
Professional Documents
Culture Documents
Synovial Tissue Research State of The Art Review
Synovial Tissue Research State of The Art Review
Uploaded by
Deliana Nur Ihsani RahmiCopyright:
Available Formats
You might also like
- Redefining Lupus Nephritis, Clinical Implications of Pathophysiologic Subtypes PDFDocument14 pagesRedefining Lupus Nephritis, Clinical Implications of Pathophysiologic Subtypes PDFaneliatiarasuciNo ratings yet
- 10 1038@nrneph 2017 85 PDFDocument13 pages10 1038@nrneph 2017 85 PDFSirGonzNo ratings yet
- Smolen2018 PDFDocument23 pagesSmolen2018 PDFJose Correa100% (1)
- Tsokos 2016Document15 pagesTsokos 2016karen rinconNo ratings yet
- Nrgastro 2017 1Document12 pagesNrgastro 2017 1Golam ZakariaNo ratings yet
- Neutrophil Migration Nature RevImmunol 2016Document14 pagesNeutrophil Migration Nature RevImmunol 2016stefanie.sousaNo ratings yet
- Engineering and Physical Sciences in Oncology - Challenges and OpportunitiesDocument17 pagesEngineering and Physical Sciences in Oncology - Challenges and OpportunitiesAlessandroNo ratings yet
- Cryptococcal MeningitisDocument12 pagesCryptococcal MeningitisIan SaundersNo ratings yet
- Barturen 2018Document20 pagesBarturen 2018jezy2014No ratings yet
- Orofacial Manifestations of Systemic SclerosisDocument6 pagesOrofacial Manifestations of Systemic SclerosisIt's MeNo ratings yet
- Loeser PDFDocument9 pagesLoeser PDFGaudeamus IgiturNo ratings yet
- Estefania Gallego PonenciaDocument16 pagesEstefania Gallego PonenciaJilberth Hermann CandeloNo ratings yet
- ES GastrointestinalDocument12 pagesES GastrointestinalMateus ValenteNo ratings yet
- Oesophageal Cancer-1Document1 pageOesophageal Cancer-1BRENDANo ratings yet
- Modelling Diabetic Nephropathy in MiceDocument9 pagesModelling Diabetic Nephropathy in MiceKarina ThiemeNo ratings yet
- NRDP 20174Document17 pagesNRDP 20174EccoNo ratings yet
- Lectura Seminario 3 - NF1Document17 pagesLectura Seminario 3 - NF1Diego SoteloNo ratings yet
- Tuberculous MeningitisDocument18 pagesTuberculous Meningitistjdvv8cbfrNo ratings yet
- Manifestaciones Neurologicas VIH NatureDocument13 pagesManifestaciones Neurologicas VIH NatureGeral D. VelascoNo ratings yet
- Panes Rimola 2017Document13 pagesPanes Rimola 2017Natasya DarrelNo ratings yet
- Potential New Therapy For OphthalmopathyDocument1 pagePotential New Therapy For OphthalmopathyEsteban Martin Chiotti KaneshimaNo ratings yet
- Oligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Document11 pagesOligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Orlando SotoNo ratings yet
- Kellum 2018Document14 pagesKellum 2018hemer hadyn calderon alvitesNo ratings yet
- Targeting Neoantigens To Augment Antitumour ImmunityDocument14 pagesTargeting Neoantigens To Augment Antitumour Immunitylaura isabellaNo ratings yet
- Primer. Vejiga. 2017Document19 pagesPrimer. Vejiga. 2017Isabel Gago CastilloNo ratings yet
- Living KidneyDocument9 pagesLiving KidneyEss liNo ratings yet
- Reviews: Hirschsprung Disease - Integrating Basic Science and Clinical Medicine To Improve OutcomesDocument16 pagesReviews: Hirschsprung Disease - Integrating Basic Science and Clinical Medicine To Improve OutcomesThanh Thảo PhanNo ratings yet
- Reviews: Computational Genomics Tools For Dissecting Tumour-Immune Cell InteractionsDocument18 pagesReviews: Computational Genomics Tools For Dissecting Tumour-Immune Cell Interactionsdata lmleNo ratings yet
- Consensus: StatementDocument10 pagesConsensus: StatementAdrilupiss ArroyoNo ratings yet
- Update On Outcome Assessment in MyositisDocument16 pagesUpdate On Outcome Assessment in MyositisKevin Christofer NavejasNo ratings yet
- Kahrilas 2017Document12 pagesKahrilas 2017Josseph EscobarNo ratings yet
- Hepatocarcinoma 2Document23 pagesHepatocarcinoma 2NaraMayhumiDeBelenMerinoOrtizNo ratings yet
- Beyond Binding Antibody - Lu Et Al. NatureDocument17 pagesBeyond Binding Antibody - Lu Et Al. NatureSamia NouhNo ratings yet
- Membranosa 2Document17 pagesMembranosa 2Carolina CastroNo ratings yet
- Art RitisDocument15 pagesArt RitisHarwin JHoel Salazar UrbanoNo ratings yet
- 16 Bioresponsive MaterialsDocument17 pages16 Bioresponsive MaterialsAlex. SonicaNo ratings yet
- Alhmeimer 23445Document15 pagesAlhmeimer 23445safia osmanNo ratings yet
- ANTYPHOSPHODocument20 pagesANTYPHOSPHOLuis David Beltran OntiverosNo ratings yet
- Scleroderma Renal Crisis and Renal Involvement in Systemic SclerosisDocument14 pagesScleroderma Renal Crisis and Renal Involvement in Systemic Sclerosiszlaticab4246No ratings yet
- Abdollahi-Roodsaz2016 Artigo3Document10 pagesAbdollahi-Roodsaz2016 Artigo3JamilaNo ratings yet
- Nrgastro 2017 38Document15 pagesNrgastro 2017 38Fasya DaffaNo ratings yet
- Development and Regulation of Single - and Multi-Species Candida Albicans BiofilmsDocument13 pagesDevelopment and Regulation of Single - and Multi-Species Candida Albicans BiofilmsCatalina AguayoNo ratings yet
- Yazici Et Al - 2018 - Behçet SyndromeDocument13 pagesYazici Et Al - 2018 - Behçet SyndromeantonioivNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Kuner 2016Document11 pagesKuner 2016Guilherme MonteiroNo ratings yet
- Reviews: Autism Genetics: Opportunities and Challenges For Clinical TranslationDocument15 pagesReviews: Autism Genetics: Opportunities and Challenges For Clinical TranslationAlexandra DragomirNo ratings yet
- Reviews: A Clinicopathological Approach To The Diagnosis of DementiaDocument16 pagesReviews: A Clinicopathological Approach To The Diagnosis of DementiaLeonardo Barrera ArizaNo ratings yet
- 1 ISAPP Consensus Statement PREBIOTICS 2017Document12 pages1 ISAPP Consensus Statement PREBIOTICS 2017KatherineNo ratings yet
- Dyslipidaemia in Nephrotic Syndrome: Mechanisms and TreatmentDocument14 pagesDyslipidaemia in Nephrotic Syndrome: Mechanisms and TreatmentEss liNo ratings yet
- CiliopatiasDocument15 pagesCiliopatiasdhernandez35No ratings yet
- Primer: Antiphospholipid SyndromeDocument19 pagesPrimer: Antiphospholipid SyndromenowimsunheeNo ratings yet
- Escobar Mor Real e 2018Document15 pagesEscobar Mor Real e 2018HIDAYATUL RAHMINo ratings yet
- Nrneurol 2018 30 PDFDocument16 pagesNrneurol 2018 30 PDFFathan MustafidNo ratings yet
- 10 1038@nrurol 2018 1Document15 pages10 1038@nrurol 2018 1cristianNo ratings yet
- Wing Ho Man (2017) Microbiota of The Respiratory Tract, Gatekeeper To Respiratory HealthDocument12 pagesWing Ho Man (2017) Microbiota of The Respiratory Tract, Gatekeeper To Respiratory HealthLuan DiasNo ratings yet
- A Systemic View of Alzheimer Disease 2017Document12 pagesA Systemic View of Alzheimer Disease 2017Jaime Arevalo PanduroNo ratings yet
- Complex Regional Pain Syndrome - Diagnosis, Treatment and Future PerspectivesDocument14 pagesComplex Regional Pain Syndrome - Diagnosis, Treatment and Future Perspectivesyulita kesumaNo ratings yet
- Reviews: Inflammation in Gout: Mechanisms and Therapeutic TargetsDocument9 pagesReviews: Inflammation in Gout: Mechanisms and Therapeutic TargetsBless MineNo ratings yet
- Nrneph 2017 148Document19 pagesNrneph 2017 148Gabriela CarolinaNo ratings yet
- Raynaud’s Phenomenon: A Guide to Pathogenesis and TreatmentFrom EverandRaynaud’s Phenomenon: A Guide to Pathogenesis and TreatmentFredrick M. WigleyNo ratings yet
- Case Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Document18 pagesCase Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Shane Aileen AngelesNo ratings yet
- DrugmedsDocument52 pagesDrugmedsshirleyNo ratings yet
- Hiv/Aids: Elsebey NotesDocument22 pagesHiv/Aids: Elsebey NotesrsimranjitNo ratings yet
- Gross Anatomy of The Digestive System Lecture Notes Lecture 2Document5 pagesGross Anatomy of The Digestive System Lecture Notes Lecture 2Lorelie AsisNo ratings yet
- Multiple Sclerosis Lancet 2018Document15 pagesMultiple Sclerosis Lancet 2018Sarah Miryam CoffanoNo ratings yet
- Ebook Psychology Psyc2020 Psyc2021 Custom Edition by Schutte E Ed Et A PDF Full Chapter PDFDocument67 pagesEbook Psychology Psyc2020 Psyc2021 Custom Edition by Schutte E Ed Et A PDF Full Chapter PDFedward.bittner820100% (35)
- Week 6 PCP Workbook QsDocument6 pagesWeek 6 PCP Workbook Qsapi-479849199No ratings yet
- Module Pharma 1Document21 pagesModule Pharma 1Donya GholamiNo ratings yet
- NEET PG Syllabus 2024 - Detailed Subject-Wise TopicsDocument70 pagesNEET PG Syllabus 2024 - Detailed Subject-Wise Topicsmayur TNo ratings yet
- Aubf Lab Microscopic Examination Part 1Document2 pagesAubf Lab Microscopic Examination Part 1Hannah KateNo ratings yet
- Furosemide Summary Report Committee Veterinary Medicinal Products enDocument9 pagesFurosemide Summary Report Committee Veterinary Medicinal Products enLucijaRomićNo ratings yet
- OSCE Book 2010-1 PDFDocument256 pagesOSCE Book 2010-1 PDFSyeda Eshaal Javaid100% (1)
- Case Study Fracture 2 (Drug Study and NCP)Document8 pagesCase Study Fracture 2 (Drug Study and NCP)chrom17No ratings yet
- Trigger Topics For FMG Exams by MistDocument3 pagesTrigger Topics For FMG Exams by Mistvijay resuNo ratings yet
- Cardio Exercise Testing in Children and AdolecentsDocument288 pagesCardio Exercise Testing in Children and AdolecentsTeoNo ratings yet
- Escleritis EpiescleritisDocument16 pagesEscleritis EpiescleritisAngeloCarpioNo ratings yet
- 2 OS To PrintDocument12 pages2 OS To PrintDENTAL REVIEWER ONLY0% (1)
- Sessile Serrated Adenoma - Libre PathologyDocument5 pagesSessile Serrated Adenoma - Libre PathologyfadoNo ratings yet
- Thyroid Disorders Part I Hyperthyroidism Little 2006Document9 pagesThyroid Disorders Part I Hyperthyroidism Little 2006Jing XueNo ratings yet
- Amiodarone Infusion GuidelineDocument3 pagesAmiodarone Infusion GuidelineNur SusiawantyNo ratings yet
- Idiopathic Talipes Equinovarus Congenital ClubfootDocument15 pagesIdiopathic Talipes Equinovarus Congenital ClubfootNindy PutriNo ratings yet
- Barium Enema and Biliary System1Document18 pagesBarium Enema and Biliary System1sheenamarielaruyaNo ratings yet
- Ketorolac Tromethamine Injection Usp: Product MonographDocument41 pagesKetorolac Tromethamine Injection Usp: Product MonographWahyu AriawanNo ratings yet
- Bifascicular Block Revealing Steinerts Myotonic DystrophyDocument8 pagesBifascicular Block Revealing Steinerts Myotonic DystrophyIJAR JOURNALNo ratings yet
- K - 7 Supraventrikular Takikardia (IKA)Document12 pagesK - 7 Supraventrikular Takikardia (IKA)thomasfelixNo ratings yet
- AMPXICILLINDocument3 pagesAMPXICILLINPark JeongyeonNo ratings yet
- Tinea Versicolor (Pityriasis Versicolor) - UpToDateDocument47 pagesTinea Versicolor (Pityriasis Versicolor) - UpToDatejotaere RobNo ratings yet
- Facial InjuryDocument40 pagesFacial Injuryahmad iffa maududyNo ratings yet
- Curiculum VitaeDocument5 pagesCuriculum VitaeZEINABAHMEDNo ratings yet
- " Drop Foot": Arranged By: Nabiilah Aznesia NPM 71170891191Document12 pages" Drop Foot": Arranged By: Nabiilah Aznesia NPM 71170891191NaomiRimaClaudyaNo ratings yet

























































































Synovial Tissue Research State of The Art Review
Synovial Tissue Research State of The Art Review
Uploaded by
Deliana Nur Ihsani RahmiOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Synovial Tissue Research State of The Art Review
Synovial Tissue Research State of The Art Review
Uploaded by
Deliana Nur Ihsani RahmiCopyright:
Available Formats
REVIEWS
Synovial tissue research:
a state‑of‑the-art review
Carl Orr1, Elsa Sousa2, David L. Boyle3, Maya H. Buch4, Christopher D. Buckley5,
Juan D. Cañete6, Anca I. Catrina7, Ernest H. S. Choy8, Paul Emery4, Ursula Fearon9,
Andrew Filer5, Danielle Gerlag10,11, Frances Humby12, John D. Isaacs13, Søren A. Just14,
Bernard R. Lauwerys15, Benoit Le Goff16, Antonio Manzo17, Trudy McGarry9,
Iain B. McInnes18, Aurélie Najm16, Constantino Pitzalis12, Arthur Pratt13, Malcolm Smith19,
Paul P. Tak10,20, Rogier Thurlings21, João E. Fonseca2 and Douglas J. Veale1
Abstract | The synovium is the major target tissue of inflammatory arthritides such as rheumatoid
arthritis. The study of synovial tissue has advanced considerably throughout the past few decades
from arthroplasty and blind needle biopsy to the use of arthroscopic and ultrasonographic
technologies that enable easier visualization and improve the reliability of synovial biopsies.
