Professional Documents
Culture Documents
Diagnosis and Management of Systemic Endemic Mycoses Causing Pulmonary Disease
Diagnosis and Management of Systemic Endemic Mycoses Causing Pulmonary Disease
Uploaded by
yovanOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Diagnosis and Management of Systemic Endemic Mycoses Causing Pulmonary Disease
Diagnosis and Management of Systemic Endemic Mycoses Causing Pulmonary Disease
Uploaded by
yovanCopyright:
Available Formats
Review
Respiration 2018;96:283–301 Received: April 23, 2018
Accepted: April 23, 2018
DOI: 10.1159/000489501 Published online: June 28, 2018
Diagnosis and Management of Systemic
Endemic Mycoses Causing Pulmonary
Disease
Helmut J.F. Salzer a, b Gerd Burchard c Oliver A. Cornely d
Christoph Lange a, b, e, f Thierry Rolling c, g Stefan Schmiedel g Michael Libman h
Domenico Capone i, j Thuy Le k, l Margareth P. Dalcolmo m Jan Heyckendorf a, b
a Division of Clinical Infectious Diseases, Research Center Borstel, Borstel, Germany; b German Center for Infection
Research, Clinical Tuberculosis Center, Borstel, Germany; c Bernhard Nocht Institute for Tropical Medicine, Hamburg,
Germany; d Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), Clinical
Trials Centre Cologne (ZKS Köln), University of Cologne and Department I of Internal Medicine, ECMM Excellence
Center of Medical Mycology, University Hospital of Cologne, Cologne, Germany; e International Health/Infectious
Diseases, University of Lübeck, Lübeck, Germany; f Department of Medicine, Karolinska Institutet, Stockholm,
Sweden; g Section of Infectious Diseases and Tropical Medicine, 1st Department of Internal Medicine, University
Medical Centre Hamburg-Eppendorf, Hamburg, Germany; h J.D. MacLean Centre for Tropical Diseases, McGill
University, Montreal, QC, Canada; i Pulmonology and Radiology Services, Rio de Janeiro State University, Rio de
Janeiro, Brazil; j Federal University of Rio de Janeiro, Rio de Janeiro, Brazil; k Division of Infectious Diseases, Duke
University School of Medicine, Durham, NC, USA; l Wellcome Trust Major Overseas Programme, Oxford University
Clinical Research Unit, Ho Chi Minh City, Vietnam; m Helio Fraga Reference Center, FIOCRUZ, Rio de Janeiro, Brazil
Keywords while histoplasmosis and blastomycosis also occur predom-
Endemic mycoses · Pulmonary disease · Diagnosis · inantly in the Americas, these mycoses have also been re-
Management · Treatment ported on other continents, especially in sub-Saharan Africa.
Talaromycosis is endemic in tropical and subtropical regions
in South-East Asia and southern China. Systemic endemic
Abstract mycoses causing pulmonary disease are usually acquired via
Systemic endemic mycoses cause high rates of morbidity the airborne route by inhalation of fungal spores. Infections
and mortality in certain regions of the world and the real im- can range from asymptomatic or mild with flu-like illnesses
pact on global health is not well understood. Diagnosis and to severe pulmonary or disseminated diseases. Skin involve-
management remain challenging, especially in low-preva- ment is frequent in patients with paracoccidioidomycosis,
lence settings, where disease awareness is lacking. The main blastomycosis, sporotrichosis, and talaromycosis and mani-
challenges include the variability of clinical presentation, the fests as localized lesions or diffuse nodules in disseminated
fastidious and slow-growing nature of the fungal pathogens, disease, but can also occur with other endemic mycoses. Cul-
the paucity of diagnostic tests, and the lack of options and ture and/or characteristic histopathology from clinical sam-
toxicity of antifungal drugs. Coccidioidomycosis and para- ples is the diagnostic standard for endemic mycoses. Immu-
coccidioidomycosis are restricted to the Americas only, and nological assays are often not available for the diagnosis of
© 2018 S. Karger AG, Basel Helmut J.F. Salzer, MD, MPH
Division of Clinical Infectious Diseases, Research Center Borstel
Leibniz Lung Center, Parkallee 35
E-Mail karger@karger.com
DE–23845 Borstel (Germany)
www.karger.com/res
E-Mail hsalzer @ fz-borstel.de
most endemic mycoses and molecular amplification meth- systemic endemic mycoses causing pulmonary disease is
ods for the detection of fungal nucleic acids are not stan- challenging, because mycoses may resemble other diseas-
dardized at present. The first-line treatment for mild to mod- es (e.g., pulmonary tuberculosis, bacterial or viral pneu-
erate histoplasmosis, paracoccidioidomycosis, blastomyco- monia, lung cancer) (Fig. 1), and physicians in low-prev-
sis, sporotrichosis, and talaromycosis is itraconazole. Severe alence settings may not be familiar with the disease mani-
illness is treated with amphotericin B. Patients with severe festations. Establishing a diagnosis is further complicated
coccidioidomycosis should receive fluconazole. Treatment by the difficulty in growing these organisms and by the
duration depends on the specific endemic mycosis, the se- paucity of nonculture-based diagnostic assays, specifically
verity of disease, and the immune status of the patient, rang- the lack of standardization of serological and molecular
ing between 6 weeks and lifelong treatment. tests. Pathologists may not be familiar with the histopath-
© 2018 S. Karger AG, Basel ological features. Furthermore, disease management is of-
ten complex, including long-term antifungal treatment,
drug-drug interactions, therapeutic drug monitoring
Introduction (TDM), frequent follow-ups to monitor for antifungal
side effects, and disease relapse and complications.
Systemic endemic mycoses include a group of dimor- The aim of this review is to guide physicians in the di-
phic fungi that are found in distinct geographical regions. agnosis and management of systemic endemic mycoses
Paracoccidioidomycosis and talaromycosis are found in causing pulmonary disease. It should raise awareness
tropical and sub-tropical regions, while coccidioidomy- about important disease characteristics (Tables 1, 2), diag-
cosis is found in warm and dry climates of semi-deserts nostic tests (Table 3), and antifungal treatment (Table 4).
and blastomycosis in temperate climates. Histoplasmosis
occurs under variable conditions ranging from tropical to
temperate climates. The impact of climate change and Disease Characteristics
changes due to migration is uncertain and the real global
burden of endemic mycoses is not well understood [1]. Histoplasmosis
Inhalation of fungal spores may cause infection. Clini- Histoplasmosis caused by the dimorphic fungus His-
cal presentation can vary from asymptomatic to dissemi- toplasma capsulatum is found worldwide, but particular-
nated fatal disease and depends on the immune status of ly in North, Central, and South America (Table 1). It has
the host and the infectious dose from the environmental been reported from parts of southern and eastern Europe,
exposure. Most endemic mycoses, including histoplasmo- Africa, Asia, and Australia; however, reports are usually
sis, coccidioidomycosis, blastomycosis, and sporotricho- limited to a few cases [2]. It has the potential to cause
sis, are capable of causing large outbreaks. Diagnosis of larger outbreaks [3].
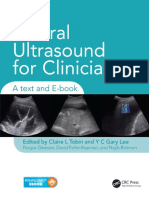
a b
Fig. 1. a Chest X-ray showing macronodular infiltrates in both upper lobes. b Corresponding CT scan of the chest
showing two macronodular consolidations on the right side, smaller nodules, and traction bronchiectasis mim-
icking pulmonary tuberculosis in a patient with histoplasmosis.
284 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
Table 1. Disease characteristics
Species Endemic areas Reservoir Route of Populations Prevention Commentary
transmission at risk
Histoplasmosis Histoplasma capsula- North and Central America, Soil, animal drop- Aerogenic Local population, travelers Immunocompromised Disease severity partly
tum sensu latu Africa (Central, South, West) pings (bats), caves, to endemic regions (visit- individuals should avoid depends on amount of
– Histoplasma capsu- caverns, abandoned ing caves, abandoned activities with disturbing inoculum and host im-
latum var. capsulatum buildings buildings, construction material/soil in regions of mune status
– Histoplasma capsula- works) high prevalence
tum var. duboisi (=
African histoplasmo-
sis)
– Others
Paracocci- Paracoccidioides brasil- South America (Brazil, Peru, Soil Aerogenic Local population, especially Human infections are not In some endemic (rural,
dioidomycosis iensis, Argentina, Colombia, Ecuador, smokers with COPD, work- contagious humid) areas of Brazil
Paracoccidioides lutzii Venezuela) ers in rural areas (e.g., incidence close to 40 cas-
farmers), few cases in trav- es/100,000 inhabitants;
elers very high male to female
ratio
Coccidioido- Coccidioides immitis, Southwestern USA – Arizona Soil of certain arid Aerogenic, inhala- Persons after exposure in Residents can avoid ac- Approximately 2/3 of
mycosis Coccidioides posadasii (66% of cases), central and areas tion of dust (con- endemic regions (highest in tivities that expose them persons experience few or
southern California (31% of struction, landscap- dry periods following a to dust or desert soil and no symptoms
cases), New Mexico, Texas, few ing, farming, ar- rainy season), often associ- stay indoors during dust
cases from Washington, Utah chaeology, ated with outdoor activities storms. Laboratory per-
– Mexico, Central and South excavation, recre- and dust; very rare cases in sonnel handling the or-
America ational pursuits) or travelers ganism should practice
from dust clouds biosafety level 3 precau-
(earthquakes, wind- tions
storms)
Blastomycosis Blastomyces dermatiti- South-Eastern and South-Cen- Soil containing de- Aerogenic, skin No special population, Human infections are not
dis, tral states of the USA and Ca- caying vegetation or inoculation often seen in children, can contagious, immunocom-
Blastomyces gilchristii nadian provinces bordering the decomposed wood, be opportunistic in immu- promised individuals
Great Lakes, and New York associated with wa- nocompromised hosts should avoid activities
state and Canada along the St. terways with disturbing material/
Lawrence River and the Nelson soil in regions of high
River prevalence
Sporotrichosis Sporothrix schenckii, Found worldwide from tem- Soil, moss, decaying Skin inoculation, No special population, Skin protection in people
Sporothrix brasiliensis, perate to tropical climate, en- wood and vegetation aerogenic higher risk for immuno- working in gardening or
Sporothrix globose, demic in Peru compromised patients landscaping
Sporothrix mexicana
Talaromycosis Talaromyces marneffei Southeast Asia, northeastern Bamboo rats, soil in Aerogenic, skin Residents and travelers in Transmission has been
(formally Penicillium India, and southern China bamboo rat burrows, inoculation endemic regions who are reported
marneffei) soil enriched with immunocompromised,
animal excreta especially patients with
advanced HIV infection
AIDS, acquired immune deficiency syndrome; COPD, chronic obstructive pulmonary disease; HIV, human immunodeficiency syndrome.
a b
Fig. 2. Diffuse small nodules in both lungs on chest X-ray (a) and axial CT scan of the chest (b) mimicking mil-
iary tuberculosis in a patient with histoplasmosis.
