
Whitereyes - Ocular/Medical/General Information: Glasses History
Whitereyes - Ocular/Medical/General Information: Glasses History
You might also like
- Test Bank For Wongs Essentials of Pediatric Nursing 11th Edition Marilyn J Hockenberry Cheryl C Rodgers David WilsonDocument7 pagesTest Bank For Wongs Essentials of Pediatric Nursing 11th Edition Marilyn J Hockenberry Cheryl C Rodgers David Wilsondennisgallegosmkrgyabsod100% (19)
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- CRM New ScriptDocument13 pagesCRM New ScriptCleriss98No ratings yet
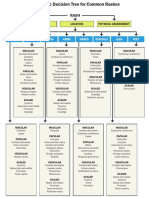
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
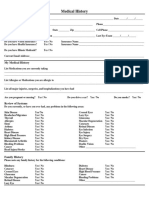
- New Patient Medical History Form 2023 03 29Document2 pagesNew Patient Medical History Form 2023 03 29Trouvaille medicoNo ratings yet
- Medical Examination Form 2022-2023Document5 pagesMedical Examination Form 2022-2023Linh ĐặngNo ratings yet
- 35137-iUBT296 Client Consultation Form v1Document7 pages35137-iUBT296 Client Consultation Form v1RamzzzNo ratings yet
- New Patient Registration FormDocument4 pagesNew Patient Registration Formapi-358908929No ratings yet
- Annex V Annual Medical Examination AME FormDocument5 pagesAnnex V Annual Medical Examination AME FormRohini RoopnarineNo ratings yet
- Questionaire - Reasearch Group-2Document4 pagesQuestionaire - Reasearch Group-2Salah Ud DinNo ratings yet
- Identifying Information and Healthcare Provider (For Child Patient)Document9 pagesIdentifying Information and Healthcare Provider (For Child Patient)Prabha GuptaNo ratings yet
- Registration FormDocument3 pagesRegistration Formbwalsh82No ratings yet
- Healthhistoryform 2018Document2 pagesHealthhistoryform 2018iwasan991No ratings yet
- Health Declaration Form: Your Offspring, Sibling(s)Document4 pagesHealth Declaration Form: Your Offspring, Sibling(s)Peter Angelo GeleraNo ratings yet
- Patient'S ProfileDocument17 pagesPatient'S ProfileLucas JelmarNo ratings yet
- 37821-iUCT32 Consultation Form v2Document11 pages37821-iUCT32 Consultation Form v2taraturgooseNo ratings yet
- 36316-IUCT22 Client Consultation Form v1Document7 pages36316-IUCT22 Client Consultation Form v1michellepayne1806No ratings yet
- Case Study Male MSW 1Document27 pagesCase Study Male MSW 1JONAMAY RAMIREZNo ratings yet
- Baseline Occupational Medical Evaluation Proposed Reporting Revised FormatDocument3 pagesBaseline Occupational Medical Evaluation Proposed Reporting Revised FormatAhmed OsmanNo ratings yet
- Uw Autism Center Intake Packet: What Are Your Primary Patient Concerns? Please Be SpecificDocument10 pagesUw Autism Center Intake Packet: What Are Your Primary Patient Concerns? Please Be SpecificPrabha GuptaNo ratings yet
- Medical History 2020Document1 pageMedical History 2020api-515540617No ratings yet
- MedicineDocument282 pagesMedicineGgah VgggagagsgNo ratings yet
- 17-18 Medical FormDocument2 pages17-18 Medical FormVinOu TeChNo ratings yet
- Treatment Evidence Form: iUBT431 - Facial Electrical TreatmentsDocument5 pagesTreatment Evidence Form: iUBT431 - Facial Electrical TreatmentsVivi AnaNo ratings yet
- Medical HistoryDocument2 pagesMedical HistoryMiguel San JuanNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AClick TechnologyNo ratings yet