Rapid progress has been made in using synovial tissue to study disease pathogenesis, to stratify
patients, to discover biomarkers and novel targets, and to validate therapies, and this progress
has been facilitated by increasingly diverse and sophisticated analytical and technological
approaches. In this Review, we describe these approaches, and summarize how their use in
synovial tissue research has improved our understanding of rheumatoid arthritis and identified
candidate biomarkers that could be used in disease diagnosis and stratification, as well as in
predicting disease course and treatment response.
Chronic inflammatory arthritides comprise a heterogene- The main challenges in biomedicine and transla-
Fibroblast-like synoviocytes
(FLSs). Also known as type B ous group of diseases that are characterized by inflamma- tional research in RA are early diagnosis, personalized
synovial lining cells, FLSs tion of the synovium, which is often accompanied by the medicine and the development of meaningful outcome
account for the majority of destruction of adjacent cartilage and bone. Inflammation assessments7. A logical hypothesis is that each of these
cells in the synovial lining layer. is characterized by synovial neovascularization, stromal aims can be facilitated by the identification and devel-
proliferation and leukocyte extravasation1. For the pur- opment of appropriate biomarkers. However, although
pose of this Review, we focus on rheumatoid arthritis peripheral blood biomarkers such as rheumatoid factor
(RA), owing to its prevalence and the fact that this dis- and anti-citrullinated protein antibodies (ACPAs) have
ease is the most extensively studied and most common been shown to be relatively specific and might predict the
cause of synovitis. RA is usually persistent and progres- development of RA in asymptomatic individuals8, they
sive, and leads to joint damage, disability and deformity if are reportedly found in only 70–80% of patients with
left untreated. The disease is associated with a reduction RA9. Indeed, beyond rheumatoid factor and ACPAs, our
in quality of life, as well as with decreased longevity, and repertoire of blood biomarkers to assist with diagnosis
represents an important burden on health care spending2–4. and to provide insights into disease progression and
Within the past two decades, several considerable response to therapy is currently extremely limited10,11.
1
Centre for Arthritis and advances have been made in the treatment of inflamma- As the synovium is the principal target of inflamma-
Rheumatic Disease, tory arthritides in general, and particularly in the treat- tion in RA, and the resident fibroblast-like synoviocytes
University College Dublin, ment of RA. However, further progress is needed. The (FLSs) are implicated in the pathogenesis of synovitis, one
Dublin Academic Medical
patterns of clinical response to treatment are remarkably promising approach could be to search for biomarkers in
Centre, St. Vincent’s
University Hospital, Elm Park, similar for agents with different targets, and this finding inflamed synovial tissue. Using a combination of estab-
Dublin 4, Ireland. challenges our current understanding of disease mecha- lished methodologies, together with new high-throughput
Correspondence to D.J.V. nisms. In addition, despite the aforementioned unprece- omics technologies that have the capability to examine the
douglas.veale@ucd.ie dented progress, a substantial proportion of patients with expression of genes and their products on a scale never
doi:10.1038/nrrheum.2017.115 RA still do not achieve a state of low disease activity or before possible (BOX 1), a new opportunity awaits in the
Published online 13 Jul 2017 remission following treatment5,6. search for these biomarkers. This Review summarizes
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 1
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Key points how synovial tissue research has advanced our under-
standing of RA, contributed to progress in addressing
• Synovial tissue is the target tissue for autoimmune arthritides such as rheumatoid key challenges in the field and identified candidate bio-
arthritis. markers (TABLE 1). We first briefly discuss the anatomy
• Synovial biopsy is a safe and well-tolerated procedure that is becoming more widely and physiology of the healthy synovial joint, the main
available. changes that occur in the inflamed joint, and current
• There is a significant body of work from the past 30 years analysing the cellular and approaches to biopsy retrieval and analysis.
molecular changes in synovial tissue from patients with rheumatoid arthritis to
identify specific biomarkers. Synovial joint anatomy and physiology
• Technological advances in molecular and cellular analysis now provide new The synovial joint comprises opposing bones with artic-
opportunities for defining new biomarkers and targets. ular surfaces that are covered by cartilage. The main
protein in bone is type I collagen, whereas cartilage com-
prises mainly type II collagen and proteoglycan mole-
cules. The non-articulating surfaces of synovial joints
Author addresses are lined by a thin adventitious layer known as the syn-
1
Centre for Arthritis and Rheumatic Disease, University College Dublin, Dublin
ovium. Normal synovial tissue comprises one to three
Academic Medical Centre, St. Vincent’s University Hospital, Elm Park, Dublin 4, layers of specialized columnar FLSs that are interspersed
Ireland. with macrophages12. The entire structure is enclosed by
2
Instituto de Medicina Molecular, Faculdade de Medicina da Universidade de Lisboa, a fibrous capsule and, together with ligaments, muscles
Av. Prof. Egas Moniz, 1649–035, Lisbon, Portugal. and tendons, the fibrous capsule confers strength and
3
University of California San Diego School of Medicine, 9500 Gilman Drive, La Jolla, stability to the joint.
California 92093, USA. Several factors contribute to the maintenance of
4
Leeds Musculoskeletal Biomedical Research Unit, University of Leeds, Chapel Allerton normal homeostasis in the synovial joint, including the
Hospital, Chapeltown Road, Leeds LS7 4SA, UK. expression of the protective lubricin13, the secretion of
5
Rheumatology Research Group, University of Birmingham, Edgbaston, Birmingham matrix metalloproteinases (MMPs) by FLSs, the immune
B15 2TT, UK. sentinel roles of resident macrophages and FLSs, the reg-
6
Arthritis Unit, Rheumatology Department, Hospital Clínic, IDIBAPS, Villarroel 170, ulated entry and exit of leukocytes involved in immune
08036 Barcelona, Spain. surveillance, and local regulation by cytokines and
7
Rheumatology Unit, Department of Medicine (Solna), Karolinska Institute and growth factors.
Karolinska University Hospital, 171 76 Stockholm, Sweden. Cytokines and growth factors are important regula-
8
Cardiff University School of Medicine, Institute of Infection and Immunity, 1 st Floor, tors of FLSs and chondrocytes14–16. Cytokines are catego-
Tenovus Building, Heath Park, Cardiff CF14 4XN, UK. rized as either pro-inflammatory or anti-inflammatory
9
Department of Molecular Rheumatology, Trinity College Dublin, University of Dublin, depending on their immediate effects on specific tissues,
College Green, Dublin 2, Ireland. although considerable potential exists for pleiotropism
10
Department of Clinical Immunology & Rheumatology, Amsterdam Rheumatology depending on the cells targeted and the microenviron-
and Immunology Centre, Academic Medical Centre, University of Amsterdam, ment. Cytokines and growth factors are ubiquitous in the
Room F4‑105, PO Box 22700, 1100 DE, Amsterdam, Netherlands. synovium and synovial space, and originate either from
11
Clinical Unit Cambridge, GlaxoSmithKline, Cambridge, UK. the plasma or from FLSs, chondrocytes and cells in the
12
Centre for Experimental Medicine and Rheumatology, John Vane Science Centre, surrounding tissues16.
William Harvey Research Institute, Barts and the London School of Medicine and The joint is a dynamic environment that is subject to
Dentistry, Queen Mary University of London, Charterhouse Square, London minor trauma continually — owing to movement and,
EC1M 6BQ, UK. in some joints, compression due to weight bearing —
13
Institute of Cellular Medicine, Faculty of Medical Sciences, Newcastle University, and is therefore subject to continued wound healing and
Framlington Place, Newcastle upon Tyne NE2 4HH, UK. repair processes. Continual remodelling of the articular
14
Department of Medicine, Svendborg Hospital, Odense University Hospital, cartilage and adjacent bone is therefore necessary, and
Valdemarsgade 53, 5700 Svendborg, Denmark. this process requires a balance of anabolic and catabolic
15
Université catholique de Louvain and Department of Rheumatology, Cliniques enzyme activity in both cartilage and bone. Carefully
Universitaires Saint-Luc, Avenue Hippocrate 10, 1200 Bruxelles, Belgium. regulated proteolytic enzymes are responsible for main-
16
Rheumatology Unit, Nantes University Hospital, Hôtel-Dieu, 1 place Alexis-Ricordeau, taining the balance between anabolic and catabolic pro-
44093 Nantes cedex 1, France. cesses within the joint and cartilage17. The collagenases
17
Rheumatology and Translational Immunology Research Laboratories (LaRIT), MMP1 (interstitial collagenase), MMP3 (strome-
Division of Rheumatology, IRCCS Policlinico San Matteo Foundation/University of lysin‑1), MMP8 (neutrophil collagenase), MMP13
Pavia, P.le Golgi 19, 27100 Pavia, Italy.
(collagenase 3) and MMP18 (also known as MMP19)
18
Institute of Infection, Immunity and Inflammation, College of Medicine, are the most important of these enzymes, as they are the
Veterinary and Life Sciences, University of Glasgow, 120 University Avenue,
only known enzymes that can directly cleave collagen at
Glasgow G12 8TA, UK.
a neutral pH18, but other MMPs contribute to collagen
19
Rheumatology, Flinders University, GPO Box 2100, Adelaide 5001, South Australia,
degradation once its triple helix structure has become
Australia.
unravelled19.
20
GlaxoSmithKline, Cambridge, UK.
Serine and cysteine proteinases are required to acti-
21
Institute for Molecular Life Sciences, RadboudUMC, Theodoor Craanenlaan 11,
vate pro-MMPs (that is, MMP precursors) after they are
Nijmegen 6525 GA, Netherlands.
secreted. Furthermore, inhibitors of these proteinases
2 | ADVANCE ONLINE PUBLICATION www.nature.com/nrrheum
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Box 1 | Synovial tissue research and the omics approach Angiogenesis accompanies this immune cell accumu-
lation, but it occurs in an abnormal manner that results
The widespread availability of synovial tissue biopsy procedures and analytical methods in different patterns of blood vessels in different inflam-
throughout the world52 will inevitably enable a targeted approach to the identification matory arthropathies25. The new blood vessels seem to
of synovial biomarkers. The advent of new proteomic, transcriptomic and genomic be in an immature state26. They permit increased leuko-
technologies, and the ability to combine clinical and radiological markers with these
cyte migration, and the synovial tissue transforms into
technologies, will facilitate progress in this area. The omics approach has been usefully
applied to the identification of key players and protein interactions in several diseases. an invading pannus that can cause cartilage and bone
Studying the genome, RNA expression or protein expression each have different biases, destruction27,28. Despite the increased vascular supply,
and combined approaches could arguably lead to a more accurate assessment of marked hypoxia has been demonstrated in inflamed syn-
important protagonists104. ovial membranes in vivo29. The low tissue partial oxygen
Proteomics offers the advantage that the functional units (that is, the proteins) of the pressures in inflamed synovial joint tissue are associated
cell are being studied directly, and this approach is likely to provide information that with significant increases in macroscopic synovitis scores
most accurately reflects what is actually happening in the synovium. Technologies and markers of microscopic inflammation, such as CD68+
such as SomaLogics that have the power to measure thousands of proteins in small macrophages and CD3+ T cells in the sublining, and var-
volumes of tissue have the potential to enable a more complete characterization of ious pro-inflammatory mediators (including TNF, IL‑1β,
the protein networks that underlie diseases such as rheumatoid arthritis (RA)160.
IFNγ and the chemokine macrophage inflammatory pro-
Furthermore, new technologies for protein separation, processing and identification
are expected to increase proteome coverage. In RA, the proteomics approach has so tein 3α (MIP3α; also known as CCL20)). When primary
far focused on peripheral blood mononuclear cells, serum and synovial fluid66,67,139; the synovial fluid cells are exposed in vitro to partial oxygen
possibility that the synovial tissue itself might hold the key to elucidating the pressures similar to those in inflamed joints, cell migra-
underlying disease-associated protein networks has yet to be fully exploited by tion is significantly increased, suggesting that hypoxia
proteomic studies. drives pathological changes in the synovium26.
In relation to transcriptomic analysis, microarray technology has, to date, been the Many of the pathological changes in inflamed synovial
most frequently used strategy in the field of biomarker research. This technology tissue are reflected in the synovial fluid, which has also
facilitates the identification of candidate genes that are involved in pathophysiological been studied intensively. Inflammation alters the perme-
processes. However, gene expression levels do not always predict protein levels ability of synovial tissue30; in the RA‑affected synovium,
owing to transcriptional and translational regulatory mechanisms and the activity of
the permeability to large molecules is increased, but that
protein-degradation processes17.