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 285
Pulmonary Disease DOI: 10.1159/000489501
Table 2. Symptoms and radiological patterns of systemic endemic mycoses causing pulmonary disease
Clinical presentation Most frequent Organ involvements Chest radiological pattern Commentary
symptoms
Histo- – Acute diffuse pulmonary disease Asymptomatic or Pulmonary Diffuse infiltrates, opacities, small or large Immunosuppression as risk
plasmosis (infiltrates) mild “flu-like symptoms” dissemination to any organ nodules, mediastinal mass, cavities (in factor for severe disease with
– Acute localized pulmonary disease (e.g., eye) chronic pulmonary disease), lymph node dissemination (e.g., advanced
(localized infiltrates, mediastinal enlargement HIV infection)
lymphadenopathy)
– Chronic cavitary
– Mediastinal syndromes (e.g., medi-
astinitis, fibrosis)
– Broncholithiasis
– Nodules
Paracoccidio- Acute/subacute form (juvenile) (5– Respiratory symptoms Lymphatic system (lymph nodes, Consolidations (75%), multiple nodules, More severe in immunocom-
idomycosis 25%) Skin lesions liver, spleen, bone marrow, skin, interlobar septal thickening, lymph node promised patients; HIV-infect-
– Lymphadenopathy, hepatospleno- and mucous membranes (45– enlargement (hilar), (very) rarely pleural ed patients more often present
megaly 65%), organ abscess formations, effusion, nodule predominance towards the with fever, lymphadenopathy,
– Cutaneous lesions, fistula formation fever (50–80%), pulmonary inferior pulmonary lobes. hepatosplenomegaly, and cuta-
– Rarely pulmonary involvement (84%), bone (5%), CNS (menin- Nodule diameters from 0.5 to 3 cm with neous lesions
Chronic form (adult) (74–96%) gomyelitis) (2–3%), and adrenal ill-defined contour cavitation, miliary pat- Relapses usually occur within 3
– Pulmonary (77%) gland tern (rare), diffuse interstitial infiltration, years after initial treatment
– Other organs (skin, etc.) posttreatment fibrosis, and scars
Coccidio- Primary infection: mostly with pul- Estimated 2/3 of patients are asymp- Primary infection: lung, pleura, Primary infection: unilateral infiltrate with Radiographic findings may
idomycosis monary involvement tomatic skin, and musculoskeletal hilar adenopathy, parapneumonic effusion, persist for years
Extrapulmonary infection: indolent Fever, cough, chest pain, and arthal- Extrapulmonary: skin and soft tis- thin-walled cavities or nodules Residual pulmonary nodules
course gias in primary infection sue, skeleton, CNS (meninges and Chronic infection: and thin-walled cavities usually
Erythema nodosum spinal cord), eye, heart, liver, coccidioidal cavities (in 2–8% of patients), have no clinical consequences
kidneys, prostate complicated by CPA or abscess formation, Rarely cavity ruptures after
fistulae, persistent pneumonia, chronic fi- years with broncho-pleural
bro-cavitary changes (mixtures of infiltrates, fistula
cavitation, and hilar adenopathy), diffuse More severe in immunocom-
reticulonodular (miliary) pneumonia promised, elderly, diabetes
mellitus, pregnancy
Blastomycosis Pulmonary disease (90%) Pulmonary: nonspecific, cough, fever, Mostly pulmonary, but frequent- Consolidations, interstitial infiltrations,
Extrapulmonary disease night sweats, weight loss, chest pain, ly skin involvement, sometimes nodules and masses, involvement of mul-
and hemoptysis bone and joints, CNS, and geni- tiple or single lobes, less adenopathy
tourinary
Sporotrichosis Lymphocutaneous: most common Lymphocutaneous: ulcerative or Skin and lymphatic, pulmonary,
Pulmonary infection mainly in nodular lesions, lymphangitis osteoarticular, CNS
COPD and alcohol use Pulmonary: fever, cough night
Osteoarticular infection: in particular sweats, weight loss
joints Osteoarticular: pain, swelling, de-
CNS: meningitis is rare creased range of motion, draining
Dissemination: in patients with ad- sinuses in affected joints
vanced HIV infection
Talaromycosis Localized disease: seen in non-HIV- Localized disease: depends on organ Reticuloendothelial system (liver, Interstitial to alveola infiltrates, reticulo-
infected persons involved spleen, lymph nodes, bone mar- nodular pattern, nodules, miliary pattern
Disseminated disease most common Disseminated disease: fever, fatigue, row), skin, pulmonary, gastroin-
in patients with advanced HIV infec- weight loss, lymphadenopathy, hepa- testinal, osteoarticular, CNS
tion tosplenomegaly, skin lesions (primar-
ily on the face)
CNS, central nervous system; CPA, chronic pulmonary aspergillosis; TB, tuberculosis.
Fig. 3. Axial CT scan of the chest showing bipulmonary, solid nod-
ules (white arrows) in a 27-year-old female biology student with
cough and fever lasting for several weeks after returning from a
field trip exploring bat caves in Central America. Diagnosis of pul-
monary histoplasmosis was established by positive culture and
Histoplasma capsulatum var. capsulatum-specific PCR from lung
tissue as well as positive H. capsulatum antibody detection. Histo-
pathology from lung tissue showed noncaseating granulomas with
giant cells, but without evidence of fungi (Grocott’s methenamine
silver stain). Cytology and routine microbiological cultures from
bronchoalveolar lavage fluid revealed no evidence of fungi.
286 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
Table 3. Diagnostic tests to establish diagnosis of endemic mycoses and histological appearance
Culture Histopathology Antigen detection Serology Molecular methods
Histoplasmosis Isolation from clinical specimens Tuberculoid granuloma with intracellular A polyclonal antibody-based antigen test Antibody detection by ID, CF, PCR assays available in
remains gold standard (cave: dan- yeast cells (can be mistaken for trypano- in urine is commercially available in the or Western blot available, high reference laboratories,
ger of laboratory infection by Histo- soma, leishmania amastigotes, or Talaromy- USA; cross-reactivity with other fungal specificity, however, results may not standardized
plasma capsulatum in mycel phase) ces marneffei yeast cells) infections, including Blastomyces dermatiti- be falsely negative in immuno-
dis, CPA may occur; suppressed patients and in those
a monoclonal antibody-based lateral flow who present with acute disease
antigen detection assay is currently under
evaluation
Paracoccioido- Cultures are diagnostic, but can Tuberculoid granuloma with multipolar Antigen detection in BAL has been de- DID, CIE, ELISA, and immu- PCR assays available in
mycosis take up to a month to grow budding yeast cells (“ship-pilot´s wheel” or scribed (gp43, not expressed in Paracoc- noblotting; utility is hampered reference laboratories,
“Mickey Mouse head”) cidioides lutzii), but not standardized by cross-reactivity with other but are not standardized
endemic fungi; inaccuracies in
the diagnosis in P. lutzii infec-
tion.
Coccidioido- Culture confirms the diagnosis; Tuberculoid granuloma with spherules Coccidioides galactomannan antigen test ID and CF; Most clinical infec- PCR assays are being
mycosis Cultures must be manipulated in a (60–100 µm with endospores of 2–5 µm) available in reference laboratories; low tions diagnosed serologically in evaluated
biosafety level III laboratory sensitivity (70%) the setting of a compatible clini-
cal syndrome
Blastomycosis Culture confirms the diagnosis; Tuberculoid granuloma with unipolar EIA for polysaccharide cell wall antigen ID and CF have no role in diag- PCR assays have not been
diagnostic yield is high for both broad-based budding yeast cells commercially available; high sensitivity nosis because poor sensitivity tested in large studies
bronchoscopy and sputum samples, (93%) but low specificity (79%) due to and significant cross reactivity
but takes 1–4 weeks cross-reaction with other fungi
Sporotrichosis Isolation from clinical specimens Necrotizing granulomas, paucity of yeasts Not available One EIA has been developed, PCR‐based assays have
remains gold standard; clinical but is not available been developed, yet to be
specimens should be inoculated on evaluated
Sabouraud agar and incubated at
room temperature for 1–4 weeks
Talaromycosis T. marneffei can be cultured from Binary fission yeasts within histiocytes or EIAs detecting mannoprotein in the fungal Antibody detection by ID, EIA, PCR‐based assays have
blood and other clinical samples, extracellularly; T. marneffei may be con- cell wall in blood and urine, have high or Western blot available; low been developed, low
but can take up to 14 days for iden- fused with H. capsulatum, but has a central sensitivity and specificity but are not com- sensitivity in HIV-infected sensitivities (60–70%),
tification transverse septum unlike any other com- mercially available yet; patients not standardized
mon pathogenic yeasts over 80% of patients with disseminated
talaromycosis are galactomannan antigen
(“Aspergillus spp.”) positive in sera
BAL, bronchoalveolar lavage; CF, complement fixation; CIE, counterimmunoelectrophoresis; CPA, chronic pulmonary aspergillosis; DID, double immunodiffusion technique; EIA, enzyme immunoassay;
ELISA, enzyme-linked immunosorbent assay; ID, immunodiffusion; PCR, polymerase chain reaction.
a b
Fig. 4. a Chest X-ray showing bipulmonary diffuse pulmonary micronodules sparing the periphery in a 50-year-
old HIV-positive male presenting with cough and dyspnea. b Corresponding axial CT scan of the chest showing
diffuse, confluent perihilar pulmonary nodules. Biopsy from ulcerative lesions of the larynx and the anus dem-
onstrated Histoplasma capsulatum.