- טפסים לביטוח רפואיDocument3 pagesטפסים לביטוח רפואיmaricelangob3No ratings yet
- Medicalhistoryformpg 1Document2 pagesMedicalhistoryformpg 1reynanfrancebernabeNo ratings yet
- Medical Examination Report (Aidil Fit)Document2 pagesMedical Examination Report (Aidil Fit)Husni WahyudiNo ratings yet
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Evaluation of Patients With PolyuriaDocument25 pagesEvaluation of Patients With Polyurianaura ghinaNo ratings yet
- Norway Down SynrdomeDocument56 pagesNorway Down SynrdomeAjay RoopeshNo ratings yet
- DSMES Assessment Template (Chart 7)Document4 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Facial Client Intake Form: by Signing This Form, The Client Agrees To The FollowingDocument1 pageFacial Client Intake Form: by Signing This Form, The Client Agrees To The Followingarasan2297No ratings yet
- Patient InformationDocument2 pagesPatient Informationsteve6621No ratings yet
- Medical Declaration 2022 2023Document1 pageMedical Declaration 2022 2023M. YoussefNo ratings yet
- SurveyhypertensionDocument3 pagesSurveyhypertensionNiran ThapaNo ratings yet
- Dermato History FormDocument1 pageDermato History Formlaila.forestaNo ratings yet
- PANAMADocument3 pagesPANAMA7vs8ndtrrcNo ratings yet
- Jaundice Symptoms in Adults - Google SearchDocument1 pageJaundice Symptoms in Adults - Google Searchs8903082No ratings yet
- Hospital Claim - Template24 - Page4Document1 pageHospital Claim - Template24 - Page4chamuditha dilshanNo ratings yet
- Patient Medical History (Eng)Document2 pagesPatient Medical History (Eng)desaisaravNo ratings yet
- Form 19Document1 pageForm 19Nurul Huda KhanNo ratings yet
- Abdominal Lab MaterialsDocument11 pagesAbdominal Lab MaterialsPunnam Anurag ReddyNo ratings yet
- Medical Screening Questionnaire: Before You BeginDocument6 pagesMedical Screening Questionnaire: Before You Begins9sxxtjmqjNo ratings yet
- Daniel Cameron Asscoiates New Patient FormsDocument25 pagesDaniel Cameron Asscoiates New Patient Formsjudymw2000No ratings yet
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- DSMES Assessment Template (Chart 7)Document5 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Assessment FormDocument8 pagesAssessment FormbonnieyfNo ratings yet
- Health Declaration For Care 4 U Policy / Medical InsuranceDocument2 pagesHealth Declaration For Care 4 U Policy / Medical InsuranceMarco AglibotNo ratings yet
- Questionnaire On Awareness of Diabetes Mellitus Dr. Kanak ChoudhuryDocument3 pagesQuestionnaire On Awareness of Diabetes Mellitus Dr. Kanak ChoudhuryBichayan Debbarma100% (1)
- SDO TARLAC PROVINCE Health Screening and AssessmentDocument2 pagesSDO TARLAC PROVINCE Health Screening and AssessmentKrishna Mae GarciaNo ratings yet
- New Patient/Consultation Form: AllergiesDocument2 pagesNew Patient/Consultation Form: AllergiesAlexander Flores SaraviaNo ratings yet
- New Patient Health History Form: (Please Explain Below)Document2 pagesNew Patient Health History Form: (Please Explain Below)KevinNo ratings yet
- 37981-iUBT311 Treatment Evidence Form v2Document5 pages37981-iUBT311 Treatment Evidence Form v2Aline Brito Ferreira de CastroNo ratings yet
- Legal History and PEDocument1 pageLegal History and PELoreto District Hospital LDHNo ratings yet