Microarrays contain probes for thousands of different genes, and they are suitable to small molecules (for example, urea and glucose) is
for screening large cohorts; however, the high-throughput techniques used in decreased, an effect that is attributable to a combination
transcriptomics also enable the detection of significant gene-expression differences of increased vessel permeability, cellular infiltration and
within modestly sized cohorts161. Transcriptomic analysis is already being used to synovial hyperplasia. As a result, the total protein content
examine the gene signatures of synovial tissue, and such investigation is augmented of synovial fluid is higher during inflammation than in
by the newer sequencing technologies that enable deeper transcriptional coverage the steady state. The molecular weight distribution of the
than do microarrays and that include spliced variants. Several studies have lubrication macromolecule hyaluronic acid is also altered
demonstrated that microarray technology is a useful and practical methodology for during inflammation, with a shift towards lower molecular
studying gene expression in RA, and have characterized gene-expression patterns in weight forms in RA31. In addition, rheumatoid joints show
the synovia of patients with RA (see the section of the main text entitled
increased loss of hyaluronic acid compared with healthy
‘Gene-expression profiles’)162,163.
joints, and the mean hyaluronic acid concentration is
lower in synovial fluid samples from patients with osteoar-
(such as tissue inhibitors of metalloproteinases (TIMPs) thritis (OA) or RA than in those from healthy controls32,33.
and inhibitors of serine proteinases (SERPINs)) are also Synovial fluid samples from patients with inflamma-
present in the normal joint 20. The levels and activity of tory arthritides have markedly raised cytokine concentra-
these enzymes can be monitored indirectly by measuring tions34. The role of cytokines in initiating and perpetuating
their degradation products in the synovial fluid21. the synovial inflammatory response continues to be stud-
ied intensively, and has already led to the development
Features of the inflamed joint of several useful therapeutic agents and to the identi-
The inflamed synovium has been studied at the macro- fication of further potential targets16. Changes in the
Intimal lining layer scopic, microscopic and molecular levels. The synovium cellular infiltrate of RA‑affected synovial tissue have
The lining of the synovium is the primary target of disturbed immunomodulatory long been recognized to be associated with the clinical
comprising a few cells without pathways in RA. Rheumatoid synovial tissue appears course of disease, and have been used to identify specific
a basement membrane and
which covers the nonarticular
to be macroscopically hyperplastic and hypervascular responses to conventional and biologic DMARDs35–37.
surface of the joint capsule. (FIG. 1a,b), while microscopic analysis reveals hyperplasia In summary, the synovial tissue of patients with
of the intimal lining layer (FIG. 1c) and the accumulation of inflammatory arthritides displays numerous alterations
Synovial sublining inflammatory cells (FIG. 1d), including T and B lympho- relative to healthy synovial tissue. Thus, the study of syn-
A loose connective tissue that
cytes, plasma cells, macrophages, neutrophils, mast cells, ovial tissue is crucial to improving our understanding of
lies beneath the intimal lining
of the synovium. natural killer cells and dendritic cells, in the synovial these diseases.
sublining22. Like the target organs in other autoimmune
Pannus diseases (for example, Sjögren syndrome and auto Synovial biopsy
A ‘tumour-like’ mass of immune thyroiditis), infiltrating T cells and B cells have The utility of synovial biopsy is clear; the analysis of
hyperplastic synovial tissue
that expands into the joint,
been demonstrated to form aggregates that have vary- biopsy-obtained synovial tissue samples has increased
invading into bone and ing degrees of organization and the potential to produce our understanding of the pathogenesis of RA, identified
cartilage. disease-specific ACPAs23,24. potential therapeutic targets, and enabled the evaluation
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 3
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
Table 1 | Areas in which synovial tissue research has provided insights into rheumatoid arthritis
Research areas Examples of key findings Refs
Pathogenesis of RA Fibroblast-like synoviocytes in RA‑affected joints have a distinct DNA methylation pattern, and express 77
genes involved in the JAK–STAT pathway and HOX genes
CD68+ macrophages are central effector cells in RA 118
CD3+CD45RO+ TH17 cells are pivotal in RA 72
CD20 CD22 B cells produce antibodies and cooperate with T cells in RA
+ +
23
Synovial biomarkers of early JNK activation is increased in early RA but not in undifferentiated arthritis 101
arthritis
Synovial CD22 and CD38 expression distinguishes patients with RA from those with non‑RA disease 99
Synovial biomarkers that Numbers of CD68+ macrophages, CCR7+ T cells and CD20+CD22+ B cells correlate with 116,121,136
correlate with treatment treatment-induced changes in disease activity
response and disease
severity Levels of ICAM1, MMP1 and OPG correlate with treatment response 40,48,57
Levels of S100A8, S100A9 and S100A12 correlate with the severity of joint erosion 139
TIE2 expression is higher in erosive disease than in self-limiting disease 100
Synovial biomarkers of RA Reduced numbers of CD68+ macrophages are found in patients in remission 121
remission
CCR7, CC‑chemokine receptor 7; HOX, homeobox; ICAM1, intercellular adhesion molecule 1; JAK, Janus kinase; JNK, JUN N‑terminal kinase; MMP1, matrix
metalloproteinase 1; OPG, osteoprotegerin; RA, rheumatoid arthritis; STAT, signal transducer and activator of transcription; TIE2, tyrosine kinase with Ig and EGF
homology domains 2; TH17, T helper 17.
of current and new treatments35–57. Synovial tissue ana inflammation might be differentially expressed in differ-
lysis might also provide insights into the mechanism ent parts of the same joint, particularly in the cartilage–
of action of a given agent 58. This section discusses how pannus junction (CPJ) versus non-CPJ sites, which are
synovial biopsy and analysis are carried out, and sum- known to behave differently 61. However, the numbers of
marizes the main areas in which synovial tissue analysis T cells62,63 and plasma cells63, and the expression levels
has proven informative. of several MMPs63 and granzymes63, are reported to be
similar in biopsy samples from CPJ and non-CPJ sources.
Retrieving synovial tissue samples One study did find a difference for macrophages64,
Synovial tissue can be obtained by needle biopsy, but other studies did not replicate this finding 62,63.
arthroplasty, arthroscopic biopsy, or using ultrasound to Studies examining the optimal number of synovial tis-
guide the biopsy needle or grasping forceps58 (FIG. 2). sue specimens required for reproducible research stud-
Arthroscopic biopsy enables the direct visualization ies suggest that at least six biopsy specimens should be
of the synovium, and the operator can select an area of obtained58,65.
synovium to biopsy. By contrast, ultrasonography ena- Although immunohistochemical analysis of syn-
bles the indirect visualization of synovial thickness, and ovial tissue (FIG. 3) has a minor clinical role in the dif-
synovial vascularity can simultaneously be assessed ferential diagnosis of arthritis (for example, infectious,
by Doppler ultrasonography when selecting a suitable granulomatous, infiltrative diseases or crystal arthrop-
biopsy site. Although blind biopsy has been validated, athies), the identification of biomarkers that could be
arthroscopic biopsy and ultrasound-guided biopsy pro- used for diagnosis or for predicting disease progression
cedures are favoured by the majority of investigators and response to treatment remains an unmet challenge.
for proof‑of‑concept experiments, as sampling is more Therefore, studies of the synovium have expanded
specific for synovial tissue than connective tissue using beyond immunohistochemistry to involve methods of
these methods52. tissue digestion, homogenization and whole-tissue cul-
Arthroscopic and ultrasound-guided biopsy pro- ture (FIG. 4). Methods of examining synovial tissue at a
cedures are safe and well-tolerated. Data from 15,682 molecular level include detailed omics technologies
arthroscopies performed by rheumatologists revealed (BOX 1). For such analysis, the synovial tissue obtained
a complication rate of 0.9% for haemarthrosis, 0.2% for from the joint is placed on saline-dampened gauze,
deep vein thrombosis, and 0.1% for both wound infec- snap-frozen in the cryoprotective optimal cutting tem-
tion and joint infection59. These data were reproducible perature (OCT) compound or placed directly into an
at other centres, and the overall complication rate was less RNA-stablizing solution (such as RNAlater).
than 0.3%. Similarly, a systematic review reported an over- Synovial fluid samples are centrifuged, and a cell pel-
Arthroplasty all major complication rate of 0.4% for ultrasound-guided let can be isolated or separated using a Ficoll gradient to
Surgical reconstruction or biopsy procedures60. provide synovial fluid mononuclear cells. Several prog-
replacement of a synovial joint. nostic biomarkers of RA have been identified in synovial
Synovial tissue analysis fluid and validated in serum samples66. Studies using this
Arthroscopic biopsy
Minimally invasive procedure
Questions remain about the best location from which strategy first identified proteins that were of potential
to examine a synovial joint to obtain a biopsy sample within a given joint. In par- interest in the synovial fluid, and then searched for anti-
using an endoscope. ticular, concerns have been raised that mediators of bodies to these proteins in the plasma67. The approach of
4 | ADVANCE ONLINE PUBLICATION www.nature.com/nrrheum
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
a b effect72. Indeed, studies of synovial fluid and synovial tis-
sue from patients with RA have shown an enrichment of
so‑called ex-TH17 cells at the site of inflammation73. This
finding might explain the failure of anti‑IL‑17 therapy
in some patients as the differentiated T cells no longer
produce IL‑17. Further emphasizing the importance of
direct synovial tissue analysis is the fact that no circulat-
ing biomarkers have yet been identified that can provide
a readout of the activity of the primary invasive cells in
RA, the FLSs74.
Synovial tissue analysis has also revealed some sur-
c d prising findings regarding pathogenic mechanisms
involved in RA. One study of paired biopsy samples
taken from the inflamed knee joint and an inflamed
small joint of patients with RA demonstrated similar
mean cell numbers for all markers investigated in the
synovial sublinings of both tissues75. Of further note,
patients with clinically evident disease that manifests at
small joints have been shown to have similar — albeit
less pronounced — abnormalities in clinically unin-
volved knee joints64,75,76. However, hyperplasia of the
intimal lining layer seemed to depend on local pro-
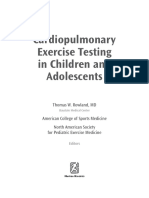
Figure 1 | The macroscopic and microscopic appearance of rheumatoid synovial cesses; different joints showed no similarity in terms
Nature Reviews | Rheumatology
tissue. Macroscopic images of synovial tissue from a patient with rheumatoid arthritis of the numbers of intimal macrophages or FLSs 64.
demonstrating inflamed and hyperplastic synovial villi (part a) and hypervascularity Consistent with these findings, in RA, the FLSs from
(part b). Representative microscopic appearance, stained with haematoxylin and eosin, different joints of the same patient show distinct DNA
demonstrating the cellular infiltrate and lining layer hyperplasia thickness (indicated by methylation and transcriptome signatures, as well as
the black line) (part c) and representative Factor VIII immunostaining of the rheumatoid differences in FLS invasiveness, depending on their
synovium demonstrating increased synovial blood vessels (part d) (original positional memory77,78.
magnifications ×10).
Early arthritis and disease stratification
Since 2002, cohorts of patients with early arthritis have
obtaining and analysing different types of samples from been gathered, and have provided clinical, histologi-
the same patient might be useful in future experiments cal, DNA-level, mRNA-level and proteomic data; such
of synovial tissue, and the results of such research might cohorts represent instrumental resources for investigat-
be more easily translated into clinical practice, as serum ing early disease79. Synovial tissue analysis is beginning
samples can be obtained in a relatively non-invasive to have an impact on our understanding of early arthritis.
manner. It is important to note that although synovial Although some progress has been made in terms of diag-
fluid might reflect the synovial compartment better than nosing RA earlier, signs of joint destruction can already
does blood, it still provides only indirect information, be present at the time of diagnosis and so developing our
and therefore studies of synovial tissue are essential68. understanding of early disease is important 80. We know
Although most research studies of synovial tissue biop- today that early, aggressive treatment is more successful
sies have involved patients with RA, which is the focus of than is delayed treatment 81,82, and a ‘window of opportu-
this Review, synovial tissue sampling might also be useful nity’ is suggested to exist, during which RA can be most
in the context of other inflammatory arthropathies such successfully treated. Therefore, the use of biomarkers to
Ex-TH17 cells as psoriatic arthritis68–71. secure a diagnosis as early as possible will enable treat-
T helper 17 (TH17) cells can ment in the most timely manner and will secure the best
switch to become ex-TH17 cells Main areas of progress outcomes83. Patients with undifferentiated arthritis might
that no longer produce IL‑17 As mentioned above, synovial tissue research has fuelled benefit most from early diagnosis. Although ACPA
but have the ability to produce
IFNγ.
progress in several key areas; these areas are summarized detection is reasonably specific (96%), the diagnos-
in TABLE 1 and discussed in more detail here. tic sensitivity of ACPAs in early arthritis is 57%81, and
Positional memory up to 30% of patients with RA never develop ACPAs,
Cells might demonstrate Insights into the pathogenesis of synovitis highlighting the need for alternative biomarkers84,85. An
different DNA ‘fingerprints’
The importance of directly analysing synovial tissue — association has been defined between the presence of
depending on the site of the
body at which they reside. the target tissue in RA — is evident from studies investi- circulating ACPAs and the subsequent development
gating the pathogenesis of RA. For example, T helper 17 of RA in individuals with arthralgia86, and of bone ero-
Undifferentiated arthritis (TH17) cells are expanded in the blood of some patients sions in patients with early untreated arthritis87. However,
Inflammatory oligoarthritis or with RA, and this finding provided the rationale for clin- a positive ACPA status in those with arthralgia is associ-
polyarthritis that does not
conform to any of the
ical trials of anti‑IL‑17 monoclonal antibodies; however, ated with the subsequent development of arthritis in only
recognized inflammatory as limited TH17 expansion occurs within the synovium 20–30% of individuals after 30 months of follow-up88,89,
arthritis types. of patients with RA, this therapeutic approach had little further emphasizing the need for additional biomarkers.
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 5
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
a b The analysis of synovial tissue samples from patients
with early RA has provided important insights. In initial
studies, the synovia of patients with early disease have
shown few molecular differences when compared with
synovia of patients with late disease23,95. However, a study
published in 2012 identified a highly expanded, specific
T cell clone in the synovia of patients with early RA,
which underlines the importance of T cells in early-stage
disease96. Another study has indicated that epigenetic
changes occurring in FLSs over time might define the
different stages of RA after clinical onset 97. Furthermore,
in a preliminary report published in 2016, synovial
tissue obtained by ultrasound-guided biopsy from
unselected treatment-naive patients with early arthri-
c d tis showed increased expression of the macrophage-
derived chemokines CXC-chemokine ligand 4 (CXCL4;
also called platelet factor 4) and CXCL7 (platelet basic
protein) only during the first 3 months of symptomatic
arthritis and not later in the disease98.
In addition to identifying potential pathogenic
mechanisms, synovial tissue biopsy might be useful for
informing differential diagnosis in early inflammatory
arthritis, as suggested by a study in which synovial CD22
and CD38 expression could distinguish patients with
RA from those with non‑RA disease99. The use of syn-
ovial biomarkers for early disease stratification was also
reported in a study of 50 patients with early arthritis who
had undergone synovial biopsy at inclusion and were
Figure 2 | Synovial tissue retrieval methods. a | NeedleNature
arthroscopy of |the
Reviews knee joint.
Rheumatology followed for 2 years100. The focus was on the angiogenic
b | Macroscopic image of synovial tissue biopsy using grasping forceps visualized by processes involved in the initiation and perpetuation of
arthroscopy. c | Ultrasound-guided biopsy. d | Representative image of an synovial inflammation, in particular vascular endothe-
ultrasonography scan. lial growth factor (VEGF) and angiopoietins 1 and 2,
and their tyrosine kinase receptors VEGFR and tyros-
ine kinase with Ig and EGF homology domains 2 (TIE2;
A delay in diagnosing RA could arise from either a also known as angiopoietin 1 receptor). The expression
lack of a definitive biomarker or a failure to meet current of TIE2 was significantly increased in the synovia of
diagnostic criteria, and these criteria have a considerable patients with erosive disease compared with the synovia
reliance on biomarkers; thus, further research into spe- of patients who had self-limiting disease, and the expres-
cific susceptibility biomarkers is warranted. Two studies sion of activated, phosphorylated TIE‑2 was significantly
published since 2015 have identified circulating bio- increased in patients with persistent non-erosive disease
markers of RA in patients who lack detectable circulat- or persistent erosive disease compared with patients
ing ACPAs; this subset of patients is an important group who had self-limiting disease. In addition, the activa-
to study, and data from these patients might contribute tion of JUN N‑terminal kinase (JNK) is elevated in the
greatly to our understanding of disease pathogenesis90,91. synovia of patients with early RA relative to the synovia
Synovial tissue analysis could be key to the identification of patients with undifferentiated arthritis, before the
of the required biomarkers. classification criteria for RA are met 101. Together, these
Cohorts of individuals who are at risk of develop- studies indicate that synovial tissue analysis can provide
ing arthritis have been the subject of much research. information relevant to disease diagnosis.