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 287
Pulmonary Disease DOI: 10.1159/000489501
The clinical manifestations vary depending on the im- acute diffuse pulmonary disease with diffuse infiltrates
mune status of the host and the infectious dose (Table 2). on chest imaging, (2) acute localized pulmonary disease
The disease is usually asymptomatic or manifests as an with localized infiltrates and mediastinal lymphadenop-
acute respiratory illness that is self-limiting in immuno- athy, (3) chronic cavitary pulmonary histoplasmosis, and
competent persons, but it can result in severe illness with (4) mediastinal syndromes (e.g., mediastinitis, fibrosis),
progressive pulmonary disease or disseminated infec- broncholithiasis, or pulmonary nodules (Fig. 1–4) [2, 4].
tion, especially in immunocompromised persons. In Disseminated histoplasmosis occurs primarily in pa-
most cases histoplasmosis presents with various pulmo- tients with underlying immunocompromising disorders,
nary symptoms, often as a subacute pulmonary infection in particular those with impairment of T-cell immunity
3–21 days after exposure. Symptoms are usually mild. such as in HIV infection, in patients who are treated with
Fever, chills, headache, myalgia, anorexia, cough, and TNF-α inhibitors, and in patients with IFN-γ receptor
chest pain may occur in the more heavily exposed indi- deficiency [5, 6]. In endemic areas or in travelers with an
viduals. Pulmonary histoplasmosis is generally classified appropriate travel history, pulmonary histoplasmosis
according to radiographical appearance and includes (1) should be considered as an important differential diag-
Table 4. Treatment regimens for pulmonary endemic mycoses based on available guidelines
Recommended regimen Duration Alternative treatment Commentary
Histoplasmosis Mild to moderate: Itraconazole 200 mg p.o. t.i.d. for 3 days 6–12 weeks Posaconazole 400 mg (oral suspension) b.i.d. – No treatment recommended for mild symptoms <4
(loading dose) followed by 200 mg p.o. once daily or b.i.d. [58] weeks or for pulmonary nodules or broncholithiasis or
Severe: Liposomal amphotericin B 3–5 mg/kg/day IV (pre- Voriconazole 200 mg p.o. b.i.d. [59] mediastinal fibrosis only
ferred) for 2 weeks or until clinical improvement followed by Isavuconazole 200 mg t.i.d. for 2 days, fol- – Oral solution has a better absorption – 12-month
itraconazole (see above) lowed by 200 mg once daily [60] treatment duration is recommended in patients with
or chronic (cavitary) histoplasmosis
Deoxycholate amphotericin B 0.7–1.0 mg/kg/day IV for 1-2 – Surgery (e.g., lobectomy) should be discussed in pa-
weeks or until clinical improvement followed by itraconazole tients with residual pulmonary cavities (CAVE: risk of
(see above) relapse or long-term complications such as CPA)
– Echinocandins are not effective
Paracoccidio- Mild to moderate: Itraconazole 200 mg p.o. once daily 12 months Cotimoxazole 960 mg p.o. b.i.d. or t.i.d. – Cotrimoxazole increases treatment duration to 18–24
idomycosis Severe: Liposomal amphotericin B 3–5 mg/kg/day IV (pre- (9–18 month) months
ferred) until clinical improvement followed by itraconazole (see
above)
or
Deoxycholate amphotericin B 0.5–0.7 mg/kg/day IV until clini-
cal improvement followed by itraconazole (see above)
Coccidio- Mild: No treatment recommended 3–6 months Itraconazole 200 mg p.o. b.i.d. – Patients with a mild disease usually recover without
idomycosis Severe: Fluconazole 400 mg p.o. once daily antifungal treatment
Severe disease in immunocompromised hosts: Liposomal am- 12 months Liposomal amphotericin B 3–5 mg/kg/day IV – Fluconazole has fewer side effects and drug interac-
photericin B 4–6 mg/kg/day plus fluconazole 400 mg daily until tions compared to itraconazole
clinical improvement – Liposomal amphotericin B as an alternative for more
or severe cases
Deoxycholate amphotericin B 0.7–1.0 mg/kg/day IV plus fluco- – Treatment duration of 6–12 months in immunocom-
nazole 400 mg daily until clinical improvement promised patients
Blastomycosis Mild to moderate: Itraconazole 200 mg p.o. t.i.d. for 3 days 6–12 months Fluconazole 400–800 mg p.o. per day – Alternative treatment with ketoconazole or flucon-
(loading dose), followed by 200 mg p.o. b.i.d. Voriconazole 200 to 400 mg p.o. b.i.d. after azole less effective
Severe: Liposomal amphotericin B 3-5 mg/kg/day IV (pre- amphotericin B therapy for CNS disease – CAVE: higher toxicity of ketoconazole
ferred) for 1–2 weeks or until clinical improvement followed by – Voriconazole or posaconazole may also be effective,
itraconazole (see above) but lack of evidence
or
Deoxycholate amphotericin B 0.7–1.0 mg/kg/day IV until clini-
cal improvement followed by itraconazole (see above)
Sporotrichosis Mild to moderate: Itraconazole 200 mg p.o. b.i.d. ≥12 months Fluconazole 400–800 mg p.o. daily – Surgical resection should be discussed
Severe: Liposomal amphotericin B 3–5 mg/kg/day IV until – Alternative treatment less effective
clinical improvement followed by itraconazole (see above)
or
Deoxycholate amphotericin B 0.7–1.0 mg/kg/day IV until clini-
cal improvement followed by itraconazole (see above)
Talaromycosis Regardless of disease severity: Liposomal amphotericin B 3–5 12 weeks Voriconazole 400 mg b.i.d. on day 1 followed – Initial treatment with amphotericin B deoxycholate
mg/kg/day IV for 1–2 weeks followed by itraconazole (see by 200 mg b.i.d. for 12 weeks reduces mortality by 50% compared to itraconazole at 6
above) Itraconazole 200 mg p.o. t.i.d. for 3 days, months in HIV-associated talaromycosis in the IVAP
or followed by 200 mg p.o. b.i.d. for 12 weeks for trial [52]
Deoxycholate amphotericin B 0.7–1.0 mg/kg/day IV for 2 patients unable to tolerate or have no access
weeks or until clinical improvement followed by itraconazole to amphotericin B
(see above)
CPA, chronic pulmonary aspergillosis; b.i.d., twice a day; p.o., per os; t.i.d., three times a day; IV, intravenously.
288 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
nosis to pulmonary tuberculosis, malignancy and sar- current risks of developing chronic pulmonary asper-
coidosis. Extrapulmonary manifestations such as peri- gillosis or pulmonary abscesses, or fistulae as long-term
carditis, arthritis/arthralgia, or erythema nodosum are sequelae [7, 12, 13].
also reported.
Paracoccidioidomycosis
Coccidioidomycosis Paracoccidioidomycosis caused by the dimorphic
Pulmonary coccidioidomycosis (i.e., valley fever) re- fungi Paracoccidioides brasiliensis and Paracoccidioides
fers to pulmonary infection by the dimorphic fungi Coc- lutzii is found in certain parts of South America, espe-
cidioides immitis and Coccidioides posadasii (Table 1). It cially in Brazil, but also in Argentina, Colombia, Ecua-
is endemic in the southwestern parts of the USA (Califor-
nia, Arizona, New Mexico, Utah, and Nevada) and parts
of Central and South America (Mexico, Brazil, Argenti-
Color version available online
na). Outbreaks have been reported in military trainees, in
archeological workers, or have been associated with dust
storms, as well as laboratory-acquired infection [7–11].
Approximately two-thirds of infected persons re-
main asymptomatic or develop self-limiting respiratory
symptoms. When symptomatic, pulmonary involve-
ment is common (>95% of all cases). The most common
clinical manifestations are chest pain, cough, fever,
weight loss, and fatigue, often associated with dermato-
logical manifestations including erythema nodosum
(Fig. 5) or erythema multiforme and rheumatological
manifestations including myalgia and arthralgia. Ra-
diological presentation can vary considerably (Table 2)
(Fig. 6, 7). The disease can spread from the lungs hema-
togenously to bones, joints, skin, and the central ner-
vous system. Some patients have persistent pulmonary
complications including residual pulmonary nodules
(coccidioidomas), fibrosis and cavities, with the con- Fig. 5. Erythema nodosum in a patient with coccidioidomycosis.
a b
Fig. 6. a Chest X-ray of a 30-year-old man with coccidioidomycosis showing bilateral large confluent infiltrates
predominantly located in the lower lung fields. b Corresponding axial CT scan of the chest shows multiple large
nodules. The patient presented with intense asthenia, cough, and chest pain. Clinical symptoms started 7 days
after having participated in armadillo hunting in northeastern Brazil.
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 289
Pulmonary Disease DOI: 10.1159/000489501
dor, Peru, and Venezuela [14, 15]. It is usually seen in manifested by enlarged lymph nodes that can develop
individuals working in rural areas (e.g., farmers). Out- into abscesses or draining fistulae. Important differential
breaks of paracoccidioidomycosis have been reported diagnoses such as visceral leishmaniasis or tuberculosis
[16, 17]. should be considered. The disease can disseminate
Infection is often asymptomatic. Symptomatic disease through the reticuloendothelial system manifested as
is divided in an acute/subacute form and a chronic form. hepatosplenomegaly and bone marrow dysfunction.
The acute form occurs in children and young adults (ju- The chronic (adult) form represents reactivation of the
venile form), develops more rapidly, usually within 45 primary infection and develops over months to years.
days after exposure, is progressive and more severe. Pa- Pulmonary involvement is the most frequent manifesta-
tients present with infection of the lymphatic system, tion, but the disease may affect any other organs
(Fig. 8–10). Patients usually present with dry cough and
dyspnea and can have extensive radiographic findings
varying from localized consolidations, nodules, cavities,
and bilateral infiltrates to chronic findings of septal or
interlobular thickening consistent with fibrosis. Hema-
togenous dissemination to the oropharynx area occurs
over 50% of the time and is manifested as granulomatous
ulcerative oropharyngeal lesions called “mulberry-like”
stomatitis (Fig. 11). Infection by P. brasiliensis occurs
mainly by inhalation. Patients often present with pulmo-
nary symptoms associated with fever, leukocytosis with
hypereosinophilia, and radiological signs of apical pleural
and pulmonary lesions (Fig. 12). Enlarged lymph nodes
Fig. 7. A 50-year-old female traveled for 1 week on a retreat to a are not a common finding, except in children. Immuno-
lodge in the Arizona desert. Eleven days after return, she presented compromised patients such as those with HIV infection,
with cough, dyspnea, and fever. She was diagnosed as having coc- cancer, malnutrition, alcoholism, or drug abuse are at risk
cidioidomycosis. Soon afterwards, she developed typical erythema
nodosum lesions on her legs. Her chest X-ray showed faint reticu-
for the development of disseminated disease with a more
lar opacities in the right upper lobe, as well as a nodular opacity in rapid progression with involvement of the lung, liver,
the right apex. A CT scan shows a cavitating nodule in the right lymph nodes, and skin. Occasionally it is found in travel-
apex. Mediastinal images revealed multiple enlarged lymph nodes. ers [18].
a b
Fig. 8. Axial CT scans of the chest showing various types of lesions of paracoccidioidomycosis in a 42-year-old
farmer presenting with fever, asthenia, severe weight loss, dysphagia, and cough. Physical examination showed
diffuse enlarged lymph nodes, notably in the mid and posterior cervical chains and a small ulcerated lesion in the
pharynx. Microscopy of bronchoalveolar lavage showed Paracoccidioides brasiliensis. a Axial CT scan of the chest
shows nodules associated with ground-glass opacities and consolidations beside cavities with irregular walls.
b The larger cavity on the left side shows a small round mass inside. Basal parts of the lung show peripheral con-
fluent opacities without cavities, some displaying the reverse halo sign.
290 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
Color version available online
a b
Fig. 9. a Fistulated and enlarged cervical lymph node in a 60-year-old farmer from Brazil presenting with cough,
dysphagia, and hoarseness since 6 months. Microscopy of lymph node material revealed Paracoccidioides brasil-
iensis. b Axial CT scan of the chest at the carina level shows nodules and consolidation with a thickened bron-
chovascular bundle (white arrows) in addition to areas of cicatricial emphysema.
Color version available online
a b
c d
Fig. 10. a Chest X-ray showing diffuse micronodular interstitial infiltrates predominantly in the lower fields of
the lung in a 35-year-old farmer in the interior of the state of Rio de Janeiro. He presented with fever for about
40 days, asthenia, and severe weight loss. Immunodiffusion was positive for Paracoccidioides brasiliensis. b For-
ty days later the X-ray showed a progression of the pulmonary lesions with volumetric reduction and hypertrans-
parent images. c Axial CT scan of the chest showing extensive areas of cicatricial emphysema in the left upper
lobe. The patient developed respiratory insufficiency and died. d Postmortem biopsy revealed budding cells of P.
brasiliensis (silver stain).
