
Wound Assestment
Wound Assestment
You might also like
- Dermatology Essentials for Medical AssistantsFrom EverandDermatology Essentials for Medical AssistantsRating: 4 out of 5 stars4/5 (1)
- 50 Multiple ChoiceDocument11 pages50 Multiple ChoiceMac Chi Le Nu83% (6)
- Iggy Med Surg Test Bank Chapter 005Document19 pagesIggy Med Surg Test Bank Chapter 005Tracy Bartell80% (10)
- Oral Maxillofacial Surgery Displacement Complications: Gerald Alexander,, Hany AttiaDocument8 pagesOral Maxillofacial Surgery Displacement Complications: Gerald Alexander,, Hany AttiaKamilla MoraisNo ratings yet
- NURS 270 Midterm #1 Blueprint ReviewDocument25 pagesNURS 270 Midterm #1 Blueprint ReviewAgajddNo ratings yet
- Skin Care PowerpointDocument52 pagesSkin Care Powerpointisapatrick812667% (3)
- Wound Documentation TipsDocument2 pagesWound Documentation TipsDonna Balch Sardina100% (1)
- Emdr Final DraftDocument15 pagesEmdr Final Draftapi-506581034No ratings yet
- Sbar Template RN ToDocument2 pagesSbar Template RN ToInes100% (2)
- Types of Medication OrdersDocument2 pagesTypes of Medication OrdersAndrei Caraiman67% (3)
- Wound Care: The BasicsDocument26 pagesWound Care: The Basicsomar abdulrauofNo ratings yet
- Wound Care The BasicsDocument26 pagesWound Care The BasicsIntan Purnamasari100% (1)
- Wound CareDocument17 pagesWound CareLestia AgustinaNo ratings yet
- Wound Care 1Document12 pagesWound Care 1Afril CadagNo ratings yet
- 4 Wounds and Wound CareDocument25 pages4 Wounds and Wound Caredoc-fahad aftabNo ratings yet
- Suturing WorkshopDocument87 pagesSuturing WorkshopVictor OpreaNo ratings yet
- Complex Wounds 2020Document38 pagesComplex Wounds 2020Ài ZìjǐNo ratings yet
- Nursing Care For Patient With Wound Nursing Care For Patient With WoundDocument48 pagesNursing Care For Patient With Wound Nursing Care For Patient With Woundayu triaNo ratings yet
- Technical Writing Assign 2Document8 pagesTechnical Writing Assign 2Miss DNo ratings yet
- Wound Care: Presentation For ACC Lab March 22, 2006Document19 pagesWound Care: Presentation For ACC Lab March 22, 2006heka_amrongNo ratings yet
- Nursing Care For Patient With Wound: by PurwaningsihDocument48 pagesNursing Care For Patient With Wound: by Purwaningsihzaenal abidinNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- Principles of Wound Care: Professor Claire HaleDocument20 pagesPrinciples of Wound Care: Professor Claire HaleMACPANAMERANo ratings yet
- Pressure Ulcer CareDocument39 pagesPressure Ulcer CareRosalyn YuNo ratings yet
- Basic SurgeryDocument52 pagesBasic SurgeryMusabbirNo ratings yet
- Safari - 26 Mar 2023, 11:28 AMDocument1 pageSafari - 26 Mar 2023, 11:28 AMErza KabashiNo ratings yet
- Chapter 6 WoundhealingDocument41 pagesChapter 6 WoundhealingMelba AlanoNo ratings yet
- Wound Classification and Care 2022 KD LEDGEDocument35 pagesWound Classification and Care 2022 KD LEDGEamandaNo ratings yet
- Wound ManagementDocument6 pagesWound ManagementBianca Corina MusatNo ratings yet
- Nursing Aspect - Wound ManagementDocument54 pagesNursing Aspect - Wound ManagementBbieSyg Usagi Tsukino0% (1)
- SKINDocument12 pagesSKINJaleah Gwyneth Fernandez EdullantesNo ratings yet
- WoundsDocument40 pagesWoundsDr Sania SardarNo ratings yet
- SuturingDocument40 pagesSuturingAldora OktavianaNo ratings yet