One potential corollary of such studies is the promise Only a limited number of studies have analysed syno-
of a cure for RA, or a preventive approach that could vial tissue from patients with early RA, and so the use of
detect and therapeutically target the initial breach of synovial tissue markers in early diagnosis is clearly still
self-tolerance92. The synovial tissue of patients who are evolving. Although more research is needed, these stud-
at risk of arthritis has been examined in two relatively ies suggest that a synovial biopsy at disease presentation
small studies. Little evidence of synovitis was found in could be a useful tool for both patients and physicians, as
Disease stratification the first study88, and subtle T cell infiltration was noted it could enable the stratification of early RA into short-du-
The concept that a disease in the second89. Further study of synovial tissue samples ration, self-limiting disease (which may be erosive or
can be classified into distinct from at‑risk individuals is required, as is the analysis non-erosive) versus severe, persistent and destructive
subsets that exhibit of other tissues, such as the lung and lymph nodes, inflammatory disease, thereby informing the most appro-
differential outcomes and
responses, and that can each
which might be important in the very early stages priate treatment strategy102,103. This personalized medicine
be labelled by a biomarker or of arthritis as they are the first sites at which antigen approach tailors treatment on the basis of biomarkers
a combination of biomarkers. is presented93,94. and so‑called ‘disease signatures’ (REF. 98), which enable
6 | ADVANCE ONLINE PUBLICATION www.nature.com/nrrheum
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
a b antirheumatic treatments112,113. In addition, the number
of lymphocyte aggregates is reported to be predictive of
the clinical response to infliximab treatment 112,114.
Positivity for lymphocyte aggregates increased the
power of a prediction model that included baseline
disease activity evaluated by 28‑joint disease activ-
ity score (DAS28), ACPA positivity and synovial TNF
expression112. Taken together, these studies suggest that
although lymphoid aggregates may not enable the strat-
ification of disease into subtypes, they might represent a
biomarker of treatment response.
Lymphocytes. Simple cell counts (or cellular infiltrates)
were recognized as RA‑associated synovial tissue bio-
markers more than 20 years ago. In a study published
Figure 3 | Synovial tissue immunostaining. Representative
Nature Reviews
images | Rheumatology
of biopsy-obtained in 1989, T cell numbers were shown to decrease after
rheumatoid synovial tissue demonstrating CD19+ B cell lymphoid aggregate (part a) and at least 6 months of gold treatment, and the ratio of TH
CD3+ T cells (part b). Original magnifications ×10.
cells to suppressor T cells or cytotoxic T cells was found
to be reduced in patients who were treated successfully 35.
disease stratification104,105. The sensitivity and specificity Furthermore, the number of biopsy samples in which
of disease stratification could theoretically be improved B cells could be identified decreased from 36% before
by using a combination of biomarkers. For example, a successful treatment to 7% after treatment 35.
positive clinical response of RA to anti-TNF treat- Further evidence that the abundance of synovial lym-
ment with etanercept has been predicted using a bio- phocytes (as assessed by staining for cell markers) rep-
marker signature comprising 13 autoantibodies and 11 resents a biomarker of treatment response comes from
cytokines. This study included three ethnically distinct studies of the following RA therapies: 16 weeks of metho
populations, and for North Americans it demonstrated a trexate, which caused a decrease in the synovial expres-
positive predictive value of 71%, although independent sion of markers of T cells (CD3 and CD8) and plasma
validation is required11. cells (CD38)115; 4 weeks of infliximab, which reduced
Disease stratification is important as therapies are synovial CD3+ T cell numbers in patients showing a clin-
commonly selected on a trial-and-error basis but less ical response38; 2 weeks of infliximab, which reduced the
than 50% of patients with RA experience a 50% improve- numbers of synovial CD3+ T cells and CD22+ B cells44;
ment in their arthritis in response to any single biologic 2 weeks of prednisolone, which reduced the numbers of
therapy 106–108. In the time that an ineffective treatment is synovial CD4+ T cells, CD5+ B cells and CD38+ plasma
administered, the disease might progress, and patients cells, as well as the number of CD55+ FLSs41; and various
could potentially experience unnecessary adverse events. durations of rituximab treatment, which partially but
Therefore, biomarkers that predict response to a given not invariably depleted synovial B cells, with reductions
treatment will be of great clinical utility. Synovial bio- in T cells and CD68+ macrophage numbers53,116,117. The
markers are likely to be of the greatest clinical utility, changes in CD68+ macrophage numbers after rituximab
and a great deal of work has concentrated on studying treatment have been replicated independently in another
features of the inflamed, RA‑affected synovium before centre118. By contrast, one other group showed reduc-
and after treatment. Examples of such studies, and others tions in B cell numbers with minimal or no change in
that have analysed the ability of synovial tissue biomark- macrophages and T cells119; this variation in findings is
ers to predict disease prognosis and response to therapy, possibly explained by differences in patient populations,
are summarized in the next section. methods for immunohistochemistry or analysis such as
digital image analysis.
Different types of synovial biomarker
Lymphocyte aggregates. A detailed discussion of lym- Macrophages. Although macrophages were not included
phocyte aggregates is beyond the scope of this Review, in the 1989 study described at the start of the previous
and the topic has recently been discussed in detail else- section35, the most convincing evidence for a cellular
where109; however, we wish to briefly highlight the poten- biomarker of treatment response points to the macro
tial biomarker role of these structures here. A number of phage marker CD68. This evidence comes from many
studies have addressed whether lymphocyte aggregates studies, including those of patients receiving the fol-
of synovitis are associated with clinical phenotype or the lowing RA therapies: 2 weeks of prednisolone, which
development of persistent, erosive disease. In two large reduced CD68+ macrophage abundance in the synovial
studies, lymphocyte aggregates were found in approxi- sublining 41; 12 weeks of gold therapy, which was associ-
mately 30% of patients with established RA but did not ated with an abundance of changes in all synovial layers
associate with a clinical phenotype110,111. Similarly, the independently of the site of synovial biopsy 120; various
presence of lymphocyte aggregates in patients with early durations of treatment with methotrexate or gold121, for
arthritis did not predict an aggressive disease course, which the reduction in CD68+ macrophage numbers
and aggregates were rapidly diminished by several in the synovial sublining was particularly pronounced
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 7
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
a b and sublining macrophages after active treatment,
including rituximab124; in addition, it has been shown
that DAS28 is more susceptible to placebo effects than
synovial CD68 expression125. Therefore, while we do not
propose to focus on synovial biomarkers without clin-
ical assessment, using this biomarker has been shown
to be less susceptible to the placebo effect and expec-
tation bias123,125. This work has led to the development
of a simple decision tree to inform ‘go/no‑go’ deci-
sion-making in drug development, which incorporates
clinical assessment, mechanism of action and synovial
CD68 expression and has been used in the evaluation of
numerous compounds since its proposal51. In a ballot at
c d the Outcome Measures in Rheumatology (OMERACT)
9 conference general assembly in 2008, 59% of the del-
egates agreed that CD68 expression in synovial tissue
is less susceptible to a placebo effect and expectation
bias than clinical evaluation, compared with 13% who
disagreed118.Therefore, substantial evidence exists to sug-
gest that synovial CD68 expression in synovial sublining
macrophages demonstrates validity, reliability and feasi-
bility as a biomarker of disease activity and could there-
fore be used to assess the therapeutic efficacy of novel
treatments118,123,125,126. All of these studies have used the
same standardized techniques of immunohistochemistry,
which have been extensively validated across multiple
EULAR European Synovitis Study Group centres118.
Figure 4 | Ex vivo synovial tissue culture viability. To establish ex vivo rheumatoid By contrast, three studies from the same centre
synovial biopsies, whole synovial tissue can be transferred Nature Reviews
directly | Rheumatology
from the biopsy
reported minimal or no change in macrophage cells,
forceps to culture medium. Synovial tissue can be maintained in culture for up to 72 h
and remains viable during this time. a | Representative photomicrographs of synovial possibly owing to the use of different methology; in
tissue, after 72 h in culture, stained with fluorescent calcein green indicating viable cell studies of rituximab119, abatacept 127 and, more recently,
nuclei (white arrows). b | Viable blood vessels in cultured synovial tissue (white arrow). the signal transducer and activator of transcription
c,d | Representative photomicrographs of synovial tissue, after 72 h in culture, embedded (STAT) inhibitor tofacitinib128 some reduction in sub-
in optimal cutting temperature (OCT) compound and stained with haematoxylin and lining macrophages was apparent but this reduction was
eosin to demonstrate the intact structural morphology of the synovial tissue: intact lining not statistically significant. A proof‑of‑concept study of
layer, sublining layer and blood vessels (black arrows). Original magnifications ×10. a CC-chemokine receptor 1 (CCR1) antagonist, used at
high doses to achieve high levels of receptor occupancy,
in those who showed a clinical response according to did show a reduction in macrophages, CCR1+ cells and
ACR criteria; 16 weeks of treatment with leflunomide a trend towards clinical response129. Additionally, in
or methotrexate, which were specifically associated the single study in which similarly high levels of CCR1
with abundance changes in the synovial sublining and receptor occupancy were achieved there was clear evi-
the intimal lining layer, respectively 40; various durations dence of clinical efficacy 130, supporting the predictive
of infliximab treatment, which reduced CD68+ macro value of this approach.
phage numbers in the synovial sublining 44,122; anakinra,
over 24 weeks, which reduced the size of the intimal Cytokines. As mentioned in the ‘Features of the inflamed
CD68+ macrophage population42; and various durations joint’ section, the increased expression of several
of rituximab treatment, which reduced the abundance cytokines in inflamed synovial tissue is well established.
of intimal lining CD68+ macrophages in responders53. Indeed, synovial TNF and IL‑6 concentrations correlate
One study has systematically investigated the utility with disease activity, independently of disease duration26.
of synovial sublining-localized CD68+ macrophages With regards to the effects of treatment on cytokines,
as a candidate biomarker across different interven- the expression levels of IL‑1β and TNF were 40% (95% CI
tions and kinetics, and found that changes in the num- 18–56%) and 52% (95% CI 10–74%) lower, respectively,
bers of these cells correlate with clinical improvement following prednisolone therapy compared with placebo
independently of the therapeutic strategy; the number treatment 41. Notably, this effect was mainly attributable
of CD68+ macrophages decreased as disease activity to changes in the synovial sublining, and seemed to cor-
reduced (as measured by DAS28), thus demonstrating relate with clinical improvement41. Significant changes in
that such cell counts could be used as a biomarker of cytokine expression have also been reported in the syno-
therapeutic response123. This finding was confirmed in vial lining, perivascular tissue and connective tissue after
a multicentre study that reported excellent intercentre 12 weeks of gold treatment35. In the intimal lining layer, the
agreement 118. Furthermore, the sensitivity to change levels of IL‑1α, IL‑1β and IL‑6 were significantly reduced
of synovial CD68 expression is good for both DAS28 after treatment, and this reduction seemed to correlate
8 | ADVANCE ONLINE PUBLICATION www.nature.com/nrrheum
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
with clinical response. TNF was also reduced in all three expression, suggesting that targeting CCR1 results in
areas, but the reduction in the synovial lining was not sta- changes that could also represent biomarkers of response
tistically significant35. In another study, TNF levels were to this antagonist 129.
only slightly reduced in synovial samples from patients
who received 16 weeks of treatment with either metho- S100 proteins. Similarly to some cytokines and chemok-
trexate or leflunomide40. IL‑1β levels were only moder- ines, the S100 protein family — which comprises closely
ately reduced in the leflunomide-treated patients, whereas related, low-molecular-weight (9–14 kDa) acidic calci-
reductions in the methotrexate-treated patients were um-binding proteins — have pro-inflammatory effects,
significant, which potentially reflects the different mech- and they are overexpressed in inflammatory compart-
anisms of action of these DMARDs40. Another study has ments. S100 proteins are involved in calcium-dependent
also reported that the expression of IL‑1β (but not that cell activities such as cytoskeleton regulation, and cell
of IL‑1α) is significantly reduced after 16 weeks of treat- migration and adhesion, and they also have extracellu-
ment with methotrexate and found that this reduction lar roles136. S100A8 (also known as MRP8) and S100A9
correlated with clinical response115. (also known as MRP14) regulate myeloid cell function
As highlighted above, targeting cytokine signal- and control inflammation137, and S100A12 (also known
ling pathways, for example the STAT pathway, is an as MRP6) has important activities in relation to innate
interesting and novel approach. Tofacitinib has shown and acquired immune responses138. One study using
significant clinical benefit in patients with RA and is quantitative proteomics demonstrated an association
associated with a significant reduction in expression of between the severity of joint erosion in RA and the levels
phosphorylated STAT in synovial tissue, which suggests of S100A8, S100A9 and S100A12 in both synovial fluid
that the level of phosphorylated STAT could be a useful and serum samples139; this potential role of S100 proteins
biomarker of response to this therapy128. Although not as synovial biomarkers requires further study.
itself a cytokine, acute serum amyloid A (A‑SAA) regu-
lates the expression of cytokines and is expressed in RA Adhesion molecules. The expression of intercellular
synovial tissue, where it has a role in inducing angio adhesion molecule 1 (ICAM1) is significantly reduced
genesis, cell–matrix interactions, and the expression of in patients with RA who are treated with either lefluno-
chemokines and MMPs 131. Furthermore, blockade mide or methotrexate40. Notably, the significant decrease
of the A‑SAA receptors scavenger receptor class B mem- in ICAM1 expression was seen only in those who
ber 1 (SRB1)131 and Toll-like receptor 2 (TLR2) inhibits responded to treatment. The expression of vascular cell
FLS migration and invasion in synovial explants from adhesion molecular 1 (VCAM1) was reduced in both
patients with RA132. Importantly, baseline serum A‑SAA treatment groups, but this reduction was significant only
levels independently correlate with the 28‑joint swol- in the leflunomide-treated patients40.
len joint count and 1‑year radiographic progression in Another study demonstrated that the expression of
patients with RA20. Therefore, serum A‑SAA is a prom- VCAM1 and E‑selectin was significantly reduced after
ising biomarker of disease activity, warranting further 16 weeks of treatment with methotrexate, but in this
investigation of its expression in the synovia of patients study the changes in ICAM1 expression did not reach
with RA133. statistical significance115. Similarly, treatment with inflix-
imab has been shown to reduce VCAM‑1 and E‑selectin
Chemokines. Leukocytes are attracted to target tissues expression in repeat biopsies taken 4 weeks after treat-
by soluble chemotactic cytokines termed chemokines, ment38. Interestingly, the effect of anakinra might be dose-
which are released from activated cells in the tissue to dependent, as patients taking a dose of 150 mg per day — but
stimulate leukocyte migration through the endothe- not those receiving a lower dose of 30 mg per day — were
lial barrier 134. The chemokine monocyte chemotactic shown to have reduced synovial expression of E‑selectin,
protein 1 (MCP1; also known as CCL2), among others, ICAM1 and VCAM1 (REF. 42). Together, these stud-
is expressed abundantly in both serum and synovial ies highlight the biomarker role of synovial adhesion
tissue samples from patients with RA49. The develop- molecule expression.
ment of clinical signs of synovial inflammation in RA
is specifically associated with the increased synthesis of Mediators and products of bone, cartilage and synovial
CXCL8 (also known as IL‑8)135, and the expression tissue degradation. Serum levels of collagen biomarkers
of both CXCL8 and MCP1 in synovial tissue (both the and MMPs are known to predict radiographic progres-
lining and sublining) reflects response to therapy in sion in RA, and therefore could represent prognostic
patients with active RA who have received infliximab; biomarkers27,140, but could the synovial levels of these
the synovial expression of growth-regulated protein‑α molecules also be a biomarker?