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 291
Pulmonary Disease DOI: 10.1159/000489501
Color version available online
a b
c d
Fig. 11. a “Mulberry-like” stomatitis in a 44-year-old female patient from Brazil with paracoccidioidomycosis.
She was admitted with the suspicion of oral pharyngeal cancer. b X-ray of the chest showed localized infiltrates
in the lower and middle fields of both lungs (left > right). c Corresponding CT scan of the chest shows localized
consolidations with bounded ground-glass opacities. d After 1 year of antifungal treatment with itraconazole
radiological findings were resolved.
Blastomycosis very diverse radiological findings, which include alveolar
The causative pathogens for blastomycosis are the di- infiltrates, consolidation with or without cavitation, mili-
morphic fungi Blastomyces dermatitidis and Blastomyces tary or reticulonodular patterns, and small pleural effu-
gilchristii, which are found in humid soil containing de- sions. Acute pneumonia can potentially lead to acute re-
caying vegetation or decomposed wood and are associ- spiratory distress syndrome with multiorgan failure and
ated with freshwater drainage basins [19]. It is reported mortality rates of 50%. The clinical appearance of chron-
mainly in North America and in Africa, but occasionally ic blastomycosis pneumonia is similar to tuberculosis,
has also been reported in Central and South America, lung cancer, or histoplasmosis. The radiological pattern
Mexico, India, and the Middle East. Blastomycosis has is often described as alveola or fibronodular infiltrations,
caused a number of outbreaks [20]. mainly with an upper lobe distribution [21]. The absence
After inhalation of the fungus, the most commonly af- of mediastinal lymph node involvement can be helpful in
fected organ is the lung followed by the skin, genitouri- distinguishing blastomycosis from histoplasmosis.
nary tract, and central nervous system (Fig. 13) [21]. Lung
involvement is classified as acute or chronic pneumonia. Sporotrichosis
Acute blastomycosis pneumonia cannot be readily distin- The dimorphic fungus Sporothrix schenckii causes
guished from viral or bacterial pneumonia [21], and has sporotrichosis, a chronic infection mainly found in
292 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
a b c
Fig. 12. Different radiological manifestations of paracoccidioidomycosis in patients coming from rural regions
of Brazil. X-rays of the chest showing extensive consolidating infiltrates of both lungs (a), infiltrates predomi-
nately located in the mid and lower fields of both lungs (b), and a more micronodular pattern of distribution
mimicking miliary tuberculosis (c).
healthy individuals with outdoor activities that involve The infection has an insidious onset over weeks to
inoculation of soil through the skin or subcutaneous tis- months. The clinical symptoms range from mild to mod-
sues such as gardening and landscaping [22, 23]. It is erate infection with localized disease, to disseminated in-
found worldwide in temperate, but also tropical and sub- fection with multiple organ involvement, to severe dis-
tropical areas. Larger outbreaks of sporotrichosis have ease including respiratory failure and shock [31]. The
been reported [24]. most prominent clinical features in HIV-infected pa-
Disseminated disease involving the central nervous sys- tients are fever, weight loss, anemia, generalized lymph-
tem may occur in immunosuppressed patients (e.g. HIV/ adenopathy, hepatomegaly, and splenomegaly [31]. Typ-
AIDS, alcoholism, diabetes) [25]. Infection is either due to ical central umbilicated skin lesions are present in 70% of
inhalation of spores or through skin inoculation. The most HIV-infected and up to 40% of non-HIV-infected pa-
common form is the lympho-cutaneous manifestation, tients and aid in the rapid diagnosis [32]. Besides the skin
which has only mild systemic involvement (Fig. 14). Pul- and reticuloendothelial system involvement, talaromyco-
monary involvement usually occurs in patients with chron- sis often invade the gastrointestinal tract with oropharyn-
ic obstructive pulmonary disease and alcohol use, and pro- geal ulcerations and diarrhea, the pulmonary system with
gresses to death if untreated. Symptoms and radiographic progressive respiratory failure, and occasionally the cen-
appearance are similar to pulmonary tuberculosis and oth- tral nervous system with meningoencephalitis. Arthritis
er chronic fungal infections (Fig. 15) [26]. and osteomyelitis are more commonly observed in non-
HIV-infected patients. The radiological appearance is di-
Talaromycosis verse and includes interstitial to alveolar infiltrates, or
Talaromycosis is caused by the dimorphic fungus Ta- both (Fig. 16), and reticulonodular consolidation, with
laromyces marneffei (formally Penicillium marneffei) and occasionally a miliary pattern similar to tuberculosis
is endemic in South-East Asia, southern China and north- (Fig. 17) [33].
eastern India [27]. Talaromycosis mainly affects immu-
nocompromised patients living or traveling to these re-
gions, in particular patients with advanced HIV infection, Diagnosis
with hematological malignancy, and patients undergoing
immunosuppressive therapy [28, 29]. Although bamboo In low-prevalence settings the diagnostic workup for
rats are a natural reservoir, infection risk is not associated endemic mycoses is challenged by the availability of diag-
with exposure to bamboo rats but is associated with high nostic tests, and will differ widely from site to site. In ad-
humidity and exposure to plants and farmed animals in dition, the positive predictive values of some nonculture-
highland regions [30]. based tests will be significantly lower than in endemic set-
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 293
Pulmonary Disease DOI: 10.1159/000489501
Color version available online
a
b c d
Fig. 13. a, b Chest X-rays of a 42-year-old male resident of Mon- painful skin lesions, unresponsive to several courses of antibacte-
treal, Canada, showing extensive consolidation mostly involving rial agents. Exposures were most like to be in rural regions of
the superior segment (S6) of the right lower lobe. He was also a south-western Quebec (c) and central Manitoba (d), Canada. Bi-
recreational hunter in the region of the St. Laurence river valley. opsy specimens revealed noncaseating granulomatous changes,
He presented with a 2-month history of cough, mild hemoptysis, and cultures from biopsy specimens grew Blastomyces. There were
and intermittent fevers. Biopsy revealed budding yeast cells, and no respiratory symptoms, but in both cases small nodular lesions
culture from a bronchoalveolar lavage grew Blastomyces derma- were seen on pulmonary imaging, which resolved with antifungal
titidis. c, d Two male patients with slowly growing, minimally treatment.
Color version available online
Fig. 14. Slowly progressive skin lesions in a
24-year-old male traveler returning from
several months in India, where he partici-
pated in gardening activities at his resi-
dence. The initial ulcerating verrucous
lesion appeared on the tip of 4th digit,
followed by the appearance of popular/
nodular lesions on the forearm. Culture
from the fingertip ulcer grew Sporothrix
schenkii.
294 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
Color version available online
a
d e
Fig. 15. a Pyogenic and ulcerated cutaneous lesion of thighs of a sizes. c Small nodular cavities can be seen in both lungs, some par-
24-year-old male pig caregiver in Brazil, reported onset of the dis- tially occupied by material with soft tissue density. d A large thick-
ease about 4 months ago complaining of sporadic fever, cough, walled cavity of the left lung with an irregular wall can be seen. e
asthenia, and weight loss. Chest X-ray (b) and axial CT scans (c, Culture of biopsies harvested from the cutaneous lesion demon-
d) show irregularly shaped thick-walled cavitations of different strated growth of Sporothrix schenkii.
tings. As such, awareness of geographical distribution ticularly for coccidioides) requires biosafety level 3
and exposure risks of endemic mycoses, along with case laboratory precautions, and the laboratory should be
discussion involving an interdisciplinary team compris- alerted when infection is suspected. Table 3 summarizes
ing infectious disease specialists, microbiologists, radiol- diagnostic tests to establish the diagnosis of endemic my-
ogists, and pathologists are paramount to making the coses.
diagnosis [34]. Culture of most of these organisms (par-
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 295
Pulmonary Disease DOI: 10.1159/000489501
probably due to a lower fungal burden. Similarly, sensi-
tivity is lower in localized pulmonary disease. Of note,
there is strong cross-reactivity with other endemic myco-
ses such as blastomycosis, paracoccidioidomycosis, and
talaromycosis [38]. Histoplasma sp. contain galactoman-
nan in the cell wall, and may give a positive result in
galactomannan assays used for the diagnosis of asper
gillosis.
(d) Antibody test. Histoplasma-specific antibodies can
be detected either by immunodiffusion, by complement
fixation or by EIA, and a commercial assay is available in
Fig. 16. Progressive bilateral alveola and interstitial infiltrates with
the USA. Due to the time needed for the development of
air bronchogram signs in the left lower lobe in a 32-year-old man specific antibodies (up to 3 months) a negative test does
who presented to the Hospital for Tropical Diseases in Ho Chi not always exclude histoplasmosis. In contrast to antigen
Minh City in 2015 with 2 weeks of fever, weight loss, fatigue, testing, sensitivity is higher in immunocompetent hosts,
cough, difficulty breathing when laying down, abdominal pain, and therefore antigen and antibody are often used togeth-
and diffuse central umbilicated nodules on his face, body, and ex-
tremities. He was diagnosed with HIV and had a CD4 cell count of er to maximize overall sensitivity [38]. The histoplasmin
3 cells/mm3. His skin culture grew Talaromyces marneffei, while delayed-type hypersensitivity skin test is used mainly for
sputum and blood culture showed no growth. epidemiological studies, and is not sufficiently accurate
for use in individual case diagnosis
(e) PCR. Several protocols using a variety of molecular
targets have been described in the literature, but the role
Histoplasmosis for PCR in the diagnostic workup is not yet certain [34].
While evidence is too scarce to recommend a specific Fluorescence in situ hybridization (FISH) has also been
diagnostic scheme, a combination of at least two of the described.
following diagnostic methods seems reasonable:
(a) Histology. Typically, biopsy specimens show tuber- Coccidioidomycosis
culoid granulomas with many polymorphonuclear leuco- Serology is the main method for diagnosing Coccid-
cytes and histiocytes with intracellular yeast cells. Differ- iodes infection in the USA, where EIAs for specific IgM
entiation from tuberculosis or sarcoidosis may be diffi- and IgG are commercially available [39]. A confirmatory
cult – especially in low-prevalence settings. Sensitivity immunodiffusion test should be ordered after a positive
and specificity of histology are highly dependent on the EIA due to higher specificity [40]. In contrast to most
pathologist’s experience, but may be enhanced by fungal other infectious diseases, anti-coccidioidal antibodies
stains, e.g., Gomori methenamine silver and periodic will be positive only in the case of an ongoing or recent
acid–Schiff stains [35]. The tiny yeast forms (approx. infection. A limitation is that antibodies will only form
2 µm) are easily missed. after a latency period of several weeks; therefore the ab-
(b) Culture. Sensitivity depends on the clinical mani- sence of antibodies does not exclude infection in the ear-
festation, the immunity status of the host, and the fungal ly course of illness. Direct microscopic examination of
burden – it is low in patients with acute pulmonary his- clinical specimens and/or culture may be a faster means
toplasmosis [36]. Repeated sputum and/or bronchoalve- of diagnosing Coccidiodes infections [39]. Fungal growth
olar lavage (BAL) and/or bone marrow aspirate for cul- can be observed within 1 week, and identification is fol-
tures and a long incubation period of cultures (up to 6 lowed by a commercially available Genprobe with detects
weeks) may be necessary. C. immitis-specific nucleic acid sequence. To assert dis-
(c) Antigen test. An enzyme immunoassay (EIA) for seminated coccidioidomycosis, it is usually necessary to
detection of H. capsulatum galactomannan from blood, visualize fungi in extrapulmonary biopsy specimens [39].
urine, and BAL is commercially available in the USA [37].