- Skin Integrity and Wound CareDocument38 pagesSkin Integrity and Wound CareMiu MiuNo ratings yet
- Cheat Sheet 2Document5 pagesCheat Sheet 2Katelyn HillNo ratings yet
- Debridement of Pressure UlcersDocument10 pagesDebridement of Pressure UlcersMa. Mechile MartinezNo ratings yet
- Skin Integrity Epidermis-Multiple Layers, Stratum Corneum - ThinDocument11 pagesSkin Integrity Epidermis-Multiple Layers, Stratum Corneum - ThinsakonzNo ratings yet
- Tissue Integrity and Wound CarestudentDocument38 pagesTissue Integrity and Wound Carestudentbernard arcigaNo ratings yet
- Skin IntegrityDocument112 pagesSkin IntegrityHerlina NababanNo ratings yet
- Wound Dressing: Nor Afifi Syafika Binti Mohd NasirDocument55 pagesWound Dressing: Nor Afifi Syafika Binti Mohd NasirlekhaNo ratings yet
- NCM 103 - Topic 5 - Wound CareDocument66 pagesNCM 103 - Topic 5 - Wound CareChalle MontemayorNo ratings yet
- Case Summary Pediatrics32 5-Year-ODocument12 pagesCase Summary Pediatrics32 5-Year-OMaryam FadahNo ratings yet
- WoundsDocument69 pagesWoundssamNo ratings yet
- Ulcer and Its ManagementDocument19 pagesUlcer and Its ManagementSaad Ur Rahman 9 DNo ratings yet
- Skin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxDocument92 pagesSkin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxAT4-11 HUMSS 2 CEDRICK ILAO100% (1)
- Wound DressingDocument26 pagesWound DressingIkram HossainNo ratings yet
- Pressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyDocument40 pagesPressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyjyothiNo ratings yet
- Approach To A Dermatologic PatientDocument3 pagesApproach To A Dermatologic PatientJessica Febrina WuisanNo ratings yet
- Physical Examination of The SkinDocument4 pagesPhysical Examination of The SkinJessica Febrina WuisanNo ratings yet
- Wound Care IntroductionDocument4 pagesWound Care IntroductionNikki Ann Kanapi FernandezNo ratings yet
- Wound and Skin Ulcer Management Care Guide PDFDocument21 pagesWound and Skin Ulcer Management Care Guide PDFAdriel Chandra AngNo ratings yet
- Basic First AidDocument16 pagesBasic First AidDanica DolorNo ratings yet
- Skinhairnail Ass 1Document43 pagesSkinhairnail Ass 1Airene Aquino BusaniaNo ratings yet
- Emilio Aguinaldo College: Case StudyDocument12 pagesEmilio Aguinaldo College: Case StudyEldonVinceIsidroNo ratings yet
- 08-Skin TumoursDocument8 pages08-Skin TumoursChris Tan100% (1)
- Wound Assessment & CareDocument32 pagesWound Assessment & Caresami siddiqNo ratings yet
- Wound NoteDocument16 pagesWound NoteofasusiNo ratings yet
- Anatomy ProjectDocument7 pagesAnatomy Projecthala sadeddinNo ratings yet
- Wound Care IntroductionDocument11 pagesWound Care IntroductionJasmine JacobNo ratings yet
- Derma Notes 1 June 15Document6 pagesDerma Notes 1 June 15diviNo ratings yet
- Pathophysiology and Prevention of Scar Tissues - NataDocument45 pagesPathophysiology and Prevention of Scar Tissues - Natadenybudiman04100% (1)
- Wound AssessmentDocument4 pagesWound Assessmentonlyabc123No ratings yet
- RNSG 1413wounds Fall2006Document67 pagesRNSG 1413wounds Fall2006api-3697326100% (1)
- Skin Injury: Dr. Imam FirmansyahDocument28 pagesSkin Injury: Dr. Imam FirmansyahVanquish VeinNo ratings yet
- Sebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Diagast Duffy Fyb 78015 IgmDocument4 pagesDiagast Duffy Fyb 78015 Igmthuydungyct146No ratings yet
- Hospital & Clinical Pharmacy Q&ADocument22 pagesHospital & Clinical Pharmacy Q&AKrishan KumarNo ratings yet
- CAE Healthcare: Your Worldwide Training Partner of ChoiceDocument39 pagesCAE Healthcare: Your Worldwide Training Partner of Choicejfrías_2No ratings yet
- Moderate SedationDocument39 pagesModerate SedationRiZqi Rufi100% (1)
- Biomedical Instrumentation: COURSE CODE: 15EC1148Document2 pagesBiomedical Instrumentation: COURSE CODE: 15EC1148hema maliniNo ratings yet
- Signed Paramedicine Agreement With DOH - EsteroDocument32 pagesSigned Paramedicine Agreement With DOH - EsteroNews-PressNo ratings yet
- OXYGEN THERAPY AND HUMIDIFICATION G4 Minor1 PPPDocument73 pagesOXYGEN THERAPY AND HUMIDIFICATION G4 Minor1 PPPChris ZantiraNo ratings yet
- 2how To Use Homeopathic RemediesDocument7 pages2how To Use Homeopathic RemediesTom JoadNo ratings yet
- IMEC Series IntroductionDocument49 pagesIMEC Series IntroductionNicolas NeffaNo ratings yet
- LX Medif-Form enDocument2 pagesLX Medif-Form enmoulimraan786No ratings yet
- Standards of Practice For Interventional Radiology and Interventional NeuroradiologyDocument37 pagesStandards of Practice For Interventional Radiology and Interventional NeuroradiologybethNo ratings yet
- Patient Assessment ToolDocument2 pagesPatient Assessment ToolRachael93% (41)
- Systemic and Local Applications of Steroids in Endodontics: An Update ReviewDocument8 pagesSystemic and Local Applications of Steroids in Endodontics: An Update ReviewJorge OrbeNo ratings yet
- S P S D: Chizoid Ersonality Tyle and IsorderDocument10 pagesS P S D: Chizoid Ersonality Tyle and Isordergraceprimasari0% (1)
- OsteoarthritisDocument4 pagesOsteoarthritisdrnareshNo ratings yet
- Merenstein Gardners Handbook of Neonatal Intensive Care 8Th Edition Sandra Lee Gardner Brian S Carter Mary I Enzman Hines Jacinto A Hernandez Download PDF ChapterDocument52 pagesMerenstein Gardners Handbook of Neonatal Intensive Care 8Th Edition Sandra Lee Gardner Brian S Carter Mary I Enzman Hines Jacinto A Hernandez Download PDF Chapterrichard.martin380100% (18)
- GERIATRIC HEALTH PresentationDocument40 pagesGERIATRIC HEALTH Presentationapi-19712253No ratings yet
- R G C I & R C: Ajiv Andhi Ancer NstituteDocument7 pagesR G C I & R C: Ajiv Andhi Ancer NstituteShubham JainNo ratings yet
- El Kersh2015Document8 pagesEl Kersh2015Sathoodeh BanuNo ratings yet
- Complete Urine Examination (CUE), Urine: MR.P V Rama RaoDocument19 pagesComplete Urine Examination (CUE), Urine: MR.P V Rama RaoGautam PendyalaNo ratings yet
- Tumor Pituitari: Pembimbing: Ervita Yuda, DR., SPPD, M.Kes Davin Takaryanto, DRDocument34 pagesTumor Pituitari: Pembimbing: Ervita Yuda, DR., SPPD, M.Kes Davin Takaryanto, DRDavin TakaryantoNo ratings yet
- Formularium 2020Document5 pagesFormularium 2020primamedikaNo ratings yet
- CAGE QuestionnaireDocument1 pageCAGE QuestionnaireRaluca MariaNo ratings yet
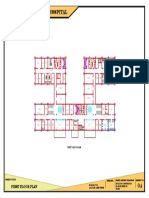
- 100 Bedded General Hospital: First Floor PlanDocument1 page100 Bedded General Hospital: First Floor PlanAshish chauhanNo ratings yet
























































