(GROα), RANTES (also known as CCL5) and MIP1β Although MMPs are present in normal synovial
(also known as CCL4) was also reduced but not to a fluid, their concentrations are increased in synovial fluid
significant extent 44. Thus, chemokines could represent from patients with RA, psoriatic arthritis and OA17,141,142.
a target and a biomarker of treatment response. Indeed, a MMP1, in particular, might be a synovial biomarker of
=proof‑of‑concept study of an oral CCR1 antagonist treatment response, as suggested by a study reporting
in patients with RA showed a trend towards clinical that monotherapy with methotrexate or leflunomide
improvement and a concomitant, significant reduc- significantly reduced the expression of MMP1 and the
tion in synovial macrophage numbers and chemokine MMP1:TIMP1 ratio in synovial tissue samples from
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 9
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
patients with RA after 4 months of treatment 40. Notably, that 38 transcripts were associated with clinical response
the changes were more pronounced in patients who to infliximab treatment 114. A study of paired synovial
fulfilled the ACR20 response criteria40. tissue samples taken from patients with RA before and
In addition to studies of matrix-degrading MMPs, a 12 weeks after initiation of adalimumab treatment also
number of studies have analysed the effects of immuno identified genes that were differentially expressed in sam-
modulatory treatment on synovial mediators of bone ples from responders and non-responders151. These genes
destruction. Treatment with either infliximab or etaner- could be split into two distinct families: genes involved in
cept increases the expression of osteoprotegerin (OPG; the regulation of immune responses and genes involved
also known as TNFRSF11B) in synovial tissue, but had in the regulation of cell division. To confirm the micro
no effect on the expression of receptor activator of nuclear array findings, the synovial expression of selected mol-
factor‑κB ligand (RANKL; also known as TNFSF11), ecules was assessed using specific antibodies, and the
resulting in an increased OPG:RANKL ratio48. By con- expression of IL‑7 receptor α‑chain (IL‑7Rα), CXCL11,
trast, rituximab induces a 99% decrease in the numbers of IL‑18, IL‑18 receptor accessory protein (IL‑18RAP) and
receptor activator of nuclear factor‑κB (RANK)-positive the proliferation marker MKI67 was found to be sig-
osteoclast precursors and 37% decrease in RANKL nificantly higher in poor responders than in moderate
expression, but only a nonsignificant reduction in syn- and good responders. Thus, these findings link gene-
ovial OPG expression143. However, not all RA therapies expression changes to protein-level changes and, consist-
induce changes in the levels of these bone-destructive ent with studies discussed above, they emphasize the role of
mediators; indeed, abatacept does not significantly molecules involved in cytokine and chemokine signalling as
affect the synovial levels of mRNA expression of OPG, potential biomarkers of treatment response151.
RANK or RANKL127, suggesting that the biomarker role Gene-expression analyses also support the role of
of these synovial molecules might only be relevant in macrophages and T cells as biomarkers of treatment
specific settings. response. For example, a study of paired synovial biop-
sies performed in patients with RA before and after
Antigens and antibodies. The expression of antigenic initiation of rituximab treatment revealed that clinical
proteins has been described in synovial tissue samples responders demonstrated higher synovial expression
from patients with RA. For example, one study reported of macrophage-associated and T cell-associated genes,
that deiminated protein — such as the α- and β‑chains whereas those with a poor clinical response showed
of fibrin — present in RA‑affected synovia seem to be higher synovial expression of IFNα and genes associated
major antigenic targets of ACPAs144. In addition, anti‑Sa with matrix remodelling 152.
antibodies that recognize deiminated vimentin have
been isolated from RA‑affected synovia and seem to be Challenges in biomarker identification
specific to RA145. Intracellular citrullinated proteins that Most studies of serial synovial biopsies have been per-
colocalize with ACPA reactivity have also been identified formed on patients with known diagnoses and have aimed
in synovial tissue from patients with RA146, but the pres- to investigate response to treatment. There remains a crit-
ence of citrullinated antigens in synovia is not specific ical need to identify diagnostic biomarkers that can be
to RA24. Finally, anti-fillagrin antibodies are produced by used in clinical practice. Biomarkers could reduce the time
local plasma cells that are resident in the RA pannus147, taken and patient numbers required to evaluate the poten-
and thus could also be synovial biomarkers of RA. tial efficacy of new drugs51,153. The number of patients with
active disease who are eligible to participate in studies is
Gene-expression profiles. Most of the previous discus- limited. As with all trials, the number of patients who are
sion has focused on protein-level data, predominantly to be put at risk by exposure to drugs at an early stage of
from immunohistochemical analyses; however, as men- drug development, as well as to be placed on placebo, are
tioned above and discussed in BOX 1, studies have also restricted by ethical considerations154.
identified changes in synovial gene-expression profiles, Although finding biomarkers in peripheral blood is
and these profiles could represent biomarkers. An exam- attractive because obtaining blood samples is more feasible
ple of how transcriptomic data can be clinically useful and less invasive than synovial biopsy, the inflamed syn-
comes from a study that used these data to create a rule- ovium is the ultimate target of inflammation and should
based classification that could differentiate between RA thus be a rich source of potential biomarkers. Furthermore,
and OA148. In addition, gene-expression variance among many confounding factors might interfere with periph-
patients with RA has been described for genes involved eral blood profiles. Some authorities have suggested that
in processes such as cell proliferation, cell survival, a more targeted approach to searching for serum markers
angiogenesis and the regulation of inflammation149. should first involve the identification of potential biomark-
Several studies have investigated links between ers in the inflamed synovial joint, and then the study of
gene-expression profiles and treatment response; for these biomarkers in the serum155. Such an approach has
example, genes involved in inflammation shown to be demonstrated clinical utility in patients with RA in a study
upregulated in pretreatment biopsy-obtained synovial reporting that candidate peripheral biomarkers of synovial
tissue from patients with RA who subsequently responded pathotype predicted response to biologic therapy156.
to anti-TNF therapy 150. In a larger follow‑up study, RNA New technologies are advancing synovial tissue ana
analysis of pretreatment synovial tissue from patients with lysis, but several issues remain to be addressed. Although
RA who were positive for lymphocyte aggregates revealed new technologies have enabled faster and more complete
10 | ADVANCE ONLINE PUBLICATION www.nature.com/nrrheum
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
analyses of proteins, the high complexity of proteins and from this emerging field. Future progress in identifying
protein isoforms in the synovial joint makes the inter- genomic biomarkers, and other types of biomarker, will
pretation of ‘shotgun’ proteomic data challenging. The probably be fuelled by synovial tissue analysis, which has
interpretation of data from microarrays is also problem- not yet been extensively performed in some areas; for
atic; for example, three widely used microarray platforms example, although many studies have attempted to iden-
have demonstrated poor reproducibility 157. In addition, tify gene-expression profiles that can predict response to
as array datasets contain high levels of background sig- anti-TNF treatment, to our knowledge only those reported
nals, they have decreased sensitivity to transcripts that above have used synovial tissue to search for these112,114,151.
are present in low numbers158.
Cost and time are also important issues; for exam- Conclusions
ple, the development of high-quality immunoanalytical Synovial tissue represents the target tissue of auto
assays can be slow and expensive, which limits the ver- immune arthritides such as RA. New, safe methods of
ification of candidate biomarkers, despite the increase obtaining samples of synovial tissue are becoming more
in the availability of means to biopsy synovial tissue. In widely available. In this Review we have highlighted
addition, when data from control synovial tissue speci- those studies that analyse the cellular and molecular
mens is available, OA is often used as a disease control, characteristics of RA synovial tissue and how the results
although it is increasingly recognized that OA has an have advanced the field in terms of patient stratifica-
underlying inflammatory response, albeit one that is lim- tion, therapeutic target development and identification
ited and less associated with specific autoimmunity than of biomarkers of response to therapy. In addition, we
is the response that underlies RA159. These issues perhaps have reviewed the use of synovial tissue analysis as an
explain why although a great many genomic biomarkers outcome measure for clinical trials in RA. Finally, the
exist that can predict response to treatment or who is most future application of rapid advances in molecular tech-
at risk of adverse events in many areas of medicine, rheu- nologies to synovial tissue analysis will probably lead to
matology seems to have experienced only limited benefit major benefits for patients with RA.
1. Tak, P. P. & Bresnihan, B. The pathogenesis and 14. Hyc, A., Osiecka-Iwan, A., Niderla-Bielinska, J., 27. Mullan, R. H. et al. Early changes in serum type II
prevention of joint damage in rheumatoid arthritis: Jankowska-Steifer, E. & Moskalewski, S. Pro-and anti- collagen biomarkers predict radiographic progression
advances from synovial biopsy and tissue analysis. inflammatory cytokines increase hyaluronan at one year in inflammatory arthritis patients after
Arthritis Rheum. 43, 2619–2633 (2000). production by rat synovial membrane in vitro. Int. biologic therapy. Arthritis Rheum. 56, 2919–2928
2. Mitchell, D. M. et al. Survival, prognosis, and causes J. Mol. Med. 24, 579–585 (2009). (2007).
of death in rheumatoid arthritis. Arthritis Rheum. 29, 15. Blewis, M. E. et al. Interactive cytokine regulation of 28. Månsson, B. et al. Cartilage and bone metabolism in
706–714 (1986). synoviocyte lubricant secretion. Tissue Eng. Part A 16, rheumatoid arthritis. Differences between rapid and
3. Pincus, T. et al. Severe functional declines, work 1329–1337 (2009). slow progression of disease identified by serum
disability, and increased mortality in seventy-five 16. McInnes, I. B. & Schett, G. Cytokines in the markers of cartilage metabolism. J. Clin. Invest. 95,
rheumatoid arthritis patients studied over nine years. pathogenesis of rheumatoid arthritis. Nat. Rev. 1071–1077 (1995).
Arthritis Rheum. 27, 864–872 (1984). Immunol. 7, 429–442 (2007). 29. Biniecka, M. et al. Oxidative damage in synovial
4. Wolfe, F., Michaud, K., Gefeller, O. & Choi, H. K. 17. Tchetverikov, I. et al. MMP protein and activity levels tissue is associated with in vivo hypoxic status in the
Predicting mortality in patients with rheumatoid in synovial fluid from patients with joint injury, arthritic joint. Ann. Rheum. Dis. 69, 1172–1178
arthritis. Arthritis Rheum. 48, 1530–1542 (2003). inflammatory arthritis, and osteoarthritis. Ann. (2010).
5. Sokka, T. et al. Remission and rheumatoid arthritis: Rheum. Dis. 64, 694–698 (2005). 30. Levick, J. R. Permeability of rheumatoid and normal
data on patients receiving usual care in twenty-four 18. Billinghurst, R. C. et al. Enhanced cleavage of type II human synovium to specific plasma proteins. Arthritis
countries. Arthritis Rheum. 58, 2642–2651 collagen by collagenases in osteoarthritic articular Rheum. 24, 1550–1560 (1981).
(2008). cartilage. J. Clin. Invest. 99, 1534–1545 (1997). 31. Dahl, L. B., Dahl, I. M., Engström-Laurent, A. &
6. Balogh, E. et al. Comparison of remission criteria in 19. Shingleton, W. D., Hodges, D. J., Brick, P. & Granath, K. Concentration and molecular weight of
a tumour necrosis factor inhibitor treated Cawston, T. E. Collagenase: a key enzyme in collagen sodium hyaluronate in synovial fluid from patients
rheumatoid arthritis longitudinal cohort: patient turnover. Biochem. Cell Biol. 74, 759–775 (1996). with rheumatoid arthritis and other arthropathies.
global health is a confounder. Arthritis Res. Ther. 15, 20. Connolly, M. et al. Acute-phase serum amyloid A Ann. Rheum. Dis. 44, 817–822 (1985).
R221 (2013). regulates tumor necrosis factor α and matrix 32. Decker, B., McKenzie, B. F., McGuckin, W. F. &
7. Fearon, U. & Veale, D. J. Key challenges in rheumatic turnover and predicts disease progression in Slocumb, C. H. Comparative distribution of proteins
and musculoskeletal disease translational research. patients with inflammatory arthritis before and after and glycoproteins of serum and synovial fluid. Arthritis
EBioMedicine 1, 95–96 (2014). biologic therapy. Arthritis Rheum. 64, 1035–1045 Rheum. 2, 162–177 (1959).
8. Hensvold, A. H. et al. How well do ACPA (2011). 33. Swann, D. A. et al. Role of hyaluronic acid in joint
discriminate and predict RA in the general 21. Lohmander, L. S., Atley, L. M., Pietka, T. A. & lubrication. Ann. Rheum. Dis. 33, 318–326
population: a study based on 12 590 population- Eyre, D. R. The release of crosslinked peptides from (1974).
representative Swedish twins. Ann. Rheum. Dis. 76, type II collagen into human synovial fluid is increased 34. Hui, A. Y., McCarty, W. J., Masuda, K.,
119–125 (2017). soon after joint injury and in osteoarthritis. Arthritis Firestein, G. S. & Sah, R. L. A systems biology
9. Rantapaa-Dahlqvist, S. et al. Antibodies against cyclic Rheum. 48, 3130–3139 (2003). approach to synovial joint lubrication in health,
citrullinated peptide and IgA rheumatoid factor 22. Tak, P. P. et al. Analysis of the synovial cell infiltrate in injury, and disease. Wiley Interdiscip. Rev. Syst. Biol.
predict the development of rheumatoid arthritis. early rheumatoid synovial tissue in relation to local Med. 4, 15–37 (2012).
Arthritis Rheum. 48, 2741–2749 (2003). disease activity. Arthritis Rheum. 40, 217–225 35. Rooney, M., Whelan, A., Feighery, C. & Bresnihan, B.