In a multicenter study with 111 patients with proven pro- Paracoccidioidomycosis
gressive disseminated histoplasmosis, the EIA reached a A definite diagnosis of paracoccidioidomycosis can be
sensitivity of 91% and a specificity of 99% in urine [38]. made after direct microscopic examination of the charac-
Sensitivity seems to be lower in immunocompetent hosts, teristic yeast forms in tissue samples (sputum, ascites, bi-
296 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
Color version available online
a b c
Fig. 17. a A 30-year-old man who presented to the Hospital for Tropical Diseases in Ho Chi Minh City in 2013
with 1 month of fever, weight loss of 12 kg, dry cough, shortness of breath, enlarged cervical lymph nodes, hepa-
tosplenomegaly, and multiple central umbilicated nodules on his face and trunk. He was diagnosed with HIV
and had a CD4 count of 12 cells/mm3. b X-ray of the chest showed a diffuse micronodular interstitial pattern
consistent with miliary talaromycosis. Cultures from the lymph node, skin lesions, and blood were all positive
for Talaromyces marneffei. c T. marneffei yeast cells obtained from a Giemsa-stained touch skin smear were seen
under the microscope.
opsies, scraping of skin lesion, etc.) stained with fungal against other endemic mycoses, in particular against his-
stains (large yeast cells surrounded with multipolar bud- toplasmosis [43]. The utility of PCR assays for the detec-
ding daughter cells resembling a “Mickey mouse head” or tion of B. dermatidis has not yet been validated in large
a “steering-wheel”) or by culturing the organism [14]. clinical studies. Finally, similar to histoplasmosis, a single
Culture can take up to 1 month to grow; therefore direct antigen detection assay is available in the USA [44]. The
microscopy remains the cornerstone in the diagnosis of assay has a high sensitivity of around 90%, but also lacks
paracoccidiodes infection. Serological methods, in par- specificity due to cross-reactivity – especially with histo-
ticular the quantitative immunodiffusion method, are plasmosis.
widely available in the endemic regions. However, in
most cases serology is not necessary for diagnosing para- Sporotrichosis
coccidioidomycosis. While it can be a useful tool to mon- Culture is the best option in the diagnostic workup of
itor treatment success, so far serologic diagnosis is not suspected sporotrichosis [45]. Culture is very sensitive,
standardized, and results from different laboratories may and visible growth can be seen within 1 week. S. schenckii
be conflicting [41]. There are no validated serological is not considered a colonizer, thus a positive clinical sam-
techniques for diagnosis of infection with P. lutzii. ple is diagnostic. While histopathology may help in show-
ing a pyogenic and granulomatous picture, the organism
Blastomycosis can only rarely be visualized due to the paucity of or
Direct proof of Blastomyces infection – either by cul- ganisms [45]. No validated serology or PCR is currently
ture or visualization of the yeast forms – is necessary for available.
a definite diagnosis of blastomycosis and the method of
choice [42]. Culturing Blastomyces organisms from respi- Talaromycosis
ratory samples of affected patients has a high sensitivity T. marneffei can be cultured from blood and clinical
of around 90%, but takes 1–4 weeks. Direct microscopic samples using standard media for bacteria culture
examination of typical yeast organisms with broad-based (Fig. 18). As growth may take approximately 1 week, a
buds is characteristic of Blastomyces; however, micros- presumptive diagnosis can be made based on the visual-
copy has a low diagnostic yield of up to 40%. Serological ization of binary fission yeasts on fungal staining of skin
tests for blastomycosis are hampered by their low sensi- scraping, sputum smear, or biopsies [46]. This enables the
tivities and their lack of specificity due to cross-reactivity initiation of antifungal therapy before confirmation of
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 297
Pulmonary Disease DOI: 10.1159/000489501
therapy followed by itraconazole consolidation therapy.
Color version available online
Generally, lipid formulations of amphotericin B are pre-
25°C SDA medium
ferred due to their relatively lower toxicity (infusion re-
lated reactions, renal failure, electrolyte disturbance, and
anemia). High-dose fluconazole is recommended as the
treatment of choice for severe coccidioidomycosis infec-
a b
tions, while patients with a mild disease usually recover
without any antifungal treatment [39]. Little evidence ex-
ists with alternative treatment strategies and the efficacy
of different antifungal drugs can differ considerably be-
37°C SDA medium
tween endemic mycoses and between different manifes-
tations within each endemic mycosis. Table 4 summa-
rizes current antifungal treatment recommendations
according to available guidelines.
c d Duration of Itraconazole Treatment
Duration of itraconazole treatment strongly depends
Fig. 18. Morphology of Talaromyces marneffei colonies on Sab- on the specific endemic mycoses, clinical syndrome, and
ouraud agar (SDA) medium and the fungus under the microscope host immune factors (Table 4). Histoplasmosis and tal-
at 25 ° C (a, b) and at 37 ° C (c, d).
aromycosis usually require a period of 2 weeks of induc-
tion therapy followed by 6–12 weeks of consolidated
treatment, while paracoccidioidomycosis and sporotri-
chosis usually require long-term treatment of at least 12
culture results. Rapid diagnostic assays are being devel- months [14, 51, 52]. Generally, the duration should be
oped including several monoclonal antibody-based anti- guided by clinical improvement and radiological resolu-
gen detection EIAs, which have high sensitivity and spec- tion. For immunosuppressed persons, secondary pro-
ificity, and are being evaluated as rapid diagnostic tests phylaxis is recommended to prevent disease relapse. In
[47, 48]. Real-time PCR assays have been developed but patients with advanced HIV infection, consolidation
sensitivities are currently insufficient (60–70%) to be therapy with itraconazole is recommended until the
clinically useful. CD4+ T-cell count increases and remains above 100 cells/
mm3 for at least 3–6 months on antiretroviral therapy.
Strategies to mitigate the underlying cause of immuno-
Management suppression will dictate the duration of secondary pro-
phylaxis (or consolidation therapy). In persons requiring
For most systemic endemic mycoses causing pulmo- immunosuppressive therapy, management requires a
nary disease including histoplasmosis, paracoccidioido- balance between strategies to mitigate immunosuppres-
mycosis, blastomycosis, sporotrichosis, and talaromyco- sion and lifelong antifungal prophylaxis.
sis, experts generally recommend antifungal treatment The treatment duration for a specific endemic mycosis
with itraconazole. It is the treatment of choice for mild to will differ depending on clinical syndrome and host fac-
moderate disease manifestations (Table 4) [14, 22, 49– tors. Pulmonary histoplasmosis with its different clinical
52]. Mild cases of histoplasmosis with symptoms less than syndromes is an illustrative example. Asymptomatic pa-
4 weeks usually do not require antifungal treatment, while tients with pulmonary nodules usually do not benefit
paracoccidioidomycosis, blastomycosis, sporotrichosis, from antifungal treatment, while symptomatic patients
and talaromycosis should be treated when diagnosed [14, do. Furthermore, patients with acute diffuse pulmonary
22, 50]. Disseminated talaromycoses should be treated as histoplasmosis often require only 6 weeks of antifungal
soon as possible to decrease mortality, and initial therapy treatment, while in patients with chronic cavitary histo-
with amphotericin B deoxycholate has been shown to be plasmosis long-term treatment of at least 12 months is
superior to itraconazole in the IVAP trial in Vietnam recommended. In AIDS patients with pulmonary histo-
[53]. For all endemic mycoses with severe disease mani- plasmosis who do not achieve immune reconstitution
festations, amphotericin B is recommended as initial even lifelong treatment may be recommended [54].
298 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
Dosage of Itraconazole Treatment Follow-Up and Complications
The commonly recommended dosage for itraconazole Azoles strongly influence the enzymatic activity of cy-
consolidation treatment is 200 mg once to twice daily de- tochrome P450 (e.g., CYP3A4), which can lead to consid-
pending on the severity of disease (Table 4). Generally, erable drug-drug interactions [56]. TDM can assist in de-
the oral solution of itraconazole is preferred due to the tecting subtherapeutic drug concentrations due to mal
improved absorption compared to capsules and tablets. absorption and drug-drug interaction and in optimizing
However, the itraconazole solution is not well tolerated individual dosage regimes. Treatment monitoring and
due to the osmotic effect of the co-formulated cyclodex- patient follow-up are essential to detect antifungal side
trin [54]. Gastric acid is required for adequate absorption effects, drug-drug interactions, treatment failure, and
of the capsules and tablets, so they should be taken im- pulmonary sequelae. Long-term sequelae such as chronic
mediately after meals or with an acidic drink. Antacids pulmonary aspergillosis should be considered in patients
should be avoided or taken at least 4–6 h apart from itra- with cavitary destruction of lung parenchyma [12, 57].
conazole tablets and capsules. The oral solution of itra- Symptoms may persist for several months and a lung
conazole, however, should be taken on an empty stom- function test (usually showing an obstructive pattern)
ach. It is recommended to start itraconazole treatment may help to monitor the course of disease.
with a loading dose of 200 mg 3 times a day for 3 days to
attain adequate drug levels more rapidly. The manufac-
turer labeling recommends a loading dose only for severe Conclusions
and life-threatening cases, but in these cases the guide-
lines usually recommend initial therapy with amphoteri- This review article should guide physicians in the di-
cin B intravenously until clinical improvement before agnosis and management of systemic endemic mycoses
continuation with oral itraconazole. Because of the vari- causing pulmonary disease. Several aspects have to be
able bioavailability and the potential for drug-drug inter- considered.
actions, TDM is recommended, especially for patients First, clinical presentation and radiological pattern of
who have severe disease, critically ill patients in intensive systemic endemic mycoses may mimic other diseases and
care unit, patients on multiple drugs including rifampicin are nonspecific. The medical history plays a central role,
and antiretroviral therapy with nonnucleoside reverse especially the travel history and information on risk fac-
transcriptase inhibitors and protease inhibitors, and pa- tors for potential environmental exposures. Having a
tients with infections of the central nervous system, eyes clinical suspicion is critical as it facilitates specific myco-
or bones. However, TDM is not universally available and logical diagnostics and communication with laboratory
several limitations have to be considered (e.g., assays are personnel on potential biosafety risk (in particular for
not standardized, optimal timing of sampling, sample Coccidioides spp.). Physicians need to be aware of basic
transportation, unclear reference values) [55]. disease manifestations and the diversity of clinical and
radiological patterns.