- Panama Form F-103 Recording Medical Examinations of Seafarers v. 04Document8 pagesPanama Form F-103 Recording Medical Examinations of Seafarers v. 04Preeti HandaNo ratings yet
- Medical History FormDocument4 pagesMedical History FormevalinadrNo ratings yet
- DIABETES in ELDERLY by Supriyanto KartodarsonoDocument23 pagesDIABETES in ELDERLY by Supriyanto Kartodarsonobryan ruditaNo ratings yet
- Diabetic Retinopathy: From Diagnosis to TreatmentFrom EverandDiabetic Retinopathy: From Diagnosis to TreatmentRating: 3 out of 5 stars3/5 (3)
- Scleroderma Diet: A Beginner's 3-Step Quick Start Guide on Managing Scleroderma Through Diet, With Sample Curated RecipesFrom EverandScleroderma Diet: A Beginner's 3-Step Quick Start Guide on Managing Scleroderma Through Diet, With Sample Curated RecipesNo ratings yet
- GTDocument122 pagesGTAnand Patel100% (1)
- Paramagnetic Oxygen Analyzer PDFDocument5 pagesParamagnetic Oxygen Analyzer PDFAnand PatelNo ratings yet
- Curriculum Vitae: 1.0 Resume Submitted ForDocument3 pagesCurriculum Vitae: 1.0 Resume Submitted ForAnand PatelNo ratings yet
- CV Format Sample - ZADCODocument4 pagesCV Format Sample - ZADCOAnand PatelNo ratings yet
- CV FormatDocument2 pagesCV FormatAnand PatelNo ratings yet
- SafariViewService - Jul 9, 2019 at 09:23Document1 pageSafariViewService - Jul 9, 2019 at 09:23Anand Patel100% (1)
- Checklist For Mechanical CompletionDocument8 pagesChecklist For Mechanical CompletionAnand PatelNo ratings yet
- ID For ABIM - Parham 2014Document140 pagesID For ABIM - Parham 2014Jeronim H'gharNo ratings yet
- Summary of Infectious DiseasesDocument415 pagesSummary of Infectious DiseasesAlston Foods BVNo ratings yet
- (Soal Materi) Summarizing Passage Paket 2Document4 pages(Soal Materi) Summarizing Passage Paket 2aswinmt12No ratings yet
- Chickenpox & ChlamydialDocument5 pagesChickenpox & ChlamydialEliezah RodriguezNo ratings yet
- CSIR Unit 4 - Full NotesDocument80 pagesCSIR Unit 4 - Full NotesSubhrajyoti BanerjeeNo ratings yet
- Herppvc PDFDocument6 pagesHerppvc PDFDr.Chetana INo ratings yet
- Common Communicable DiseasesDocument86 pagesCommon Communicable DiseasesBenj VillanuevaNo ratings yet
- Essential Drugs 2013Document378 pagesEssential Drugs 2013Chedeng KumaNo ratings yet
- June 6, 2013 Mount Ayr Record-NewsDocument14 pagesJune 6, 2013 Mount Ayr Record-NewsMountAyrRecordNewsNo ratings yet
- Virology ModuleDocument165 pagesVirology ModuleAhmed KerAtyNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Vaccinations: Slam Shraf AhmyDocument11 pagesVaccinations: Slam Shraf AhmyFahad Alkenani100% (1)
- Nclex Random Fact To StudyDocument431 pagesNclex Random Fact To StudyNeko Neko100% (1)
- BDJ Orofacial PainDocument10 pagesBDJ Orofacial PainjayashreeNo ratings yet
- Z - The Clark Zapper Blog & Rife Digital MachinesDocument1 pageZ - The Clark Zapper Blog & Rife Digital MachinescesargnomoNo ratings yet
- Treatment Chronic PainDocument18 pagesTreatment Chronic PainSukedanaNo ratings yet
- Tarlac State University Graduate StudiesDocument4 pagesTarlac State University Graduate StudiesL.J. SantosNo ratings yet
- Comparison of Rubric in KENT, BTPB and BBCRDocument23 pagesComparison of Rubric in KENT, BTPB and BBCRaswathymohan1024No ratings yet