10. Choi, I. Y. et al. MRP8/14 serum levels as a strong (1997). Changes in lymphocyte infiltration of the synovial
predictor of response to biological treatments in 23. Humby, F. et al. Ectopic lymphoid structures membrane and the clinical course of rheumatoid
patients with rheumatoid arthritis. Ann. Rheum. Dis. support ongoing production of class-switched arthritis. Arthritis Rheum. 32, 361–369 (1989).
74, 499–505 (2015). autoantibodies in rheumatoid synovium. PLoS Med. 36. Firestein, G. S., Paine, M. M. & Boyle, D. L.
11. Hueber, W. et al. Blood autoantibody and cytokine 6, e1 (2009). Mechanisms of methotrexate action in rheumatoid
profiles predict response to anti-tumor necrosis factor 24. Vossenaar, E. R. et al. The presence of citrullinated arthritis. Arthritis Rheum. 37, 193–200 (1994).
therapy in rheumatoid arthritis. Arthritis Res. Ther. proteins is not specific for rheumatoid synovial tissue. 37. Tak, P. P. et al. Reduction of synovial inflammation
11, R76 (2009). Arthritis Rheum. 50, 3485–3494 (2004). after anti‑CD4 monoclonal antibody treatment in early
12. Smith, M. D. et al. Microarchitecture and protective 25. Reece, R. J., Canete, J. D., Parsons, W. J., Emery, P. rheumatoid arthritis. Arthritis Rheum. 38,
mechanisms in synovial tissue from clinically and & Veale, D. J. Distinct vascular patterns of early 1457–1465 (1995).
arthroscopically normal knee joints. Ann. Rheum. Dis. synovitis in psoriatic, reactive, and rheumatoid 38. Tak, P. P. et al. Decrease in cellularity and expression
62, 303–307 (2003). arthritis. Arthritis Rheum. 42, 1481–1484 (1999). of adhesion molecules by anti-tumor necrosis factor α
13. Rhee, D. K. et al. The secreted glycoprotein lubricin 26. Ng, C. T. et al. Synovial tissue hypoxia and monoclonal antibody treatment in patients with
protects cartilage surfaces and inhibits synovial cell inflammation in vivo. Ann. Rheum. Dis. 69, rheumatoid arthritis. Arthritis Rheum. 39,
overgrowth. J. Clin. Invest. 115, 622–631 (2005). 1389–1395 (2010). 1077–1081 (1996).
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 11
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
39. Youssef, P. P. et al. Variability in cytokine and cell 60. Lazarou, I. et al. Ultrasound-guided synovial biopsy: a 82. van der Heijde, A. et al. The effectiveness of early
adhesion molecule staining in arthroscopic synovial systematic review according to the OMERACT filter treatment with ‘second-line’ antirheumatic drugs. A
biopsies: quantification using color video image and recommendations for minimal reporting randomized, controlled trial. Ann. Intern. Med. 124,
analysis. J. Rheumatol. 24, 2291–2298 (1997). standards in clinical studies. Rheumatology (Oxford) 699–707 (1996).
40. Kraan, M. C. et al. Modulation of inflammation and 54, 1867–1875 (2015). 83. Finckh, A., Liang, M. H., van Herckenrode, C. M. & de
metalloproteinase expression in synovial tissue by 61. Youssef, P. P. et al. Quantitative microscopic analysis Pablo, P. Long-term impact of early treatment on
leflunomide and methotrexate in patients with active of inflammation in rheumatoid arthritis synovial radiographic progression in rheumatoid arthritis: a
rheumatoid arthritis: findings in a prospective, membrane samples selected at arthroscopy compared meta-analysis. Arthritis Rheum. 55, 864–872 (2006).
randomized, double-blind, parallel-design clinical trial with samples obtained blindly by needle biopsy. 84. Whiting, P. F. et al. Systematic review: accuracy of anti-
in thirty-nine. Arthritis Rheum. 43, 1820–1830 Arthritis Rheum. 41, 663–669 (1998). citrullinated peptide antibodies for diagnosing
(2000). 62. Kirkham, B. et al. Intraarticular variability of synovial rheumatoid arthritis. Ann. Intern. Med. 152, 456–466
41. Gerlag, D. M. et al. Effects of oral prednisolone on membrane histology, immunohistology, and cytokine (2010).
biomarkers in synovial tissue and clinical mRNA expression in patients with rheumatoid 85. Lee, D. M. & Schur, P. H. Clinical utility of the anti-CCP
improvement in rheumatoid arthritis. Arthritis arthritis. J. Rheumatol. 26, 777–784 (1999). assay in patients with rheumatic diseases. Ann.
Rheum. 50, 3783–3791 (2004). 63. Smeets, T. J. M. et al. Analysis of the cell infiltrate and Rheum. Dis. 62, 870–874 (2003).
42. Cunnane, G., Madigan, A., Murphy, E., FitzGerald, O. expression of matrix metalloproteinases and 86. Bos, W. H. et al. Arthritis development in patients with
& Bresnihan, B. The effects of treatment with granzyme B in paired synovial biopsy specimens from arthralgia is strongly associated with anti-citrullinated
interleukin‑1 receptor antagonist on the inflamed the cartilage–pannus junction in patients with RA. protein antibody status: a prospective cohort study.
synovial membrane in rheumatoid arthritis. Ann. Rheum. Dis. 60, 561–565 (2001). Ann. Rheum. Dis. 69, 490–494 (2010).
Rheumatology (Oxford) 40, 62–69 (2001). 64. Soden, M. et al. Immunohistological features in the 87. Nielen, M. M. J. et al. Antibodies to citrullinated
43. Catrina, A. I. et al. Anti-tumour necrosis factor (TNF)-α synovium obtained from clinically uninvolved knee human fibrinogen (ACF) have diagnostic and
therapy (etanercept) down-regulates serum matrix joints of patients with rheumatoid arthritis. prognostic value in early arthritis. Ann. Rheum. Dis.
metalloproteinase (MMP)-3 and MMP‑1 in Br. J. Rheumatol. 28, 287–292 (1989). 64, 1199–1204 (2005).
rheumatoid arthritis. Rheumatology (Oxford) 41, 65. Smith, M. D. et al. Standardisation of synovial tissue 88. de Hair, M. J. et al. Features of the synovium of
484–489 (2002). infiltrate analysis: how far have we come? How much individuals at risk of developing rheumatoid arthritis:
44. Smeets, T. J. M., Kraan, M. C., van Loon, M. E. & further do we need to go? Ann. Rheum. Dis. 65, implications for understanding preclinical rheumatoid
Tak, P. Tumor necrosis factor α blockade reduces the 93–100 (2006). arthritis. Arthritis Rheum. 66, 513–522 (2014).
synovial cell infiltrate early after initiation of 66. Mateos, J. et al. Differential protein profiling of 89. van de Sande, M. G. et al. Different stages of rheumatoid
treatment, but apparently not by induction of synovial fluid from rheumatoid arthritis and arthritis: features of the synovium in the preclinical
apoptosis in synovial tissue. Arthritis Rheum. 48, osteoarthritis patients using LC–MALDI TOF/TOF. phase. Ann. Rheum. Dis. 70, 772–777 (2011).
2155–2162 (2003). J. Proteomics 75, 2869–2878 (2012). 90. Anderson, A. E. et al. IL‑6‑driven STAT signalling in
45. Kraan, M. C. et al. Differential effects of leflunomide 67. Biswas, S. et al. Identification of novel autoantigen in circulating CD4+ lymphocytes is a marker for early
and methotrexate on cytokine production in the synovial fluid of rheumatoid arthritis patients anticitrullinated peptide antibody-negative rheumatoid
rheumatoid arthritis. Ann. Rheum. Dis. 63, using an immunoproteomics approach. PLoS ONE 8, arthritis. Ann. Rheum. Dis. 75, 466–473 (2016).
1056–1061 (2004). e56246 (2013). 91. Hensvold, A. H. et al. Serum RANKL levels associate with
46. Rooney, T. et al. Synovial tissue interleukin‑18 68. Bresnihan, B., Tak, P. P., Emery, P., Klareskog, L. & anti- citrullinated protein antibodies in early untreated
expression and the response to treatment in patients Breedveld, F. Synovial biopsy in arthritis research: five rheumatoid arthritis and are modulated following
with inflammatory arthritis. Ann. Rheum. Dis. 63, years of concerted European collaboration. Ann. methotrexate. Arthritis Res. Ther. 17, 239 (2015).
1393–1398 (2004). Rheum. Dis. 59, 506–511 (2000). 92. Gerlag, D. M., Norris, J. M. & Tak, P. P. Towards
47. van Holten, J. et al. A multicentre, randomised, 69. Kraan, M. C. et al. Alefacept treatment in psoriatic prevention of autoantibody-positive rheumatoid arthritis:
double blind, placebo controlled phase II study of arthritis: reduction of the effector T cell population in from lifestyle modification to preventive treatment.
subcutaneous interferon beta‑1a in the treatment of peripheral blood and synovial tissue is associated with Rheumatology (Oxford) 55, 607–614 (2016).
patients with active rheumatoid arthritis. Ann. Rheum. improvement of clinical signs of arthritis. Arthritis 93. Reynisdottir, G. et al. Signs of immune activation and
Dis. 64, 64–69 (2005). Rheum. 46, 2776–2784 (2002). local inflammation are present in the bronchial tissue
48. Catrina, A. I. et al. Anti-tumor necrosis factor therapy 70. Cañete, J. D. et al. Distinct synovial immunopathology of patients with untreated early rheumatoid arthritis.
increases synovial osteoprotegerin expression in in Behcet disease and psoriatic arthritis. Arthritis Res. Ann. Rheum. Dis. 75, 1722–1727 (2016).
rheumatoid arthritis. Arthritis Rheum. 54, 76–81 Ther. 11, R17 (2009). 94. van Baarsen, L. G. et al. The cellular composition of
(2006). 71. van Kuijk, A. W. & Tak, P. P. Synovitis in psoriatic lymph nodes in the earliest phase of inflammatory
49. Haringman, J. J. et al. A randomized controlled trial arthritis: immunohistochemistry, comparisons with arthritis. Ann. Rheum. Dis. 72, 1420–1424 (2013).
with an anti‑CCL2 (anti-monocyte chemotactic protein rheumatoid arthritis, and effects of therapy. Curr. 95. Baeten, D. et al. Comparative study of the synovial
1) monoclonal antibody in patients with rheumatoid Rheumatol. Rep. 13, 353–359 (2011). histology in rheumatoid arthritis, spondyloarthropathy,
arthritis. Arthritis Rheum. 54, 2387–2392 (2006). 72. Kobezda, T., Ghassemi-Nejad, S., Mikecz, K., and osteoarthritis: influence of disease duration and
50. Makrygiannakis, D. et al. Intraarticular corticosteroids Glant, T. T. & Szekanecz, Z. Of mice and men: how activity. Ann. Rheum. Dis. 59, 945–953 (2000).
decrease synovial RANKL expression in inflammatory animal models advance our understanding of T‑cell 96. Klarenbeek, P. L. et al. Inflamed target tissue provides
arthritis. Arthritis Rheum. 54, 1463–1472 (2006). function in RA. Nat. Rev. Rheumatol. 10, 160–170 a specific niche for highly expanded T‑cell clones in
51. Gerlag, D. M. & Tak, P. P. Novel approaches for the (2014). early human autoimmune disease. Ann. Rheum. Dis.
treatment of rheumatoid arthritis: lessons from the 73. Basdeo, S. A. et al. Ex‑Th17 (nonclassical Th1) cells 71, 1088–1093 (2012).
evaluation of synovial biomarkers in clinical trials. Best are functionally distinct from classical Th1 and Th17 97. Whitaker, J. W. An imprinted rheumatoid arthritis
Pract. Res. Clin. Rheumatol. 22, 311–323 (2008). cells and are not constrained by regulatory T cells. methylome signature reflects pathogenic phenotype.
52. Harty, L. C., Gerlag, D. M., Pitzalis, C., Veale, D. J. & J. Immunol. 198, 2249–2259 (2017). Genome Med. 5, 40 (2013).
Tak, P. P. Synovial tissue analysis for the discovery of 74. Firestein, G. S. & McInnes, I. B. Immunopathogenesis 98. Yeo, L. et al. Expression of chemokines CXCL4 and
diagnostic and prognostic biomarkers in patients with of rheumatoid arthritis. Immunity 46, 183–196 CXCL7 by synovial macrophages defines an early
early arthritis. J. Rheumatol. 38, 2068–2072 (2011). (2017). stage of rheumatoid arthritis. Ann. Rheum. Dis. 75,
53. Thurlings, R. M. et al. Synovial tissue response to 75. Kraan, M. C. et al. Comparison of synovial tissues 763–771 (2016).
rituximab: mechanism of action and identification from the knee joints and the small joints of 99. Kraan, M. C. et al. Immunohistological analysis of
of biomarkers of response. Ann. Rheum. Dis. 67, rheumatoid arthritis patients: implications for synovial tissue for differential diagnosis in early
917–925 (2008). pathogenesis and evaluation of treatment. Arthritis arthritis. Rheumatology (Oxford) 38, 1074–1080
54. Vergunst, C. E. et al. Modulation of CCR2 in Rheum. 46, 2034–2038 (2002). (1999).
rheumatoid arthritis: a double-blind, randomized, 76. Kraan, M. C. et al. Asymptomatic synovitis precedes 100. van de Sande, M. G. et al. Local synovial engagement
placebo-controlled clinical trial. Arthritis Rheum. 58, clinically manifest arthritis. Arthritis Rheum. 41, of angiogenic TIE‑2 is associated with the
1931–1939 (2008). 1481–1488 (1998). development of persistent erosive rheumatoid
55. van Kuijk, A. W. et al. CCR5 blockade in rheumatoid 77. Ai, R. et al. Joint-specific DNA methylation and arthritis in patients with early arthritis. Arthritis
arthritis: a randomised, double-blind, placebo- transcriptome signatures in rheumatoid arthritis Rheum. 65, 3073–3083 (2013).
controlled clinical trial. Arthritis Rheum. 54, identify distinct pathogenic processes. Nat. Commun. 101. de Launay, D. et al. Selective involvement of ERK and
2387–2392 (2006). 7, 11849 (2016). JNK mitogen-activated protein kinases in early
56. Vergunst, C. E. et al. Blocking the receptor for C5a in 78. Frank-Bertoncelj, M. et al. Epigenetically-driven rheumatoid arthritis (1987 ACR criteria compared to
patients with rheumatoid arthritis does not reduce anatomical diversity of synovial fibroblasts guides 2010 ACR/EULAR criteria): a prospective study aimed
synovial inflammation. Rheumatology (Oxford) 46, joint-specific fibroblast functions. Nat. Commun. 23, at identification of diagnostic and prognostic
1773–1778 (2007). 14852 (2017). biomarkers as well as therapeutic targets.