Amphotericin B Treatment Second, even when an endemic mycosis is suspected,
Early intravenous amphotericin B treatment is recom- diagnoses may be hampered by the lack of availability of
mended for most severe cases of systemic endemic myco- diagnostic tests, especially in low-prevalence settings.
ses (Table 4). Generally, lipid-formulated amphotericin B Consultation with a mycology reference laboratory is rea-
is preferred due to reduced toxicity. However, in many sonable to discuss proper sample collection and available
resource-constrained settings, lipid-formulated ampho- diagnostic tests. Test results should be interpreted with
tericin B is not available or affordable. Deoxycholate am- consideration for their performance and for the lower
photericin B still remains an effective alternative, but positive predictive values of some of these tests in com-
nephrotoxicity is common and should be closely moni- parison to what are reported from endemic regions. Cul-
tored. Toxicity is significantly mitigated by daily saline ture or histology from clinical samples (e.g., BAL, lung
and potassium supplementation. The commonly recom- tissue) is the method of choice for most endemic mycoses.
mended duration of amphotericin B treatment is 1–2 A combination of different diagnostic methods is reason-
weeks, but strongly depends on the severity of disease and able, and may increase the likelihood of establishing a di-
the clinical condition of the patient. After clinical stabili- agnosis.
zation of the patient treatment should be changed to itra- Third, if antifungal treatment is indicated itraconazole
conazole. (or fluconazole in the case of coccidioidomycoses) is the
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 299
Pulmonary Disease DOI: 10.1159/000489501
treatment of choice in mild to moderate cases, except for In low-prevalence settings it is advisable to discuss pa-
talaromycosis, where amphotericin B should be the initial tients with suspected endemic mycoses with an interdis-
treatment. Early amphotericin B therapy (preferably lipid ciplinary team involving infectious disease specialists,
formulations) is recommended in severe cases until clin- microbiologists, radiologists, and pathologists.
ical stabilization of the patient before changing to itra-
conazole consolidation therapy. Drug-drug interactions,
adverse events, and possible long-term sequelae should Disclosure Statement
be monitored. Duration of treatment differs significantly
between endemic mycoses and depends on the specific The authors have no conflicts of interest to declare.
mycoses, severity of disease, clinical syndrome, and the
immune status of the hosts.
References
1 Mirsaeidi M, Motahari H, Taghizadeh 10 Petersen LR, Marshall SL, Barton-Dickson C, 18 Panackal AA, Hajjeh RA, Cetron MS, War-
Khamesi M, Sharifi A, Campos M, Schraufna- Hajjeh RA, Lindsley MD, Warnock DW, Pan- nock DW: Fungal infections among returning
gel DE: Climate change and respiratory infec- ackal AA, Shaffer JB, Haddad MB, Fisher FS, travelers. Clin Infect Dis 2002;35:1088–1095.
tions. Ann Am Thorac Soc 2016; 13: 1223– Dennis DT, Morgan J: Coccidioidomycosis 19 McTaggart LR, Brown EM, Richardson SE:
1230. among workers at an archeological site, Phylogeographic analysis of Blastomyces der-
2 Wheat LJ, Conces D, Allen SD, Blue-Hnidy D, northeastern Utah. Emerg Infect Dis 2004;10: matitidis and Blastomyces gilchristii reveals an
Loyd J: Pulmonary histoplasmosis syn- 637–642. association with North American freshwater
dromes: recognition, diagnosis, and manage- 11 Williams PL, Sable DL, Mendez P, Smyth LT: drainage basins. PLoS One 2016;11:e0159396.
ment. Semin Respir Crit Care Med 2004; 25: Symptomatic coccidioidomycosis following a 20 Roy M, Benedict K, Deak E, Kirby MA, Mc
129–144. severe natural dust storm. An outbreak at the Niel JT, Sickler CJ, Eckardt E, Marx RK, Hef-
3 Benedict K, Derado G, Mody RK: Histoplas- Naval Air Station, Lemoore, Calif. Chest fernan RT, Meece JK, Klein BS, Archer JR,
mosis-associated hospitalizations in the Unit- 1979;76:566–570. Theurer J, Davis JP, Park BJ: A large commu-
ed States, 2001–2012. Open Forum Infect Dis 12 Osaki T, Morishita H, Maeda H, Kamei K, nity outbreak of blastomycosis in Wisconsin
2016;3:ofv219. Hoshino S, Kijima T, Kumagai T, Yoshida M, with geographic and ethnic clustering. Clin
4 Capone D, Wanke B, Monteiro PC, Lazera Tachibana I, Kawase I: Pulmonary coccidioi- Infect Dis 2013;57:655–662.
MS, de Noronha Andrade G, do Valle AC, domycosis that formed a fungus ball with 21 Azar MM, Assi R, Relich RF, Schmitt BH,
Moreno AM, Londero AT: Chronic pulmo- 8-years duration. Intern Med 2005; 44: 141– Norris S, Wheat LJ, Hage CA: Blastomycosis
nary histoplasmosis in the state of Rio de Ja- 144. in Indiana: clinical and epidemiologic pat-
neiro, Brazil. Mycopathologia 1999; 145: 75– 13 Capone D, Marchiori E, Wanke B, Dantas KE, terns of disease gleaned from a multicenter
79. Cavalcanti MA, Deus Filho A, Escuissato DL, retrospective study. Chest 2015; 148: 1276–
5 Hage CA, Bowyer S, Tarvin SE, Helper D, Warszawiak D: Acute pulmonary coccidioi- 1284.
Kleiman MB, Wheat LJ: Recognition, diagno- domycosis: CT findings from 15 patients. Br J 22 Kauffman CA, Bustamante B, Chapman SW,
sis, and treatment of histoplasmosis compli- Radiol 2008;81:721–724. Pappas PG; Infectious Diseases Society of
cating tumor necrosis factor blocker therapy. 14 Shikanai-Yasuda MA, Mendes RP, Colombo America: Clinical practice guidelines for the
Clin Infect Dis 2010;50:85–92. AL, Queiroz-Telles F, Kono ASG, Paniago management of sporotrichosis: 2007 update
6 Zerbe CS, Holland SM: Disseminated histo- AM, Nathan A, Valle A, Bagagli E, Benard G, by the Infectious Diseases Society of America.
plasmosis in persons with interferon-gamma Ferreira MS, Teixeira MM, Silva-Vergara ML, Clin Infect Dis 2007;45:1255–1265.
receptor 1 deficiency. Clin Infect Dis 2005; Pereira RM, Cavalcante RS, Hahn R, Durlach- 23 Kauffman CA: Sporotrichosis. Clin Infect Dis
41:e38–e41. er RR, Khoury Z, Camargo ZP, Moretti ML, 1999;29:231–236; quiz 237.
7 Galgiani JN, Ampel NM, Blair JE, Catanzaro Martinez R: Brazilian guidelines for the clini- 24 Sanchotene KO, Madrid IM, Klafke GB, Ber-
A, Johnson RH, Stevens DA, Williams PL; In- cal management of paracoccidioidomycosis. gamashi M, Della Terra PP, Rodrigues AM, de
fectious Diseases Society of America: Coccid- Rev Soc Bras Med Trop 2017;50:715–740. Camargo ZP, Xavier MO: Sporothrix brasil-
ioidomycosis. Clin Infect Dis 2005; 41: 1217– 15 Bethlem EP, Capone D, Maranhao B, Carv- iensis outbreaks and the rapid emergence of
1223. alho CR, Wanke B: Paracoccidioidomycosis. feline sporotrichosis. Mycoses 2015; 58: 652–
8 Nicas M: A point-source outbreak of Coccid- Curr Opin Pulm Med 1999;5:319–325. 658.
ioidomycosis among a highway construction 16 Barrozo LV, Benard G, Silva ME, Bagagli E, 25 Pluss JL, Opal SM: Pulmonary sporotrichosis:
crew. J Occup Environ Hyg 2018;15:57–62. Marques SA, Mendes RP: First description of review of treatment and outcome. Medicine
9 Crum N, Lamb C, Utz G, Amundson D, Wal- a cluster of acute/subacute paracoccidioido- (Baltimore) 1986;65:143–153.
lace M: Coccidioidomycosis outbreak among mycosis cases and its association with a cli- 26 Aung AK, Teh BM, McGrath C, Thompson
united states navy seals training in a Coccidi- matic anomaly. PLoS Negl Trop Dis 2010; PJ: Pulmonary sporotrichosis: case series and
oides immitis-endemic area – Coalinga, Cali- 4:e643. systematic analysis of literature on clinico-ra-
fornia. J Infect Dis 2002;186:865–868. 17 do Valle ACF, Marques de Macedo P, Almei- diological patterns and management out-
da-Paes R, Romao AR, Lazera MDS, Wanke comes. Med Mycol 2013;51:534–544.
B: Paracoccidioidomycosis after highway
construction, Rio de Janeiro, Brazil. Emerg
Infect Dis 2017;23:1917–1919.
300 Respiration 2018;96:283–301 Salzer et al.
DOI: 10.1159/000489501
27 Vanittanakom N, Cooper CR Jr, Fisher MC, Alapat D, Babady NE, Parker M, Fuller D, Kauffman CA; Infectious Diseases Society of
Sirisanthana T: Penicillium marneffei infec- Noor A, Davis TE, Rodgers M, Connolly PA, America: Clinical practice guidelines for the
tion and recent advances in the epidemiology El Haddad B, Wheat LJ: A multicenter evalu- management of blastomycosis: 2008 update
and molecular biology aspects. Clin Micro- ation of tests for diagnosis of histoplasmosis. by the Infectious Diseases Society of America.
biol Rev 2006;19:95–110. Clin Infect Dis 2011;53:448–454. Clin Infect Dis 2008;46:1801–1812.
28 Le T, Wolbers M, Chi NH, Quang VM, Chinh 39 Galgiani JN, Ampel NM, Blair JE, Catanzaro 51 Queiroz-Telles F, Fahal AH, Falci DR, Cace-
NT, Lan NP, Lam PS, Kozal MJ, Shikuma CM, A, Geertsma F, Hoover SE, Johnson RH, res DH, Chiller T, Pasqualotto AC: Neglected
Day JN, Farrar J: Epidemiology, seasonality, Kusne S, Lisse J, MacDonald JD, Meyerson endemic mycoses. Lancet Infect Dis 2017;
and predictors of outcome of aids-associated SL, Raksin PB, Siever J, Stevens DA, Sunen- 17:e367–e377.