- Varicella & Herpes ZosterDocument33 pagesVaricella & Herpes ZosterRMRNo ratings yet
- Teaching Regarding Measures To Improve Sleep?Document37 pagesTeaching Regarding Measures To Improve Sleep?Martin HusseinNo ratings yet
- Jomo Kenyatta University OF Agriculture & Technology: P.O. Box 62000, 00200 Nairobi, Kenya E-Mail: Elearning@jkuat - Ac.keDocument32 pagesJomo Kenyatta University OF Agriculture & Technology: P.O. Box 62000, 00200 Nairobi, Kenya E-Mail: Elearning@jkuat - Ac.keKeddie OneJhereNo ratings yet
- John Murtaghs General Practice Companion Handbook 7Th Edition John Murtagh Full Chapter PDF ScribdDocument67 pagesJohn Murtaghs General Practice Companion Handbook 7Th Edition John Murtagh Full Chapter PDF Scribdderrick.ayala232100% (7)
- Transfer Factor-Myths and FactsDocument10 pagesTransfer Factor-Myths and FactsIris BetancourtNo ratings yet
- Little Red Riding Hood: A Dermatologic JourneyDocument27 pagesLittle Red Riding Hood: A Dermatologic JourneyjthsNo ratings yet
- Rife RatesDocument17 pagesRife Rateszonetrek100% (1)
- Oral Pathology ModuleDocument31 pagesOral Pathology ModuleDenee Vem MatorresNo ratings yet
- Chickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella ZosterDocument12 pagesChickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella Zostersubbu2raj3372100% (2)
- Essential DrugsDocument358 pagesEssential Drugsshahera rosdiNo ratings yet






























































































Download as pdf or txt
You might also like
- Test Bank For Wongs Essentials of Pediatric Nursing 11th Edition Marilyn J Hockenberry Cheryl C Rodgers David WilsonDocument7 pagesTest Bank For Wongs Essentials of Pediatric Nursing 11th Edition Marilyn J Hockenberry Cheryl C Rodgers David Wilsondennisgallegosmkrgyabsod100% (19)
- MLC Medical FormDocument5 pagesMLC Medical FormSoekhaidir SuripnoNo ratings yet
- CRM New ScriptDocument13 pagesCRM New ScriptCleriss98No ratings yet
- WK 5 Rash Decision TreeDocument1 pageWK 5 Rash Decision TreeBetsy Brown ByersmithNo ratings yet
- New Patient Medical History Form 2023 03 29Document2 pagesNew Patient Medical History Form 2023 03 29Trouvaille medicoNo ratings yet
- Medical Examination Form 2022-2023Document5 pagesMedical Examination Form 2022-2023Linh ĐặngNo ratings yet
- 35137-iUBT296 Client Consultation Form v1Document7 pages35137-iUBT296 Client Consultation Form v1RamzzzNo ratings yet
- New Patient Registration FormDocument4 pagesNew Patient Registration Formapi-358908929No ratings yet
- Annex V Annual Medical Examination AME FormDocument5 pagesAnnex V Annual Medical Examination AME FormRohini RoopnarineNo ratings yet
- Questionaire - Reasearch Group-2Document4 pagesQuestionaire - Reasearch Group-2Salah Ud DinNo ratings yet
- Identifying Information and Healthcare Provider (For Child Patient)Document9 pagesIdentifying Information and Healthcare Provider (For Child Patient)Prabha GuptaNo ratings yet
- Registration FormDocument3 pagesRegistration Formbwalsh82No ratings yet
- Healthhistoryform 2018Document2 pagesHealthhistoryform 2018iwasan991No ratings yet
- Health Declaration Form: Your Offspring, Sibling(s)Document4 pagesHealth Declaration Form: Your Offspring, Sibling(s)Peter Angelo GeleraNo ratings yet