Download as pdf or txt
You might also like
- Dermatology Essentials for Medical AssistantsFrom EverandDermatology Essentials for Medical AssistantsRating: 4 out of 5 stars4/5 (1)
- 50 Multiple ChoiceDocument11 pages50 Multiple ChoiceMac Chi Le Nu83% (6)
- Iggy Med Surg Test Bank Chapter 005Document19 pagesIggy Med Surg Test Bank Chapter 005Tracy Bartell80% (10)
- Oral Maxillofacial Surgery Displacement Complications: Gerald Alexander,, Hany AttiaDocument8 pagesOral Maxillofacial Surgery Displacement Complications: Gerald Alexander,, Hany AttiaKamilla MoraisNo ratings yet
- NURS 270 Midterm #1 Blueprint ReviewDocument25 pagesNURS 270 Midterm #1 Blueprint ReviewAgajddNo ratings yet
- Skin Care PowerpointDocument52 pagesSkin Care Powerpointisapatrick812667% (3)
- Wound Documentation TipsDocument2 pagesWound Documentation TipsDonna Balch Sardina100% (1)
- Emdr Final DraftDocument15 pagesEmdr Final Draftapi-506581034No ratings yet
- Sbar Template RN ToDocument2 pagesSbar Template RN ToInes100% (2)
- Types of Medication OrdersDocument2 pagesTypes of Medication OrdersAndrei Caraiman67% (3)
- Wound Care: The BasicsDocument26 pagesWound Care: The Basicsomar abdulrauofNo ratings yet
- Wound Care The BasicsDocument26 pagesWound Care The BasicsIntan Purnamasari100% (1)
- Wound CareDocument17 pagesWound CareLestia AgustinaNo ratings yet
- Wound Care 1Document12 pagesWound Care 1Afril CadagNo ratings yet
- 4 Wounds and Wound CareDocument25 pages4 Wounds and Wound Caredoc-fahad aftabNo ratings yet
- Suturing WorkshopDocument87 pagesSuturing WorkshopVictor OpreaNo ratings yet
- Complex Wounds 2020Document38 pagesComplex Wounds 2020Ài ZìjǐNo ratings yet
- Nursing Care For Patient With Wound Nursing Care For Patient With WoundDocument48 pagesNursing Care For Patient With Wound Nursing Care For Patient With Woundayu triaNo ratings yet
- Technical Writing Assign 2Document8 pagesTechnical Writing Assign 2Miss DNo ratings yet
- Wound Care: Presentation For ACC Lab March 22, 2006Document19 pagesWound Care: Presentation For ACC Lab March 22, 2006heka_amrongNo ratings yet
- Nursing Care For Patient With Wound: by PurwaningsihDocument48 pagesNursing Care For Patient With Wound: by Purwaningsihzaenal abidinNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- Principles of Wound Care: Professor Claire HaleDocument20 pagesPrinciples of Wound Care: Professor Claire HaleMACPANAMERANo ratings yet
- Pressure Ulcer CareDocument39 pagesPressure Ulcer CareRosalyn YuNo ratings yet
- Basic SurgeryDocument52 pagesBasic SurgeryMusabbirNo ratings yet
- Safari - 26 Mar 2023, 11:28 AMDocument1 pageSafari - 26 Mar 2023, 11:28 AMErza KabashiNo ratings yet
- Chapter 6 WoundhealingDocument41 pagesChapter 6 WoundhealingMelba AlanoNo ratings yet
- Wound Classification and Care 2022 KD LEDGEDocument35 pagesWound Classification and Care 2022 KD LEDGEamandaNo ratings yet
- Wound ManagementDocument6 pagesWound ManagementBianca Corina MusatNo ratings yet
- Nursing Aspect - Wound ManagementDocument54 pagesNursing Aspect - Wound ManagementBbieSyg Usagi Tsukino0% (1)
- SKINDocument12 pagesSKINJaleah Gwyneth Fernandez EdullantesNo ratings yet
- WoundsDocument40 pagesWoundsDr Sania SardarNo ratings yet