57. Boumans, M. J. et al. Safety, tolerability, 79. de Hair, M. J. et al. Synovial tissue analysis for the Ann. Rheum. Dis. 71, 415–423 (2012).
pharmacokinetics, pharmacodynamics and efficacy of discovery of diagnostic and prognostic biomarkers in 102. Drossaers-Bakker, K. W. et al. Long-term outcome in
the monoclonal antibody ASK8007 blocking patients with early arthritis. J. Rheumatol. 38, rheumatoid arthritis: a simple algorithm of baseline
osteopontin in patients with rheumatoid arthritis: a 2068–2072 (2011). parameters can predict radiographic damage,
randomised, placebo controlled, proof‑of‑concept 80. van der Heijde, D. M. Joint erosions and patients with disability, and disease course at 12‑year followup.
study. Ann. Rheum. Dis. 71, 180–185 (2012). early rheumatoid arthritis. Br. J. Rheumatol. 34 Arthritis Rheum. 47, 383–390 (2002).
58. Gerlag, D. & Tak, P. P. How to perform and analyse (Suppl. 2), 74–78 (1995). 103. Scott, D. L. The diagnosis and prognosis of early
synovial biopsies. Best Pract. Res. Clin. Rheumatol. 81. Lard, L. R. et al. Early versus delayed treatment in arthritis: rationale for new prognostic criteria. Arthritis
23, 221–232 (2009). patients with recent-onset rheumatoid arthritis: Rheum. 46, 286–290 (2002).
59. Kane, D., Veale, D. J., FitzGerald, O. & Reece, R. comparison of two cohorts who received different 104. Lindstrom, T. M. & Robinson, W. H. Biomarkers for
Survey of arthroscopy performed by rheumatologists. treatment strategies. Am. J. Med. 111, 446–451 rheumatoid arthritis: making it personal. Scand.
Rheumatology (Oxford) 41, 210–215 (2002). (2001). J. Clin. Lab. Investig. 70, 79–84 (2010).
12 | ADVANCE ONLINE PUBLICATION www.nature.com/nrrheum
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
REVIEWS
105. Trusheim, M. R., Berndt, E. R. & Douglas, F. L. Stratified 127. Buch, M. H. et al. Mode of action of abatacept in 148. Woetzel, D. et al. Identification of rheumatoid arthritis
medicine: strategic and economic implications of rheumatoid arthritis patients having failed tumour and osteoarthritis patients by transcriptome-based
combining drugs and clinical biomarkers. Nat. Rev. necrosis factor blockade: a histological, gene rule set generation. Arthritis Res. Ther. 16, R84
Drug Discov. 6, 287–293 (2007). expression and dynamic magnetic resonance imaging (2014).
106. Edwards, J. C. et al. Efficacy of B‑cell-targeted therapy pilot study. Ann. Rheum. Dis. 68, 1220–1227 149. Huber, R. et al. Identification of intra-group, inter-
with rituximab in patients with rheumatoid arthritis. (2009). individual, and gene-specific variances in mRNA
N. Engl. J. Med. 350, 2572–2581 (2004). 128. Boyle, D. L. et al. The JAK inhibitor tofacitinib expression profiles in the rheumatoid arthritis
107. Genovese, M. C. et al. Abatacept for rheumatoid suppresses synovial JAK1–STAT signalling in synovial membrane. Arthritis Res. Ther. 10, R98
arthritis refractory to tumor necrosis factor α rheumatoid arthritis. Ann. Rheum. Dis. 74, (2008).
inhibition. N. Engl. J. Med. 353, 1114–1123 1311–1316 (2015). 150. van der Pouw Kraan, T. C. et al. Responsiveness to
(2005). 129. Haringman, J. J., Kraan, M. C., Smeets, T. J., anti-tumour necrosis factor α therapy is related to pre-
108. Moreland, L. W. et al. Treatment of rheumatoid Zwinderman, K. H. & Tak, P. P. Chemokine blockade treatment tissue inflammation levels in rheumatoid
arthritis with a recombinant human tumor necrosis and chronic inflammatory disease: proof of concept in arthritis patients. Ann. Rheum. Dis. 67, 563–566
factor receptor (p75)-Fc fusion protein. N. Engl. patients with rheumatoid arthritis. Ann. Rheum. Dis. (2008).
J. Med. 337, 141–147 (1997). 62, 715–721 (2003). 151. Badot, V. et al. Gene expression profiling in the
109. Pitzalis, C. et al. Ectopic lymphoid-like structures in 130. Tak, P. P. et al. Chemokine receptor CCR1 antagonist synovium identifies a predictive signature of absence
infection, cancer and autoimmunity. Nat. Rev. CCX354‑C treatment for rheumatoid arthritis: of response to adalimumab therapy in rheumatoid
Immunol. 14, 447–462 (2014). CARAT‑2, a randomised, placebo controlled clinical arthritis. Arthritis Res. Ther. 11, R57 (2009).
110. Thurlings, R. M. et al. Synovial lymphoid neogenesis trial. Ann. Rheum. Dis. 72, 337–344 (2012). 152. Gutierrez-Roelens, I. et al. Rituximab treatment
does not define a specific clinical rheumatoid arthritis 131. Mullan, R. H. et al. Acute-phase serum amyloid A induces the expression of genes involved in healing
phenotype. Arthritis Rheum. 58, 1582–1589 stimulation of angiogenesis, leukocyte recruitment, processes in the rheumatoid arthritis synovium.
(2008). and matrix degradation in rheumatoid arthritis Arthritis Rheum. 63, 1246–1254 (2011).
111. Cantaert, T. et al. B lymphocyte autoimmunity in through an NF‑κB-dependent signal transduction 153. Colburn, W. A. Selecting and validating biologic
rheumatoid synovitis is independent of ectopic pathway. Arthritis Rheum. 54, 105–114 (2006). markers for drug development. J. Clin. Pharmacol.
lymphoid neogenesis. J. Immunol. 181, 785–794 132. Connolly, M. et al. Acute serum amyloid A is an 37, 355–362 (1997).
(2008). endogenous TLR2 ligand that mediates inflammatory 154. van de Sande, M. G. H. et al. Evaluating antirheumatic
112. Klaasen, R. et al. The relationship between synovial and angiogenic mechanisms. Ann. Rheum. Dis. 75, treatments using synovial biopsy: a recommendation
lymphocyte aggregates and the clinical response to 1392–1398 (2016). for standardisation to be used in clinical trials.
infliximab in rheumatoid arthritis: a prospective 133. Connolly, M., Veale, D. J. & Fearon, U. Acute serum Ann. Rheum. Dis. 70, 423–427 (2011).
study. Arthritis Rheum. 60, 3217–3224 (2009). amyloid A regulates cytoskeletal rearrangement, cell 155. Choi, I. Y., Gerlag, D. M., Holzinger, D., Roth, J. &
113. van de Sande, M. G. et al. Presence of lymphocyte matrix interactions and promotes cell migration in Tak, P. P. From synovial tissue to peripheral blood:
aggregates in the synovium of patients with early rheumatoid arthritis. Ann. Rheum. Dis. 70, 1296– myeloid related protein 8/14 is a sensitive biomarker
arthritis in relationship to diagnosis and outcome: is it 1303 (2011). for effective treatment in early drug development in
a constant feature over time? Ann. Rheum. Dis. 70, 134. Haringman, J. J., Ludikhuize, J. & Tak, P. P. patients with rheumatoid arthritis. PLoS ONE 9,
700–703 (2011). Chemokines in joint disease: the key to e106253 (2014).
114. Lindberg, J. et al. The gene expression profile in the inflammation? Ann. Rheum. Dis. 63, 1186–1194 156. Dennis, G. Jr et al. Synovial phenotypes in
synovium as a predictor of the clinical response to (2004). rheumatoid arthritis correlate with response to
infliximab treatment in rheumatoid arthritis. PLoS 135. Kraan, M. C. et al. The development of clinical signs biologic therapeutics. Arthritis Res. Ther. 16, R90
ONE 5, e11310 (2010). of rheumatoid synovial inflammation is associated (2014).
115. Dolhain, R. J. et al. Methotrexate reduces with increased synthesis of the chemokine CXCL8 157. Tan, P. K. et al. Evaluation of gene expression
inflammatory cell numbers, expression of monokines (interleukin‑8). Arthritis Res. 3, 65–71 (2001). measurements from commercial microarray
and of adhesion molecules in synovial tissue of 136. Kang, K. Y. et al. S100A8/A9 as a biomarker for platforms. Nucleic Acids Res. 31, 5676–5684
patients with rheumatoid arthritis. Rheumatology synovial inflammation and joint damage in patients. (2003).
(Oxford) 37, 502–508 (1998). Kor. J. Intern. Med. 29, 12–19 (2014). 158. Wang, Z., Gerstein, M. & Snyder, M. RNA-Seq: a
116. Walsh, C. A. E., Fearon, U., FitzGerald, O., Veale, D. J. 137. Wittkowski, H. et al. MRP8 and MRP14, phagocyte- revolutionary tool for transcriptomics. Nat. Rev. Genet.
& Bresnihan, B. Decreased CD20 expression in specific danger signals, are sensitive biomarkers of 10, 57–63 (2009).
rheumatoid arthritis synovium following 8 weeks of disease activity in cryopyrin-associated periodic 159. Gao, W. et al. Notch signalling pathways mediate
rituximab therapy. Clin. Exp. Rheumatol. 26, 656 syndromes. Ann. Rheum. Dis. 70, 2075–2081 synovial angiogenesis in response to vascular
(2008). (2011). endothelial growth factor and angiopoietin 2.
117. Vos, K. et al. Early effects of rituximab on the synovial 138. Meijer, B., Gearry, R. B. & Day, A. S. The role of Ann. Rheum. Dis. 72, 1080–1088 (2013).
cell infiltrate in patients with rheumatoid arthritis. S100A12 as a systemic marker of inflammation. Int. 160. Ebhardt, H. A. et al. Applications of targeted
Arthritis Rheum. 56, 772–778 (2007). J. Inflam 2012, 907078 (2012). proteomics in systems biology and translational
118. Bresnihan, B. et al. Synovial macrophages as a 139. Liao, H. et al. Use of mass spectrometry to identify medicine. Proteomics 15, 3193–3208 (2015).
biomarker of response to therapeutic intervention in protein biomarkers of disease severity in the synovial 161. Smith, S. L., Plant, D., Eyre, S. & Barton, A. The
rheumatoid arthritis: standardization and consistency fluid and serum of patients with rheumatoid arthritis. potential use of expression profiling: implications for
across centers. J. Rheumatol. 36, 1800–1802 Arthritis Rheum. 50, 3792–3803 (2004). predicting treatment response in rheumatoid
(2009). 140. Green, M. J. et al. Serum MMP‑3 and MMP‑1 and arthritis. Ann. Rheum. Dis. 72, 1118–1124 (2013).
119. Kavanaugh, A. et al. Assessment of rituximab’s progression of joint damage in early rheumatoid 162. Häupl, T., Stuhlmüller, B., Grützkau, A., Radbruch, A.
immunomodulatory synovial effects (ARISE trial). 1: arthritis. Rheumatology (Oxford) 42, 83–88 & Burmester, G. R. Does gene expression analysis
clinical and synovial biomarker results. Ann. Rheum. (2003). inform us in rheumatoid arthritis? Ann. Rheum. Dis.
Dis. 67, 402–408 (2008). 141. Ishiguro, N. et al. Relationships of matrix 69, i37–i42 (2010).
120. Yanni, G., Nabil, M., Farahat, M. R., Poston, R. N. & metalloproteinases and their inhibitors to cartilage 163. van Baarsen, L. G. M. et al. Synovial tissue
Panayi, G. S. Intramuscular gold decreases cytokine proteoglycan and collagen turnover and inflammation heterogeneity in rheumatoid arthritis in relation to
expression and macrophage numbers in the as revealed by analyses of synovial fluids from patients disease activity and biomarkers in peripheral blood.
rheumatoid synovial membrane. Ann. Rheum. Dis. 53, with rheumatoid arthritis. Arthritis Rheum. 44, Arthritis Rheum. 62, 1602–1607 (2010).
315–322 (1994). 2503–2511 (2001).
121. Smith, M. D. et al. Treatment-induced remission in 142. Chandran, V. Soluble biomarkers may differentiate Acknowledgements
rheumatoid arthritis patients is characterized by a psoriasis from psoriatic arthritis. J. Rheumatol. 89, We wish to thank all our colleagues in the European Synovitis
reduction in macrophage content of synovial biopsies. 65–66 (2012). Study Group and in the OMERACT group who have sup-
Rheumatology (Oxford) 40, 367–374 (2001). 143. Boumans, M. J. et al. Rituximab abrogates joint ported the development of synovial tissue research.
122. Wijbrandts, C. A. et al. The clinical response to destruction in rheumatoid arthritis by inhibiting
infliximab in rheumatoid arthritis is in part dependent osteoclastogenesis. Ann. Rheum. Dis. 71, 108–113 Author contributions
on pretreatment tumour necrosis factor α expression (2012). D.J.V., C.O., U.F., A.N., A.P. and J.E.F. researched data for the
in the synovium. Ann. Rheum. Dis. 67, 1139–1144 144. Masson-Bessiere, C. et al. The major synovial targets article, made a substantial contribution to the discussion of
(2008). of the rheumatoid arthritis-specific antifilaggrin article content, wrote the manuscript, and reviewed and
123. Haringman, J. J. et al. Synovial tissue macrophages: autoantibodies are deiminated forms of the α- and edited the manuscript before submission. E.S., F.H., S.A.J., T.
a sensitive biomarker for response to treatment in β-chains of fibrin. J. Immunol. 166, 4177–4184 McG. and R.T. researched data for the article, wrote the man-
patients with rheumatoid arthritis. Ann. Rheum. Dis. (2001). uscript, and reviewed and edited the manuscript before sub-
64, 834–838 (2005). 145. Després, N., Boire, G., Lopez-Longo, F. J. & mission. A.F. researched data for the article, and reviewed and
124. Boumans, M. J. et al. Response to rituximab in Ménard, H. A. The Sa system: a novel antigen- edited the manuscript before submission. B.R.L. wrote the
patients with rheumatoid arthritis in different antibody system specific for rheumatoid arthritis. manuscript, and reviewed and edited the manuscript before
compartments of the immune system. Arthritis J. Rheumatol. 21, 1027–1033 (1994). submission. D.L.B., M.H.B., C.D.B., J.D.C., A.I.C., E.H.C., P.E.,
Rheum. 63, 3187–3194 (2011). 146. Baeten, D. et al. Specific presence of intracellular D.G., J.D.I., B.L., A.M., I.B.M., C.P., M.S. and P.P.T. reviewed
125. Wijbrandts, C. A. et al. Absence of changes in the citrullinated proteins in rheumatoid arthritis and edited the manuscript before submission.
number of synovial sublining macrophages after synovium: relevance to antifilaggrin autoantibodies.
ineffective treatment for rheumatoid arthritis: Arthritis Rheum. 44, 2255–2262 (2001). Competing interests statement
implications for use of synovial sublining macrophages 147. Masson-Bessiere, C. et al. In the rheumatoid pannus, The authors declare no competing interests.
as a biomarker. Arthritis Rheum. 56, 3869–3871 anti-filaggrin autoantibodies are produced by local
(2007). plasma cells and constitute a higher proportion of IgG Publisher’s note
126. Bresnihan, B. et al. Synovial tissue analysis in clinical than in synovial fluid and serum. Clin. Exp. Immunol. Springer Nature remains neutral with regard to jurisdictional
trials. J. Rheumatol. 32, 2481–2484 (2005). 119, 544–552 (2000). claims in published maps and institutional affiliations.