- Patient'S ProfileDocument17 pagesPatient'S ProfileLucas JelmarNo ratings yet
- 37821-iUCT32 Consultation Form v2Document11 pages37821-iUCT32 Consultation Form v2taraturgooseNo ratings yet
- 36316-IUCT22 Client Consultation Form v1Document7 pages36316-IUCT22 Client Consultation Form v1michellepayne1806No ratings yet
- Case Study Male MSW 1Document27 pagesCase Study Male MSW 1JONAMAY RAMIREZNo ratings yet
- Baseline Occupational Medical Evaluation Proposed Reporting Revised FormatDocument3 pagesBaseline Occupational Medical Evaluation Proposed Reporting Revised FormatAhmed OsmanNo ratings yet
- Uw Autism Center Intake Packet: What Are Your Primary Patient Concerns? Please Be SpecificDocument10 pagesUw Autism Center Intake Packet: What Are Your Primary Patient Concerns? Please Be SpecificPrabha GuptaNo ratings yet
- Medical History 2020Document1 pageMedical History 2020api-515540617No ratings yet
- MedicineDocument282 pagesMedicineGgah VgggagagsgNo ratings yet
- 17-18 Medical FormDocument2 pages17-18 Medical FormVinOu TeChNo ratings yet
- Treatment Evidence Form: iUBT431 - Facial Electrical TreatmentsDocument5 pagesTreatment Evidence Form: iUBT431 - Facial Electrical TreatmentsVivi AnaNo ratings yet
- Medical HistoryDocument2 pagesMedical HistoryMiguel San JuanNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AHector ValleNo ratings yet
- Peme Reme Form ADocument1 pagePeme Reme Form AClick TechnologyNo ratings yet
- טפסים לביטוח רפואיDocument3 pagesטפסים לביטוח רפואיmaricelangob3No ratings yet
- Medicalhistoryformpg 1Document2 pagesMedicalhistoryformpg 1reynanfrancebernabeNo ratings yet
- Medical Examination Report (Aidil Fit)Document2 pagesMedical Examination Report (Aidil Fit)Husni WahyudiNo ratings yet
- Biennial National Medical ReportDocument5 pagesBiennial National Medical ReportXimena FariasNo ratings yet
- Evaluation of Patients With PolyuriaDocument25 pagesEvaluation of Patients With Polyurianaura ghinaNo ratings yet
- Norway Down SynrdomeDocument56 pagesNorway Down SynrdomeAjay RoopeshNo ratings yet
- DSMES Assessment Template (Chart 7)Document4 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Facial Client Intake Form: by Signing This Form, The Client Agrees To The FollowingDocument1 pageFacial Client Intake Form: by Signing This Form, The Client Agrees To The Followingarasan2297No ratings yet
- Patient InformationDocument2 pagesPatient Informationsteve6621No ratings yet
- Medical Declaration 2022 2023Document1 pageMedical Declaration 2022 2023M. YoussefNo ratings yet
- SurveyhypertensionDocument3 pagesSurveyhypertensionNiran ThapaNo ratings yet
- Dermato History FormDocument1 pageDermato History Formlaila.forestaNo ratings yet
- PANAMADocument3 pagesPANAMA7vs8ndtrrcNo ratings yet
- Jaundice Symptoms in Adults - Google SearchDocument1 pageJaundice Symptoms in Adults - Google Searchs8903082No ratings yet
- Hospital Claim - Template24 - Page4Document1 pageHospital Claim - Template24 - Page4chamuditha dilshanNo ratings yet
- Patient Medical History (Eng)Document2 pagesPatient Medical History (Eng)desaisaravNo ratings yet
- Form 19Document1 pageForm 19Nurul Huda KhanNo ratings yet
