 pagesJin Et Al-2023-Cardiotoxicity of Lung Cancer Related Immunotherapy Vs ChemotherapyDimas AdhiatmaNo ratings yet
- By Aalpesh Kachhadiya 2009H108403HDocument34 pagesBy Aalpesh Kachhadiya 2009H108403HLakshmi IndiraNo ratings yet
- Tubulin and Microtubules As Targets For Anticancer DrugsDocument18 pagesTubulin and Microtubules As Targets For Anticancer DrugsRich StantonNo ratings yet
- Targeted Therapy in Oncology: Update ArticleDocument5 pagesTargeted Therapy in Oncology: Update ArticleRajeev GuptaNo ratings yet
- Pi Is 1556086415330872Document2 pagesPi Is 1556086415330872Muthia FadhilaNo ratings yet
- Cassidysyed 2016Document2 pagesCassidysyed 2016drravikishoraNo ratings yet
- Antimicrobial Agents and Chemotherapy-1999-Terashi-21.fullDocument4 pagesAntimicrobial Agents and Chemotherapy-1999-Terashi-21.fullAndikhaNo ratings yet
- Pi Is 1933287417302908Document11 pagesPi Is 1933287417302908Anonymous yptjlwJNo ratings yet
- Analysis of CD16þCD56dim NK Cells From CLL Patients Evidence Supporting ADocument9 pagesAnalysis of CD16þCD56dim NK Cells From CLL Patients Evidence Supporting Aimmunologie cellulaireNo ratings yet
- crc-23-0430.pdfDocument17 pagescrc-23-0430.pdfvijay.ganesanNo ratings yet
- Metabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsDocument33 pagesMetabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsAndi wahyuniNo ratings yet
- Procalcitonin in Special Patient Populations: Guidance For Antimicrobial TherapyDocument13 pagesProcalcitonin in Special Patient Populations: Guidance For Antimicrobial TherapyAngellikitaa DemorrisonNo ratings yet
- Tees 2016Document39 pagesTees 2016Jose Angel AbadíaNo ratings yet
- Phytanic Acid and The Risk of Non-Hodgkin LymphomaDocument6 pagesPhytanic Acid and The Risk of Non-Hodgkin LymphomaJose Angel AbadíaNo ratings yet
- Chronic Lymphocytic Leukemia (CLL) - Then and Now: Critical ReviewDocument11 pagesChronic Lymphocytic Leukemia (CLL) - Then and Now: Critical ReviewJose Angel AbadíaNo ratings yet
- Dieta y CancerDocument11 pagesDieta y CancerJose Angel AbadíaNo ratings yet
- Dieta y LeucemiaDocument53 pagesDieta y LeucemiaJose Angel AbadíaNo ratings yet
- Dietary Factors and Risk of Non-Hodgkin Lymphoma in Men and WomenDocument10 pagesDietary Factors and Risk of Non-Hodgkin Lymphoma in Men and WomenJose Angel AbadíaNo ratings yet
- Fruta y LinfomaDocument15 pagesFruta y LinfomaJose Angel AbadíaNo ratings yet
- Parik H 2016Document35 pagesParik H 2016Jose Angel AbadíaNo ratings yet
- Intakes of Fruits, Vegetables, and Related Nutrients and The Risk of Non-Hodgkin's Lymphoma Among WomenDocument10 pagesIntakes of Fruits, Vegetables, and Related Nutrients and The Risk of Non-Hodgkin's Lymphoma Among WomenJose Angel AbadíaNo ratings yet
- NIH Public Access: Author ManuscriptDocument9 pagesNIH Public Access: Author ManuscriptJose Angel AbadíaNo ratings yet
- Tees 2016Document39 pagesTees 2016Jose Angel AbadíaNo ratings yet
- CLL ChiorazziRaiDocument12 pagesCLL ChiorazziRaiJose Angel AbadíaNo ratings yet
- Rol Dieta y CancerDocument15 pagesRol Dieta y CancerJose Angel AbadíaNo ratings yet
- Kemp in 2013Document12 pagesKemp in 2013Jose Angel AbadíaNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptJose Angel AbadíaNo ratings yet
- Histologic Transformation of Chronic Lymphocytic Leukemia/Small Lymphocytic LymphomaDocument41 pagesHistologic Transformation of Chronic Lymphocytic Leukemia/Small Lymphocytic LymphomaJose Angel AbadíaNo ratings yet
- Author 'S Accepted Manuscript: WWW - Elsevier.de/endendDocument31 pagesAuthor 'S Accepted Manuscript: WWW - Elsevier.de/endendJose Angel AbadíaNo ratings yet
- Choi2016 1Document14 pagesChoi2016 1Jose Angel AbadíaNo ratings yet
- Casa Bonne 2016Document11 pagesCasa Bonne 2016Jose Angel AbadíaNo ratings yet