Penicillium marneffei infection in Ho Chi shine R, Theodore N: 2016 Infectious Diseas- 52 Le T, Kinh NV, Cuc NTK, Tung NLN, Lam
Minh City, Vietnam. Clin Infect Dis 2011;52: es Society of America (IDSA) clinical practice NT, Thuy PTT, Cuong DD, Phuc PTH, Vinh
945–952. guideline for the treatment of coccidioidomy- VH, Hanh DTH, Tam VV, Thanh NT, Thuy
29 Chan JF, Chan TS, Gill H, Lam FY, Trendell- cosis. Clin Infect Dis 2016;63:e112–e146. TP, Hang NT, Long HB, Nhan HT, Wertheim
Smith NJ, Sridhar S, Tse H, Lau SK, Hung IF, 40 Kuberski T, Herrig J, Pappagianis D: False- HFL, Merson L, Shikuma C, Day JN, Chau
Yuen KY, Woo PC: Disseminated infections positive IGM serology in coccidioidomycosis. NVV, Farrar J, Thwaites G, Wolbers M; IVAP
with Talaromyces marneffei in non-AIDS pa- J Clin Microbiol 2010;48:2047–2049. Investigators: A trial of itraconazole or am-
tients given monoclonal antibodies against 41 Vidal MS, Del Negro GM, Vicentini AP, Svid- photericin B for HIV-associated talaromyco-
CD20 and kinase inhibitors. Emerg Infect Dis zinski TI, Mendes-Giannini MJ, Almeida AM, sis. N Engl J Med 2017;376:2329–2340.
2015;21:1101–1106. Martinez R, de Camargo ZP, Taborda CP, Be- 53 Ranjana KH, Priyokumar K, Singh TJ, Gupta
30 Chariyalertsak S, Sirisanthana T, Supparat- nard G: Serological diagnosis of paracoccidi- Ch C, Sharmila L, Singh PN, Chakrabarti A:
pinyo K, Praparattanapan J, Nelson KE: Case- oidomycosis: high rate of inter-laboratorial Disseminated Penicillium marneffei infection
control study of risk factors for Penicillium variability among medical mycology reference among HIV-infected patients in Manipur
marneffei infection in human immunodefi- centers. PLoS Negl Trop Dis 2014;8:e3174. state, India. J Infect 2002;45:268–271.
ciency virus-infected patients in northern 42 Saccente M, Woods GL: Clinical and labora- 54 Kauffman CA: Histoplasmosis: a clinical and
Thailand. Clin Infect Dis 1997;24:1080–1086. tory update on blastomycosis. Clin Microbiol laboratory update. Clin Microbiol Rev 2007;
31 Supparatpinyo K, Khamwan C, Baosoung V, Rev 2010;23:367–381. 20:115–132.
Nelson KE, Sirisanthana T: Disseminated 43 Davies SF, Sarosi GA: Serodiagnosis of histo- 55 Salzer HJ, Wassilew N, Kohler N, Olaru ID,
Penicillium marneffei infection in southeast plasmosis and blastomycosis. Am Rev Respir Gunther G, Herzmann C, Kalsdorf B, San-
Asia. Lancet 1994;344:110–113. Dis 1987;136:254–255. chez-Carballo P, Terhalle E, Rolling T,
32 Kawila R, Chaiwarith R, Supparatpinyo K: 44 Durkin M, Witt J, LeMonte A, Wheat B, Con- Lange C, Heyckendorf J: Personalized med-
Clinical and laboratory characteristics of Pen- nolly P: Antigen assay with the potential to aid icine for chronic respiratory infectious dis-
icilliosis marneffei among patients with and in diagnosis of blastomycosis. J Clin Micro- eases: tuberculosis, nontuberculous myco-
without HIV infection in northern Thailand: biol 2004;42:4873–4875. bacterial pulmonary diseases, and chronic
a retrospective study. BMC Infect Dis 2013; 45 Barros MB, de Almeida Paes R, Schubach AO: pulmonary aspergillosis. Respiration 2016;
13:464. Sporothrix schenckii and sporotrichosis. Clin 92: 199–214.
33 Duong TA: Infection due to Penicillium Microbiol Rev 2011;24:633–654. 56 Dvorak Z: Drug-drug interactions by azole
marneffei, an emerging pathogen: review of 46 Supparatpinyo K, Chiewchanvit S, Hirunsri antifungals: beyond a dogma of CYP3A4 en-
155 reported cases. Clin Infect Dis 1996; 23: P, Uthammachai C, Nelson KE, Sirisanthana zyme activity inhibition. Toxicol Lett 2011;
125–130. T: Penicillium marneffei infection in patients 202:129–132.
34 Azar MM, Hage CA: Laboratory diagnostics infected with human immunodeficiency vi- 57 Salzer HJ, Heyckendorf J, Kalsdorf B, Rolling
for histoplasmosis. J Clin Microbiol 2017; 55: rus. Clin Infect Dis 1992;14:871–874. T, Lange C: Characterization of patients with
1612–1620. 47 Chaiyaroj SC, Chawengkirttikul R, Sirisinha chronic pulmonary aspergillosis according to
35 Bialek R, Ernst F, Dietz K, Najvar LK, Knob- S, Watkins P, Srinoulprasert Y: Antigen de- the new ESCMID/ERS/ECMM and IDSA
loch J, Graybill JR, Schaumburg-Lever G: tection assay for identification of Penicillium guidelines. Mycoses 2017;60:136–142.
Comparison of staining methods and a nested marneffei infection. J Clin Microbiol 2003;41: 58 Restrepo A, Tobon A, Clark B, Graham DR,
PCR assay to detect Histoplasma capsulatum 432–434. Corcoran G, Bradsher RW, Goldman M, Pan-
in tissue sections. Am J Clin Pathol 2002;117: 48 Wang YF, Cai JP, Wang YD, Dong H, Hao W, key G, Moore T, Negroni R, Graybill JR:
597–603. Jiang LX, Long J, Chan C, Woo PC, Lau SK, Salvage treatment of histoplasmosis with
36 Weydert JA, Van Natta TL, DeYoung BR: Yuen KY, Che XY: Immunoassays based on posaconazole. J Infect 2007;54:319–327.
Comparison of fungal culture versus surgical Penicillium marneffei Mp1p derived from Pi- 59 Freifeld A, Proia L, Andes D, Baddour LM,
pathology examination in the detection of chia pastoris expression system for diagnosis Blair J, Spellberg B, Arnold S, Lentnek A,
histoplasma in surgically excised pulmonary of penicilliosis. PLoS One 2011;6:e28796. Wheat LJ: Voriconazole use for endemic fun-
granulomas. Arch Pathol Lab Med 2007;131: 49 Wheat LJ, Freifeld AG, Kleiman MB, Baddley gal infections. Antimicrob Agents Chemother
780–783. JW, McKinsey DS, Loyd JE, Kauffman CA; 2009;53:1648–1651.
37 Theel ES, Jespersen DJ, Harring J, Mandrekar Infectious Diseases Society of America: Clini- 60 Thompson GR 3rd, Rendon A, Ribeiro Dos
J, Binnicker MJ: Evaluation of an enzyme im- cal practice guidelines for the management of Santos R, Queiroz-Telles F, Ostrosky-Zeich-
munoassay for detection of Histoplasma cap- patients with histoplasmosis: 2007 update by ner L, Azie N, Maher R, Lee M, Kovanda L,
sulatum antigen from urine specimens. J Clin the Infectious Diseases Society of America. Engelhardt M, Vazquez JA, Cornely OA, Per-
Microbiol 2013;51:3555–3559. Clin Infect Dis 2007;45:807–825. fect JR: Isavuconazole treatment of crypto-
38 Hage CA, Ribes JA, Wengenack NL, Baddour 50 Chapman SW, Dismukes WE, Proia LA, coccosis and dimorphic mycoses. Clin Infect
LM, Assi M, McKinsey DS, Hammoud K, Bradsher RW, Pappas PG, Threlkeld MG, Dis 2016;63:356–362.
Systemic Endemic Mycoses Causing Respiration 2018;96:283–301 301
Pulmonary Disease DOI: 10.1159/000489501
You might also like
- Oms Informe Tecnico 53Document303 pagesOms Informe Tecnico 53Javier Caviedes100% (3)
- Respiratory MycosisDocument20 pagesRespiratory MycosisNivedita MishraNo ratings yet
- Histoplasmosis AtsDocument4 pagesHistoplasmosis Atsanabella081096No ratings yet
- Clinical Presentation and Bacterial Etiology of Adult Community Acquired PneumoniaDocument7 pagesClinical Presentation and Bacterial Etiology of Adult Community Acquired PneumonialyaNo ratings yet
- Pneumocystis Jiroveci: Jay A. Fishman, MDDocument17 pagesPneumocystis Jiroveci: Jay A. Fishman, MDIsmael Armando Collantes DiazNo ratings yet
- Pneumonia ComunitariaDocument10 pagesPneumonia ComunitariaMaulida HalimahNo ratings yet
- Non-Tuberculous Mycobacterial Pulmonary Infections: ReviewDocument12 pagesNon-Tuberculous Mycobacterial Pulmonary Infections: Reviewmgoez077No ratings yet
- Tuberculosis Thesis IntroductionDocument8 pagesTuberculosis Thesis Introductionifywpqvcf100% (2)
- PHD Thesis TuberculosisDocument8 pagesPHD Thesis TuberculosisBecky Goins100% (2)
- DTSCH Arztebl Int-116 0435Document16 pagesDTSCH Arztebl Int-116 0435JoshuaNo ratings yet
- Medical Mycology Case ReportsDocument4 pagesMedical Mycology Case ReportsSebastián Garay HuertasNo ratings yet
- Histoplasmosis Review INF DIS CLIN NA 2021Document21 pagesHistoplasmosis Review INF DIS CLIN NA 2021Tatiana DiazNo ratings yet
- Vervloet Et Al-2007-Brazilian Journal of Infectious DiseasesDocument8 pagesVervloet Et Al-2007-Brazilian Journal of Infectious DiseasesCynthia GalloNo ratings yet
- NeumoniaDocument28 pagesNeumoniaresidentes isssteNo ratings yet
- Grunewald 2019Document22 pagesGrunewald 2019Josver PretellNo ratings yet
- Benefit of CT Scanning For Assessing Pulmonary Disease in The Immunodepressed PatientDocument6 pagesBenefit of CT Scanning For Assessing Pulmonary Disease in The Immunodepressed PatienthilalNo ratings yet
- 2021 - TorresDocument28 pages2021 - TorresCarlosNo ratings yet
- Lectura 4 Seminario Micosis ProfundaDocument3 pagesLectura 4 Seminario Micosis ProfundaAlessandra Saravia PachecoNo ratings yet
- LungIndia323241-4636559 125245Document5 pagesLungIndia323241-4636559 125245Nishant AggarwalNo ratings yet
- Woolfrey2012 PDFDocument22 pagesWoolfrey2012 PDFJorge BarriosNo ratings yet
- SarcoidosisDocument22 pagesSarcoidosisveerraju tvNo ratings yet
- Lecture 2 On FUNGAL INFECTIONSDocument49 pagesLecture 2 On FUNGAL INFECTIONSAMIT GUPTANo ratings yet