- Abdominal Lab MaterialsDocument11 pagesAbdominal Lab MaterialsPunnam Anurag ReddyNo ratings yet
- Medical Screening Questionnaire: Before You BeginDocument6 pagesMedical Screening Questionnaire: Before You Begins9sxxtjmqjNo ratings yet
- Daniel Cameron Asscoiates New Patient FormsDocument25 pagesDaniel Cameron Asscoiates New Patient Formsjudymw2000No ratings yet
- C105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by AstroDocument5 pagesC105a-Pre-Sea-And-Periodic-Medical-Fitness-Examinations-For-Seafarers - by Astroklinik utama Bali Puri MedikaNo ratings yet
- DSMES Assessment Template (Chart 7)Document5 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Assessment FormDocument8 pagesAssessment FormbonnieyfNo ratings yet
- Health Declaration For Care 4 U Policy / Medical InsuranceDocument2 pagesHealth Declaration For Care 4 U Policy / Medical InsuranceMarco AglibotNo ratings yet
- Questionnaire On Awareness of Diabetes Mellitus Dr. Kanak ChoudhuryDocument3 pagesQuestionnaire On Awareness of Diabetes Mellitus Dr. Kanak ChoudhuryBichayan Debbarma100% (1)
- SDO TARLAC PROVINCE Health Screening and AssessmentDocument2 pagesSDO TARLAC PROVINCE Health Screening and AssessmentKrishna Mae GarciaNo ratings yet
- New Patient/Consultation Form: AllergiesDocument2 pagesNew Patient/Consultation Form: AllergiesAlexander Flores SaraviaNo ratings yet
- New Patient Health History Form: (Please Explain Below)Document2 pagesNew Patient Health History Form: (Please Explain Below)KevinNo ratings yet
- 37981-iUBT311 Treatment Evidence Form v2Document5 pages37981-iUBT311 Treatment Evidence Form v2Aline Brito Ferreira de CastroNo ratings yet
- Legal History and PEDocument1 pageLegal History and PELoreto District Hospital LDHNo ratings yet
- Panama Form F-103 Recording Medical Examinations of Seafarers v. 04Document8 pagesPanama Form F-103 Recording Medical Examinations of Seafarers v. 04Preeti HandaNo ratings yet
- Medical History FormDocument4 pagesMedical History FormevalinadrNo ratings yet
- DIABETES in ELDERLY by Supriyanto KartodarsonoDocument23 pagesDIABETES in ELDERLY by Supriyanto Kartodarsonobryan ruditaNo ratings yet
- Diabetic Retinopathy: From Diagnosis to TreatmentFrom EverandDiabetic Retinopathy: From Diagnosis to TreatmentRating: 3 out of 5 stars3/5 (3)
- Scleroderma Diet: A Beginner's 3-Step Quick Start Guide on Managing Scleroderma Through Diet, With Sample Curated RecipesFrom EverandScleroderma Diet: A Beginner's 3-Step Quick Start Guide on Managing Scleroderma Through Diet, With Sample Curated RecipesNo ratings yet
- GTDocument122 pagesGTAnand Patel100% (1)
- Paramagnetic Oxygen Analyzer PDFDocument5 pagesParamagnetic Oxygen Analyzer PDFAnand PatelNo ratings yet
- Curriculum Vitae: 1.0 Resume Submitted ForDocument3 pagesCurriculum Vitae: 1.0 Resume Submitted ForAnand PatelNo ratings yet
- CV Format Sample - ZADCODocument4 pagesCV Format Sample - ZADCOAnand PatelNo ratings yet
- CV FormatDocument2 pagesCV FormatAnand PatelNo ratings yet
- SafariViewService - Jul 9, 2019 at 09:23Document1 pageSafariViewService - Jul 9, 2019 at 09:23Anand Patel100% (1)
- Checklist For Mechanical CompletionDocument8 pagesChecklist For Mechanical CompletionAnand PatelNo ratings yet