NATURE REVIEWS | RHEUMATOLOGY ADVANCE ONLINE PUBLICATION | 13
©
2
0
1
7
M
a
c
m
i
l
l
a
n
P
u
b
l
i
s
h
e
r
s
L
i
m
i
t
e
d
,
p
a
r
t
o
f
S
p
r
i
n
g
e
r
N
a
t
u
r
e
.
A
l
l
r
i
g
h
t
s
r
e
s
e
r
v
e
d
.
You might also like
- Redefining Lupus Nephritis, Clinical Implications of Pathophysiologic Subtypes PDFDocument14 pagesRedefining Lupus Nephritis, Clinical Implications of Pathophysiologic Subtypes PDFaneliatiarasuciNo ratings yet
- 10 1038@nrneph 2017 85 PDFDocument13 pages10 1038@nrneph 2017 85 PDFSirGonzNo ratings yet
- Smolen2018 PDFDocument23 pagesSmolen2018 PDFJose Correa100% (1)
- Tsokos 2016Document15 pagesTsokos 2016karen rinconNo ratings yet
- Nrgastro 2017 1Document12 pagesNrgastro 2017 1Golam ZakariaNo ratings yet
- Neutrophil Migration Nature RevImmunol 2016Document14 pagesNeutrophil Migration Nature RevImmunol 2016stefanie.sousaNo ratings yet
- Engineering and Physical Sciences in Oncology - Challenges and OpportunitiesDocument17 pagesEngineering and Physical Sciences in Oncology - Challenges and OpportunitiesAlessandroNo ratings yet
- Cryptococcal MeningitisDocument12 pagesCryptococcal MeningitisIan SaundersNo ratings yet
- Barturen 2018Document20 pagesBarturen 2018jezy2014No ratings yet
- Orofacial Manifestations of Systemic SclerosisDocument6 pagesOrofacial Manifestations of Systemic SclerosisIt's MeNo ratings yet
- Loeser PDFDocument9 pagesLoeser PDFGaudeamus IgiturNo ratings yet
- Estefania Gallego PonenciaDocument16 pagesEstefania Gallego PonenciaJilberth Hermann CandeloNo ratings yet
- ES GastrointestinalDocument12 pagesES GastrointestinalMateus ValenteNo ratings yet
- Oesophageal Cancer-1Document1 pageOesophageal Cancer-1BRENDANo ratings yet
- Modelling Diabetic Nephropathy in MiceDocument9 pagesModelling Diabetic Nephropathy in MiceKarina ThiemeNo ratings yet
- NRDP 20174Document17 pagesNRDP 20174EccoNo ratings yet
- Lectura Seminario 3 - NF1Document17 pagesLectura Seminario 3 - NF1Diego SoteloNo ratings yet
- Tuberculous MeningitisDocument18 pagesTuberculous Meningitistjdvv8cbfrNo ratings yet
- Manifestaciones Neurologicas VIH NatureDocument13 pagesManifestaciones Neurologicas VIH NatureGeral D. VelascoNo ratings yet
- Panes Rimola 2017Document13 pagesPanes Rimola 2017Natasya DarrelNo ratings yet
- Potential New Therapy For OphthalmopathyDocument1 pagePotential New Therapy For OphthalmopathyEsteban Martin Chiotti KaneshimaNo ratings yet
- Oligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Document11 pagesOligometastatic Prostate Cancer. Definitions, Clinical Outcomes, and Treatment Considerations (2017) .Orlando SotoNo ratings yet
- Kellum 2018Document14 pagesKellum 2018hemer hadyn calderon alvitesNo ratings yet
- Targeting Neoantigens To Augment Antitumour ImmunityDocument14 pagesTargeting Neoantigens To Augment Antitumour Immunitylaura isabellaNo ratings yet
- Primer. Vejiga. 2017Document19 pagesPrimer. Vejiga. 2017Isabel Gago CastilloNo ratings yet
- Living KidneyDocument9 pagesLiving KidneyEss liNo ratings yet
- Reviews: Hirschsprung Disease - Integrating Basic Science and Clinical Medicine To Improve OutcomesDocument16 pagesReviews: Hirschsprung Disease - Integrating Basic Science and Clinical Medicine To Improve OutcomesThanh Thảo PhanNo ratings yet
- Reviews: Computational Genomics Tools For Dissecting Tumour-Immune Cell InteractionsDocument18 pagesReviews: Computational Genomics Tools For Dissecting Tumour-Immune Cell Interactionsdata lmleNo ratings yet
- Consensus: StatementDocument10 pagesConsensus: StatementAdrilupiss ArroyoNo ratings yet
- Update On Outcome Assessment in MyositisDocument16 pagesUpdate On Outcome Assessment in MyositisKevin Christofer NavejasNo ratings yet
- Kahrilas 2017Document12 pagesKahrilas 2017Josseph EscobarNo ratings yet
- Hepatocarcinoma 2Document23 pagesHepatocarcinoma 2NaraMayhumiDeBelenMerinoOrtizNo ratings yet
- Beyond Binding Antibody - Lu Et Al. NatureDocument17 pagesBeyond Binding Antibody - Lu Et Al. NatureSamia NouhNo ratings yet
- Membranosa 2Document17 pagesMembranosa 2Carolina CastroNo ratings yet
- Art RitisDocument15 pagesArt RitisHarwin JHoel Salazar UrbanoNo ratings yet
- 16 Bioresponsive MaterialsDocument17 pages16 Bioresponsive MaterialsAlex. SonicaNo ratings yet
- Alhmeimer 23445Document15 pagesAlhmeimer 23445safia osmanNo ratings yet
- ANTYPHOSPHODocument20 pagesANTYPHOSPHOLuis David Beltran OntiverosNo ratings yet
- Scleroderma Renal Crisis and Renal Involvement in Systemic SclerosisDocument14 pagesScleroderma Renal Crisis and Renal Involvement in Systemic Sclerosiszlaticab4246No ratings yet
- Abdollahi-Roodsaz2016 Artigo3Document10 pagesAbdollahi-Roodsaz2016 Artigo3JamilaNo ratings yet
- Nrgastro 2017 38Document15 pagesNrgastro 2017 38Fasya DaffaNo ratings yet
- Development and Regulation of Single - and Multi-Species Candida Albicans BiofilmsDocument13 pagesDevelopment and Regulation of Single - and Multi-Species Candida Albicans BiofilmsCatalina AguayoNo ratings yet
- Yazici Et Al - 2018 - Behçet SyndromeDocument13 pagesYazici Et Al - 2018 - Behçet SyndromeantonioivNo ratings yet
- Multiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Document14 pagesMultiple Sclerosis Neurogenic Bladder 10.1038@nrurol.2016.53Putri Rizky AmaliaNo ratings yet
- Kuner 2016Document11 pagesKuner 2016Guilherme MonteiroNo ratings yet
- Reviews: Autism Genetics: Opportunities and Challenges For Clinical TranslationDocument15 pagesReviews: Autism Genetics: Opportunities and Challenges For Clinical TranslationAlexandra DragomirNo ratings yet
- Reviews: A Clinicopathological Approach To The Diagnosis of DementiaDocument16 pagesReviews: A Clinicopathological Approach To The Diagnosis of DementiaLeonardo Barrera ArizaNo ratings yet
- 1 ISAPP Consensus Statement PREBIOTICS 2017Document12 pages1 ISAPP Consensus Statement PREBIOTICS 2017KatherineNo ratings yet
- Dyslipidaemia in Nephrotic Syndrome: Mechanisms and TreatmentDocument14 pagesDyslipidaemia in Nephrotic Syndrome: Mechanisms and TreatmentEss liNo ratings yet
- CiliopatiasDocument15 pagesCiliopatiasdhernandez35No ratings yet
- Primer: Antiphospholipid SyndromeDocument19 pagesPrimer: Antiphospholipid SyndromenowimsunheeNo ratings yet
- Escobar Mor Real e 2018Document15 pagesEscobar Mor Real e 2018HIDAYATUL RAHMINo ratings yet
- Nrneurol 2018 30 PDFDocument16 pagesNrneurol 2018 30 PDFFathan MustafidNo ratings yet
- 10 1038@nrurol 2018 1Document15 pages10 1038@nrurol 2018 1cristianNo ratings yet
- Wing Ho Man (2017) Microbiota of The Respiratory Tract, Gatekeeper To Respiratory HealthDocument12 pagesWing Ho Man (2017) Microbiota of The Respiratory Tract, Gatekeeper To Respiratory HealthLuan DiasNo ratings yet
- A Systemic View of Alzheimer Disease 2017Document12 pagesA Systemic View of Alzheimer Disease 2017Jaime Arevalo PanduroNo ratings yet
- Complex Regional Pain Syndrome - Diagnosis, Treatment and Future PerspectivesDocument14 pagesComplex Regional Pain Syndrome - Diagnosis, Treatment and Future Perspectivesyulita kesumaNo ratings yet
- Reviews: Inflammation in Gout: Mechanisms and Therapeutic TargetsDocument9 pagesReviews: Inflammation in Gout: Mechanisms and Therapeutic TargetsBless MineNo ratings yet
- Nrneph 2017 148Document19 pagesNrneph 2017 148Gabriela CarolinaNo ratings yet
- Raynaud’s Phenomenon: A Guide to Pathogenesis and TreatmentFrom EverandRaynaud’s Phenomenon: A Guide to Pathogenesis and TreatmentFredrick M. WigleyNo ratings yet
- Case Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Document18 pagesCase Presentation Peptic Ulcer: Ma. Christina T. Alvarez Wup - Bs Nursing Iii-2Shane Aileen AngelesNo ratings yet
- DrugmedsDocument52 pagesDrugmedsshirleyNo ratings yet
- Hiv/Aids: Elsebey NotesDocument22 pagesHiv/Aids: Elsebey NotesrsimranjitNo ratings yet
- Gross Anatomy of The Digestive System Lecture Notes Lecture 2Document5 pagesGross Anatomy of The Digestive System Lecture Notes Lecture 2Lorelie AsisNo ratings yet
- Multiple Sclerosis Lancet 2018Document15 pagesMultiple Sclerosis Lancet 2018Sarah Miryam CoffanoNo ratings yet
- Ebook Psychology Psyc2020 Psyc2021 Custom Edition by Schutte E Ed Et A PDF Full Chapter PDFDocument67 pagesEbook Psychology Psyc2020 Psyc2021 Custom Edition by Schutte E Ed Et A PDF Full Chapter PDFedward.bittner820100% (35)
- Week 6 PCP Workbook QsDocument6 pagesWeek 6 PCP Workbook Qsapi-479849199No ratings yet
- Module Pharma 1Document21 pagesModule Pharma 1Donya GholamiNo ratings yet
- NEET PG Syllabus 2024 - Detailed Subject-Wise TopicsDocument70 pagesNEET PG Syllabus 2024 - Detailed Subject-Wise Topicsmayur TNo ratings yet
- Aubf Lab Microscopic Examination Part 1Document2 pagesAubf Lab Microscopic Examination Part 1Hannah KateNo ratings yet
- Furosemide Summary Report Committee Veterinary Medicinal Products enDocument9 pagesFurosemide Summary Report Committee Veterinary Medicinal Products enLucijaRomićNo ratings yet
- OSCE Book 2010-1 PDFDocument256 pagesOSCE Book 2010-1 PDFSyeda Eshaal Javaid100% (1)
- Case Study Fracture 2 (Drug Study and NCP)Document8 pagesCase Study Fracture 2 (Drug Study and NCP)chrom17No ratings yet
- Trigger Topics For FMG Exams by MistDocument3 pagesTrigger Topics For FMG Exams by Mistvijay resuNo ratings yet
- Cardio Exercise Testing in Children and AdolecentsDocument288 pagesCardio Exercise Testing in Children and AdolecentsTeoNo ratings yet
- Escleritis EpiescleritisDocument16 pagesEscleritis EpiescleritisAngeloCarpioNo ratings yet
- 2 OS To PrintDocument12 pages2 OS To PrintDENTAL REVIEWER ONLY0% (1)
- Sessile Serrated Adenoma - Libre PathologyDocument5 pagesSessile Serrated Adenoma - Libre PathologyfadoNo ratings yet
- Thyroid Disorders Part I Hyperthyroidism Little 2006Document9 pagesThyroid Disorders Part I Hyperthyroidism Little 2006Jing XueNo ratings yet
- Amiodarone Infusion GuidelineDocument3 pagesAmiodarone Infusion GuidelineNur SusiawantyNo ratings yet
- Idiopathic Talipes Equinovarus Congenital ClubfootDocument15 pagesIdiopathic Talipes Equinovarus Congenital ClubfootNindy PutriNo ratings yet
- Barium Enema and Biliary System1Document18 pagesBarium Enema and Biliary System1sheenamarielaruyaNo ratings yet
- Ketorolac Tromethamine Injection Usp: Product MonographDocument41 pagesKetorolac Tromethamine Injection Usp: Product MonographWahyu AriawanNo ratings yet
- Bifascicular Block Revealing Steinerts Myotonic DystrophyDocument8 pagesBifascicular Block Revealing Steinerts Myotonic DystrophyIJAR JOURNALNo ratings yet
- K - 7 Supraventrikular Takikardia (IKA)Document12 pagesK - 7 Supraventrikular Takikardia (IKA)thomasfelixNo ratings yet
- AMPXICILLINDocument3 pagesAMPXICILLINPark JeongyeonNo ratings yet
- Tinea Versicolor (Pityriasis Versicolor) - UpToDateDocument47 pagesTinea Versicolor (Pityriasis Versicolor) - UpToDatejotaere RobNo ratings yet
- Facial InjuryDocument40 pagesFacial Injuryahmad iffa maududyNo ratings yet
- Curiculum VitaeDocument5 pagesCuriculum VitaeZEINABAHMEDNo ratings yet
- " Drop Foot": Arranged By: Nabiilah Aznesia NPM 71170891191Document12 pages" Drop Foot": Arranged By: Nabiilah Aznesia NPM 71170891191NaomiRimaClaudyaNo ratings yet