- SuturingDocument40 pagesSuturingAldora OktavianaNo ratings yet
- Skin Integrity and Wound CareDocument38 pagesSkin Integrity and Wound CareMiu MiuNo ratings yet
- Cheat Sheet 2Document5 pagesCheat Sheet 2Katelyn HillNo ratings yet
- Debridement of Pressure UlcersDocument10 pagesDebridement of Pressure UlcersMa. Mechile MartinezNo ratings yet
- Skin Integrity Epidermis-Multiple Layers, Stratum Corneum - ThinDocument11 pagesSkin Integrity Epidermis-Multiple Layers, Stratum Corneum - ThinsakonzNo ratings yet
- Tissue Integrity and Wound CarestudentDocument38 pagesTissue Integrity and Wound Carestudentbernard arcigaNo ratings yet
- Skin IntegrityDocument112 pagesSkin IntegrityHerlina NababanNo ratings yet
- Wound Dressing: Nor Afifi Syafika Binti Mohd NasirDocument55 pagesWound Dressing: Nor Afifi Syafika Binti Mohd NasirlekhaNo ratings yet
- NCM 103 - Topic 5 - Wound CareDocument66 pagesNCM 103 - Topic 5 - Wound CareChalle MontemayorNo ratings yet
- Case Summary Pediatrics32 5-Year-ODocument12 pagesCase Summary Pediatrics32 5-Year-OMaryam FadahNo ratings yet
- WoundsDocument69 pagesWoundssamNo ratings yet
- Ulcer and Its ManagementDocument19 pagesUlcer and Its ManagementSaad Ur Rahman 9 DNo ratings yet
- Skin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxDocument92 pagesSkin - Hair.Nails Head & Neck Eyes. Ears. Nose. Sinuses Mouth. PharynxAT4-11 HUMSS 2 CEDRICK ILAO100% (1)
- Wound DressingDocument26 pagesWound DressingIkram HossainNo ratings yet
- Pressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyDocument40 pagesPressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyjyothiNo ratings yet
- Approach To A Dermatologic PatientDocument3 pagesApproach To A Dermatologic PatientJessica Febrina WuisanNo ratings yet
- Physical Examination of The SkinDocument4 pagesPhysical Examination of The SkinJessica Febrina WuisanNo ratings yet
- Wound Care IntroductionDocument4 pagesWound Care IntroductionNikki Ann Kanapi FernandezNo ratings yet
- Wound and Skin Ulcer Management Care Guide PDFDocument21 pagesWound and Skin Ulcer Management Care Guide PDFAdriel Chandra AngNo ratings yet
- Basic First AidDocument16 pagesBasic First AidDanica DolorNo ratings yet
- Skinhairnail Ass 1Document43 pagesSkinhairnail Ass 1Airene Aquino BusaniaNo ratings yet
- Emilio Aguinaldo College: Case StudyDocument12 pagesEmilio Aguinaldo College: Case StudyEldonVinceIsidroNo ratings yet
- 08-Skin TumoursDocument8 pages08-Skin TumoursChris Tan100% (1)
- Wound Assessment & CareDocument32 pagesWound Assessment & Caresami siddiqNo ratings yet
- Wound NoteDocument16 pagesWound NoteofasusiNo ratings yet
- Anatomy ProjectDocument7 pagesAnatomy Projecthala sadeddinNo ratings yet
- Wound Care IntroductionDocument11 pagesWound Care IntroductionJasmine JacobNo ratings yet
- Derma Notes 1 June 15Document6 pagesDerma Notes 1 June 15diviNo ratings yet
- Pathophysiology and Prevention of Scar Tissues - NataDocument45 pagesPathophysiology and Prevention of Scar Tissues - Natadenybudiman04100% (1)
- Wound AssessmentDocument4 pagesWound Assessmentonlyabc123No ratings yet
- RNSG 1413wounds Fall2006Document67 pagesRNSG 1413wounds Fall2006api-3697326100% (1)
- Skin Injury: Dr. Imam FirmansyahDocument28 pagesSkin Injury: Dr. Imam FirmansyahVanquish VeinNo ratings yet
- Sebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandSebaceous Cyst, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Diagast Duffy Fyb 78015 IgmDocument4 pagesDiagast Duffy Fyb 78015 Igmthuydungyct146No ratings yet
- Hospital & Clinical Pharmacy Q&ADocument22 pagesHospital & Clinical Pharmacy Q&AKrishan KumarNo ratings yet
- CAE Healthcare: Your Worldwide Training Partner of ChoiceDocument39 pagesCAE Healthcare: Your Worldwide Training Partner of Choicejfrías_2No ratings yet
- Moderate SedationDocument39 pagesModerate SedationRiZqi Rufi100% (1)
- Biomedical Instrumentation: COURSE CODE: 15EC1148Document2 pagesBiomedical Instrumentation: COURSE CODE: 15EC1148hema maliniNo ratings yet
- Signed Paramedicine Agreement With DOH - EsteroDocument32 pagesSigned Paramedicine Agreement With DOH - EsteroNews-PressNo ratings yet
- OXYGEN THERAPY AND HUMIDIFICATION G4 Minor1 PPPDocument73 pagesOXYGEN THERAPY AND HUMIDIFICATION G4 Minor1 PPPChris ZantiraNo ratings yet
- 2how To Use Homeopathic RemediesDocument7 pages2how To Use Homeopathic RemediesTom JoadNo ratings yet
- IMEC Series IntroductionDocument49 pagesIMEC Series IntroductionNicolas NeffaNo ratings yet
- LX Medif-Form enDocument2 pagesLX Medif-Form enmoulimraan786No ratings yet
- Standards of Practice For Interventional Radiology and Interventional NeuroradiologyDocument37 pagesStandards of Practice For Interventional Radiology and Interventional NeuroradiologybethNo ratings yet
- Patient Assessment ToolDocument2 pagesPatient Assessment ToolRachael93% (41)
- Systemic and Local Applications of Steroids in Endodontics: An Update ReviewDocument8 pagesSystemic and Local Applications of Steroids in Endodontics: An Update ReviewJorge OrbeNo ratings yet
- S P S D: Chizoid Ersonality Tyle and IsorderDocument10 pagesS P S D: Chizoid Ersonality Tyle and Isordergraceprimasari0% (1)
- OsteoarthritisDocument4 pagesOsteoarthritisdrnareshNo ratings yet
- Merenstein Gardners Handbook of Neonatal Intensive Care 8Th Edition Sandra Lee Gardner Brian S Carter Mary I Enzman Hines Jacinto A Hernandez Download PDF ChapterDocument52 pagesMerenstein Gardners Handbook of Neonatal Intensive Care 8Th Edition Sandra Lee Gardner Brian S Carter Mary I Enzman Hines Jacinto A Hernandez Download PDF Chapterrichard.martin380100% (18)
- GERIATRIC HEALTH PresentationDocument40 pagesGERIATRIC HEALTH Presentationapi-19712253No ratings yet
- R G C I & R C: Ajiv Andhi Ancer NstituteDocument7 pagesR G C I & R C: Ajiv Andhi Ancer NstituteShubham JainNo ratings yet
- El Kersh2015Document8 pagesEl Kersh2015Sathoodeh BanuNo ratings yet
- Complete Urine Examination (CUE), Urine: MR.P V Rama RaoDocument19 pagesComplete Urine Examination (CUE), Urine: MR.P V Rama RaoGautam PendyalaNo ratings yet
- Tumor Pituitari: Pembimbing: Ervita Yuda, DR., SPPD, M.Kes Davin Takaryanto, DRDocument34 pagesTumor Pituitari: Pembimbing: Ervita Yuda, DR., SPPD, M.Kes Davin Takaryanto, DRDavin TakaryantoNo ratings yet
- Formularium 2020Document5 pagesFormularium 2020primamedikaNo ratings yet
- CAGE QuestionnaireDocument1 pageCAGE QuestionnaireRaluca MariaNo ratings yet
- 100 Bedded General Hospital: First Floor PlanDocument1 page100 Bedded General Hospital: First Floor PlanAshish chauhanNo ratings yet