- ID For ABIM - Parham 2014Document140 pagesID For ABIM - Parham 2014Jeronim H'gharNo ratings yet
- Summary of Infectious DiseasesDocument415 pagesSummary of Infectious DiseasesAlston Foods BVNo ratings yet
- (Soal Materi) Summarizing Passage Paket 2Document4 pages(Soal Materi) Summarizing Passage Paket 2aswinmt12No ratings yet
- Chickenpox & ChlamydialDocument5 pagesChickenpox & ChlamydialEliezah RodriguezNo ratings yet
- CSIR Unit 4 - Full NotesDocument80 pagesCSIR Unit 4 - Full NotesSubhrajyoti BanerjeeNo ratings yet
- Herppvc PDFDocument6 pagesHerppvc PDFDr.Chetana INo ratings yet
- Common Communicable DiseasesDocument86 pagesCommon Communicable DiseasesBenj VillanuevaNo ratings yet
- Essential Drugs 2013Document378 pagesEssential Drugs 2013Chedeng KumaNo ratings yet
- June 6, 2013 Mount Ayr Record-NewsDocument14 pagesJune 6, 2013 Mount Ayr Record-NewsMountAyrRecordNewsNo ratings yet
- Virology ModuleDocument165 pagesVirology ModuleAhmed KerAtyNo ratings yet
- Journal Homepage: - : IntroductionDocument8 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Vaccinations: Slam Shraf AhmyDocument11 pagesVaccinations: Slam Shraf AhmyFahad Alkenani100% (1)
- Nclex Random Fact To StudyDocument431 pagesNclex Random Fact To StudyNeko Neko100% (1)
- BDJ Orofacial PainDocument10 pagesBDJ Orofacial PainjayashreeNo ratings yet
- Z - The Clark Zapper Blog & Rife Digital MachinesDocument1 pageZ - The Clark Zapper Blog & Rife Digital MachinescesargnomoNo ratings yet
- Treatment Chronic PainDocument18 pagesTreatment Chronic PainSukedanaNo ratings yet
- Tarlac State University Graduate StudiesDocument4 pagesTarlac State University Graduate StudiesL.J. SantosNo ratings yet
- Comparison of Rubric in KENT, BTPB and BBCRDocument23 pagesComparison of Rubric in KENT, BTPB and BBCRaswathymohan1024No ratings yet
- Varicella & Herpes ZosterDocument33 pagesVaricella & Herpes ZosterRMRNo ratings yet
- Teaching Regarding Measures To Improve Sleep?Document37 pagesTeaching Regarding Measures To Improve Sleep?Martin HusseinNo ratings yet
- Jomo Kenyatta University OF Agriculture & Technology: P.O. Box 62000, 00200 Nairobi, Kenya E-Mail: Elearning@jkuat - Ac.keDocument32 pagesJomo Kenyatta University OF Agriculture & Technology: P.O. Box 62000, 00200 Nairobi, Kenya E-Mail: Elearning@jkuat - Ac.keKeddie OneJhereNo ratings yet
- John Murtaghs General Practice Companion Handbook 7Th Edition John Murtagh Full Chapter PDF ScribdDocument67 pagesJohn Murtaghs General Practice Companion Handbook 7Th Edition John Murtagh Full Chapter PDF Scribdderrick.ayala232100% (7)
- Transfer Factor-Myths and FactsDocument10 pagesTransfer Factor-Myths and FactsIris BetancourtNo ratings yet
- Little Red Riding Hood: A Dermatologic JourneyDocument27 pagesLittle Red Riding Hood: A Dermatologic JourneyjthsNo ratings yet
- Rife RatesDocument17 pagesRife Rateszonetrek100% (1)
- Oral Pathology ModuleDocument31 pagesOral Pathology ModuleDenee Vem MatorresNo ratings yet
- Chickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella ZosterDocument12 pagesChickenpox Chickenpox Is A Highly Contagious Disease Caused by Primary Infection With Varicella Zostersubbu2raj3372100% (2)
- Essential DrugsDocument358 pagesEssential Drugsshahera rosdiNo ratings yet