- Accepted Manuscript: Critical Reviews in Oncology/HematologyDocument30 pagesAccepted Manuscript: Critical Reviews in Oncology/HematologyJose Angel AbadíaNo ratings yet
- Campagna 2015Document6 pagesCampagna 2015Jose Angel AbadíaNo ratings yet
- Astm C 592Document9 pagesAstm C 592hoseinNo ratings yet
- Environmental Crisis Causes and ManifestationsDocument26 pagesEnvironmental Crisis Causes and Manifestationsबाजीराव सिंघम0% (1)
- Call History 640273efa1d48Document2 pagesCall History 640273efa1d48Krishnapriya GovindNo ratings yet
- PHAS0027 RevisionDocument21 pagesPHAS0027 Revisionunknown.unknown9901No ratings yet
- An International Cohort Study of Cancer in Systemic Lupus ErythematosusDocument10 pagesAn International Cohort Study of Cancer in Systemic Lupus ErythematosusCristina TudorNo ratings yet
- NeuroVascular (NV) Holding PointsDocument2 pagesNeuroVascular (NV) Holding PointsHatem Farouk100% (2)
- T N M M T N M M: HE EW Essies Anual HE EW Essies AnualDocument8 pagesT N M M T N M M: HE EW Essies Anual HE EW Essies AnualMunna100% (1)
- Wear Solutions BrochureDocument16 pagesWear Solutions BrochureOkan KalendarNo ratings yet
- Toothpaste Survey FormDocument1 pageToothpaste Survey FormBimalendu Konar50% (2)
- Stilboestrol Tablets MSDSDocument6 pagesStilboestrol Tablets MSDSIsaac lauricNo ratings yet
- Guide To Laboratory Establishment For Plant Nutrient AnalysisDocument1 pageGuide To Laboratory Establishment For Plant Nutrient AnalysisOsama MadanatNo ratings yet
- TN-4620190912122 Form21B Signed PDFDocument1 pageTN-4620190912122 Form21B Signed PDFDHEEN MEDICALSNo ratings yet
- Obat Kausatif Infeksi: 6ggpo, 0shqwlget Grad Corporis Ult Hui Form 3DDocument5 pagesObat Kausatif Infeksi: 6ggpo, 0shqwlget Grad Corporis Ult Hui Form 3DMaulana Malik IbrahimNo ratings yet
- A Review On Ultra High Performance Concrete Part II. Hydration, Microstructure and Properties PDFDocument10 pagesA Review On Ultra High Performance Concrete Part II. Hydration, Microstructure and Properties PDFNocifLyesNo ratings yet
- (U) Daily Activity Report: Marshall DistrictDocument5 pages(U) Daily Activity Report: Marshall DistrictFauquier NowNo ratings yet
- Wet RisersDocument3 pagesWet RisersNur Amirah Abdul JamilNo ratings yet
- Environmental Geotechniques: Theories of Ion ExchangeDocument21 pagesEnvironmental Geotechniques: Theories of Ion ExchangeTenkurala srujanaNo ratings yet
- Learning Activity Sheet Electronics G10 Q3 W1Document5 pagesLearning Activity Sheet Electronics G10 Q3 W1Mark Anthony Discarga JetajobeNo ratings yet
- General Physics 1: ACTIVITY/ANSWER SHEET: Quarter 2Document1 pageGeneral Physics 1: ACTIVITY/ANSWER SHEET: Quarter 2Kashima KotaroNo ratings yet
- Discard ManagementDocument9 pagesDiscard ManagementDevvrath SinghNo ratings yet
- Chemistry Project 2021-2022Document19 pagesChemistry Project 2021-2022Rudra SathwaraNo ratings yet
- Re 51400Document14 pagesRe 51400Jamin Smtpng0% (1)
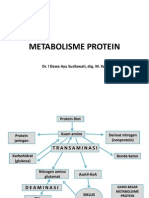
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- Material Sub Group Item CodeDocument2,818 pagesMaterial Sub Group Item Codegouri gouriNo ratings yet
- Drug Ana Surgery WardDocument11 pagesDrug Ana Surgery WardJames QuilingNo ratings yet
- Feasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentDocument9 pagesFeasibility of Screening For Preschool Behavioral and Emotional Problems in Primary Care Using The Early Childhood Screening AssessmentAhmed RamzyNo ratings yet
- Model ETR-9200 Automatic Tuning Smarter Logic ControllerDocument26 pagesModel ETR-9200 Automatic Tuning Smarter Logic ControllervhelectronicaNo ratings yet
- Barron's Bigbook Special WordDocument123 pagesBarron's Bigbook Special WordArif Al MamunNo ratings yet
- American FoodDocument10 pagesAmerican FoodEvan BanksNo ratings yet