- 6.2. NeumoníaDocument5 pages6.2. NeumoníaErmilo José Echeverría OrtegónNo ratings yet
- Primer: BronchiectasisDocument18 pagesPrimer: BronchiectasisAnanta Bryan Tohari WijayaNo ratings yet
- Multi Drug Resistant TBDocument28 pagesMulti Drug Resistant TBmedeviNo ratings yet
- Respiratory and Pulmonary Medicine: ClinmedDocument5 pagesRespiratory and Pulmonary Medicine: ClinmedPutri Zeahan Ramadhini YedismanNo ratings yet
- Principles of Management of Odontogenic InfectionsDocument99 pagesPrinciples of Management of Odontogenic InfectionsdanocprexoidNo ratings yet
- Endemic Mycoses: Blastomycosis, Histoplasmosis, and SporotrichosisDocument18 pagesEndemic Mycoses: Blastomycosis, Histoplasmosis, and SporotrichosisaugustosavioNo ratings yet
- Pulmonary Endemic MycosesDocument4 pagesPulmonary Endemic MycosesFamilia CarbajalNo ratings yet
- International Journal of Infectious DiseasesDocument5 pagesInternational Journal of Infectious Diseasesbe a doctor for you Medical studentNo ratings yet
- Biofilm InfectionsDocument25 pagesBiofilm InfectionsMaria Jose Calero GNo ratings yet
- 10 Atypical PneumoniaDocument4 pages10 Atypical PneumoniaKevinTevesYupanquiNo ratings yet
- Cshperspectmed HFP A019299Document14 pagesCshperspectmed HFP A019299windaNo ratings yet
- Antibiotics and Palliative CareDocument6 pagesAntibiotics and Palliative CareRahmanu ReztaputraNo ratings yet
- J Clin Tuberc Other Mycobact Dis: SciencedirectDocument6 pagesJ Clin Tuberc Other Mycobact Dis: SciencedirectDian Putri NingsihNo ratings yet
- Infections in The Neutropenic Patient-2001Document27 pagesInfections in The Neutropenic Patient-2001Raisa_90No ratings yet
- Petri1997 Article EpidemiologyOfInvasiveMycosisIDocument9 pagesPetri1997 Article EpidemiologyOfInvasiveMycosisIMuhamed RamadanNo ratings yet
- Advance in Pediatric DentistryDocument6 pagesAdvance in Pediatric DentistryAgtadila NovitanandaNo ratings yet
- Extrapulmonary TuberculosisDocument76 pagesExtrapulmonary Tuberculosisqayyum consultantfpscNo ratings yet
- ECMM Guidelines For MucormycosisDocument17 pagesECMM Guidelines For MucormycosisSaurabh AgrawalNo ratings yet
- 149 FullDocument10 pages149 Fullসোমনাথ মহাপাত্রNo ratings yet
- Chapter 126 - PneumoniaDocument23 pagesChapter 126 - PneumoniamnnicolasNo ratings yet
- FullDocument17 pagesFullambiebieNo ratings yet
- PneumoniaDocument10 pagesPneumoniaAubrey PerezNo ratings yet
- Thesis Pulmonary TuberculosisDocument5 pagesThesis Pulmonary TuberculosisDoMyPaperCanada100% (2)
- TracheitisDocument7 pagesTracheitisÁlvaro DezaNo ratings yet
- Thesis Tuberculosis PDFDocument7 pagesThesis Tuberculosis PDFlanawetschsiouxfalls100% (1)
- Epidemiological Profile of Acute Typical Bacterial Pneumonia at The National Reference University Hospital Center of NDjamena Risk Factors and Antibiotic ResistanceDocument13 pagesEpidemiological Profile of Acute Typical Bacterial Pneumonia at The National Reference University Hospital Center of NDjamena Risk Factors and Antibiotic ResistanceAthenaeum Scientific PublishersNo ratings yet
- Bieber, T.Document7 pagesBieber, T.Anak Agung Ayu Ira Kharisma Buana Undiksha 2019No ratings yet
- Antibioticoterapia Na Pneumonia Pediátrica 2006Document7 pagesAntibioticoterapia Na Pneumonia Pediátrica 2006Tainah__100% (1)
- Covid 19 ResearchDocument3 pagesCovid 19 ResearchTahpehs PhiriNo ratings yet
- Lee Et Al 2001 Case Report Meningococcal MeningitisDocument3 pagesLee Et Al 2001 Case Report Meningococcal MeningitisAsmae OuissadenNo ratings yet
- Defenisi PDFDocument2 pagesDefenisi PDFNyoman SuryaNo ratings yet
- Approach To The Immunocompromised Patient With Fever and Pulmonary Infiltrates - UpToDateDocument40 pagesApproach To The Immunocompromised Patient With Fever and Pulmonary Infiltrates - UpToDateJúlio ZoéNo ratings yet
- Neumococo en NacDocument15 pagesNeumococo en NacMNo ratings yet
- Community-Acquired Bacterial Meningitis (Van de Beek)Document13 pagesCommunity-Acquired Bacterial Meningitis (Van de Beek)gaz.med20No ratings yet
- Nosocomial Pneumonia: Self AssessmentDocument10 pagesNosocomial Pneumonia: Self AssessmentZali AhmadNo ratings yet
- Epidemiology and Clinical Manifestations of Mucormycosis CMIDocument9 pagesEpidemiology and Clinical Manifestations of Mucormycosis CMIDINESH VENKATESANNo ratings yet
- Basic Concepts On Communityacquired Bacterial Pneumonia in PediatricsDocument6 pagesBasic Concepts On Communityacquired Bacterial Pneumonia in PediatricsJesselle LasernaNo ratings yet
- Fimmu 09 02219Document13 pagesFimmu 09 02219skgs1970No ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- 2014 CCM-AClinicalClassificationoftheARDSDocument9 pages2014 CCM-AClinicalClassificationoftheARDSyovanNo ratings yet
- Consideration of Severe Coronavirus Disease 2019.12Document5 pagesConsideration of Severe Coronavirus Disease 2019.12yovanNo ratings yet
- Pleural Diseases (Libro) PDFDocument522 pagesPleural Diseases (Libro) PDFEdgard Eduardo Azañero EstradaNo ratings yet
- 4 5823498057307652490 PDFDocument161 pages4 5823498057307652490 PDFyovanNo ratings yet
- Accepted Manuscript: SmokehazDocument40 pagesAccepted Manuscript: SmokehazyovanNo ratings yet
- Pulmonary Thromboembolism Presenting With Abdominal SymptomsDocument3 pagesPulmonary Thromboembolism Presenting With Abdominal SymptomsyovanNo ratings yet
- Jbcxfjsrydt 7689 Yoyfdtuyiouyugchfjyupihcvhgjuyoi YgcmhluipyghvjkiDocument12 pagesJbcxfjsrydt 7689 Yoyfdtuyiouyugchfjyupihcvhgjuyoi YgcmhluipyghvjkiyovanNo ratings yet
- Edema IbefqwehfbqwhiefbweefhvqwfwqefqwejfbDocument3 pagesEdema IbefqwehfbqwhiefbweefhvqwfwqefqwejfbyovanNo ratings yet
- Ni Hms Merg Jweg Ljwe Bfgipwnfpwibg 1693lbfweDocument14 pagesNi Hms Merg Jweg Ljwe Bfgipwnfpwibg 1693lbfweyovanNo ratings yet
- Case ConceptualizationsDocument6 pagesCase ConceptualizationsRachelJoyBaloloy100% (1)
- Overview of The Company A. CategoryDocument4 pagesOverview of The Company A. CategoryJustineNo ratings yet
- Halamang GamotDocument7 pagesHalamang GamotHazel UntalanNo ratings yet
- UveitisDocument90 pagesUveitisfranceseyemd89% (9)
- Miasms: Reaction Patterns in Chronic DiseaseDocument21 pagesMiasms: Reaction Patterns in Chronic DiseaseShukan MankadNo ratings yet
- Lotf Week 2 PacketDocument22 pagesLotf Week 2 Packetapi-260262236No ratings yet
- Herbesser IVDocument24 pagesHerbesser IVsuho exoNo ratings yet
- Committee Opinion: Preparing For Clinical Emergencies in Obstetrics and GynecologyDocument3 pagesCommittee Opinion: Preparing For Clinical Emergencies in Obstetrics and GynecologyMochammad Rizal AttamimiNo ratings yet
- APA Guidelines On The Prevention of Postoperative Vomiting in ChildrenDocument35 pagesAPA Guidelines On The Prevention of Postoperative Vomiting in ChildrenMaria Lucia RossiNo ratings yet
- How To Speak So People Really Listen Sample ChapterDocument25 pagesHow To Speak So People Really Listen Sample ChapterCapstone PublishingNo ratings yet
- J Jacc 2020 11 018Document173 pagesJ Jacc 2020 11 018Ashvanee sharmaNo ratings yet
- Chapter 2 - Social CognitionDocument20 pagesChapter 2 - Social CognitionG. S.No ratings yet
- Recalls 6: Nursing Practice 5: Pero Dying NaDocument8 pagesRecalls 6: Nursing Practice 5: Pero Dying NasaguiguitpNo ratings yet
- Chain of Infection: Mr. Migron Rubin M.Sc. Nursing StudentDocument43 pagesChain of Infection: Mr. Migron Rubin M.Sc. Nursing StudentJarnel CabalsaNo ratings yet
- Best Herbs To Use For Pre Treatment Foot BathDocument3 pagesBest Herbs To Use For Pre Treatment Foot BathAndreas PapazachariouNo ratings yet
- Senbazuru Details and InstructionsDocument10 pagesSenbazuru Details and InstructionsShoeb KarimNo ratings yet
- Stroke MimikDocument48 pagesStroke MimikRafiqy Sa'adiy FaizunNo ratings yet
- HONEYDocument15 pagesHONEYSHIVANI KUMARINo ratings yet
- 101 Reasons Why Im A VegetarianDocument16 pages101 Reasons Why Im A Vegetarianvesna1313No ratings yet
- Statement of The Problem: Scope and DelimitationDocument4 pagesStatement of The Problem: Scope and DelimitationAbsquatulateNo ratings yet
- Drug Therapy in Nursing 3e Test BankDocument4 pagesDrug Therapy in Nursing 3e Test Bankmichaelstricklandcpbtqxjasr100% (52)
- Low Blood PressureDocument2 pagesLow Blood PressurebambangNo ratings yet
- Terebinthiniae Oleum: Other Names: Made FromDocument30 pagesTerebinthiniae Oleum: Other Names: Made FromDohn Joe100% (1)
- Introduction of The ResearchDocument3 pagesIntroduction of The Researchcristine baldazoNo ratings yet
- Introduction To NCBI ResourcesDocument39 pagesIntroduction To NCBI ResourcescgonzagaaNo ratings yet
- IhiwehifkyhiowlkeDocument37 pagesIhiwehifkyhiowlkeshilaroshanNo ratings yet
- RBCs Abnormal MorphologyDocument33 pagesRBCs Abnormal MorphologyLailitifa Windy SNo ratings yet
- Congenital GlaucomasDocument17 pagesCongenital GlaucomasKenny SetiawanNo ratings yet
- Emory Cardiology Newsletter June 2009Document9 pagesEmory Cardiology Newsletter June 2009hnaguNo ratings yet