Download as pdf or txt
You might also like
- About KFC: Especially For MalaysiansDocument11 pagesAbout KFC: Especially For MalaysiansSiti Zalikha Md Jamil0% (2)
- MeningoceleDocument33 pagesMeningoceleAnkira Findoro100% (1)
- Dr. Yoyos - Acute Cervical Injury FinalDocument30 pagesDr. Yoyos - Acute Cervical Injury FinalRsud Malinau Ppk BludNo ratings yet
- Pectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPectus Carinatum, (Pigeon Chest) A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Mil PRF 7024Document10 pagesMil PRF 7024kidseismicNo ratings yet
- 5 Star Hotel - REQUIREMENTS PDFDocument28 pages5 Star Hotel - REQUIREMENTS PDFAnbu SelviNo ratings yet
- Cervical Spine InjuryDocument8 pagesCervical Spine Injuryhesti06taniuchiNo ratings yet
- KGD - Pemicu 3: Ario Lukas - 405150072Document84 pagesKGD - Pemicu 3: Ario Lukas - 405150072ArioNo ratings yet
- Presentation Cervical SpineDocument48 pagesPresentation Cervical Spinekholoodrezeq8752No ratings yet
- Summary of Cervical Spine Injury GuidelinesDocument9 pagesSummary of Cervical Spine Injury GuidelinesAnonymous tN25joEXfLNo ratings yet
- Chapter 6: Spine and Spinal Cord Trauma ObjectivesDocument23 pagesChapter 6: Spine and Spinal Cord Trauma ObjectivesfadhillahilmayantiNo ratings yet
- C.1. 0Document8 pagesC.1. 0Bahna LucianNo ratings yet
- Boast 2 - Spinal ClearanceDocument1 pageBoast 2 - Spinal ClearanceSam BarnesNo ratings yet
- Mgmtof Spinal FracturesDocument2 pagesMgmtof Spinal FracturesrisnayektiNo ratings yet
- Spine and Spinal Cord InjuryDocument52 pagesSpine and Spinal Cord InjuryAdhi WiratmaNo ratings yet
- Society of Nuclear Medicine Procedure Guideline For Breast ScintigraphyDocument4 pagesSociety of Nuclear Medicine Procedure Guideline For Breast ScintigraphyLeticia PortilloNo ratings yet
- Kuliah Blok Neuroscience-SpineDocument27 pagesKuliah Blok Neuroscience-SpineCox AbeeNo ratings yet
- Oral and Maxillofacial Trauma - Fonseca - Primary ManagementDocument7 pagesOral and Maxillofacial Trauma - Fonseca - Primary ManagementyogeshNo ratings yet
- Practice Guidelines: Cervical Spine ClearanceDocument2 pagesPractice Guidelines: Cervical Spine ClearanceAnthony AlamNo ratings yet
- C Spine Clearance Ortho 3 Journal ClubDocument31 pagesC Spine Clearance Ortho 3 Journal ClubMuvenn KannanNo ratings yet
- Indication For Surgery and Spine ImmobilisationDocument2 pagesIndication For Surgery and Spine ImmobilisationMichael PrayogoNo ratings yet
- Lesson 4 - Spine InjuriesDocument8 pagesLesson 4 - Spine Injuriescarrenjoy1616No ratings yet
- Trauma To The Vertebral Column and Spinal CordDocument14 pagesTrauma To The Vertebral Column and Spinal CordБека ЭзугбаяNo ratings yet
- Cervical Tongs or Halo Ring: Application For Use in Cervical Traction (Assist)Document7 pagesCervical Tongs or Halo Ring: Application For Use in Cervical Traction (Assist)Hilary IgweNo ratings yet
- Exception Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical SpineDocument29 pagesException Include Burst # of Spine, Some Lateral Wedge # and Extension Injuries of Cervical Spinebhavesh jain100% (2)
- SCI and Spinal ShockDocument24 pagesSCI and Spinal Shockagus sukarnaNo ratings yet
- Trauma To The Vertebral Column and Spinal CordDocument14 pagesTrauma To The Vertebral Column and Spinal CordLory cNo ratings yet
- Trauma To The Vertebral Column and Spinal CordDocument14 pagesTrauma To The Vertebral Column and Spinal CordEdwardRazvanNo ratings yet
- Trauma To The Vertebral Column and Spinal CordDocument14 pagesTrauma To The Vertebral Column and Spinal CordSilviu MorteanuNo ratings yet
- Tuberculosis of SpineDocument19 pagesTuberculosis of SpinemelittaaNo ratings yet
- Myelography 1Document40 pagesMyelography 1Bikash SubediNo ratings yet
- Spinal Immobilization: By: Hatem AlsrourDocument16 pagesSpinal Immobilization: By: Hatem Alsrourhatem alsrour100% (2)
- Clearing The Cervical Spine: DR Claudia AY Cheng Senior Medical Officer Department of Anaesthesia and Intensive CareDocument78 pagesClearing The Cervical Spine: DR Claudia AY Cheng Senior Medical Officer Department of Anaesthesia and Intensive CareVictor ChanNo ratings yet
- Svoa Ne 02 020Document10 pagesSvoa Ne 02 020Trina ViskhawatNo ratings yet
- Cervical Spine Workshop: Chris Dillon, MD Regions Emergency Medicine Residency ProgramDocument89 pagesCervical Spine Workshop: Chris Dillon, MD Regions Emergency Medicine Residency ProgramAldi.SiregarNo ratings yet
- Airways in Neuro AxDocument8 pagesAirways in Neuro AxHarish BhatNo ratings yet
- Spinal Cord Injury Guide AssessmentDocument11 pagesSpinal Cord Injury Guide AssessmentKingsley Martinez CastroNo ratings yet
- Cervical Epidural Steroid Injection: DR A Sugeng Wibisono, Span, Fipm, FippDocument49 pagesCervical Epidural Steroid Injection: DR A Sugeng Wibisono, Span, Fipm, FippAndari SetianingtyasNo ratings yet
- Physical Examination of The Shoulder: Key WordsDocument10 pagesPhysical Examination of The Shoulder: Key WordsJavi LiraNo ratings yet
- SCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargDocument3 pagesSCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargnsatriotomoNo ratings yet
- Spine TraumaDocument96 pagesSpine TraumaSherlockHolmesSezNo ratings yet
- Treatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisDocument5 pagesTreatment of Neglegted Sternoclavicular (SC) Dislocation With Cannulated Screw and Cerclage Wire OsteosynthesisPeko PekoNo ratings yet
- Subaxial Cervical Spine Trauma: Cervical Injuries and Treatment (HJ Kim, Section Editor)Document9 pagesSubaxial Cervical Spine Trauma: Cervical Injuries and Treatment (HJ Kim, Section Editor)renonauvalNo ratings yet
- 1-s2.0-S0263931921000922-main-đã chuyển đổiDocument11 pages1-s2.0-S0263931921000922-main-đã chuyển đổiThế NguyễnNo ratings yet
- Injuries of The Spine2Document24 pagesInjuries of The Spine2cctmt5rpphNo ratings yet
- Principles of Critical Care MedicineDocument4 pagesPrinciples of Critical Care MedicineKarthik SNo ratings yet
- 10 1016@j Annemergmed 2018 03 033-2Document9 pages10 1016@j Annemergmed 2018 03 033-2Utami Dwi YusliNo ratings yet
- Thyroid Lobectomy and IsthmusectomyDocument12 pagesThyroid Lobectomy and IsthmusectomyAgustina100% (1)
- Neurosurgery PDFDocument8 pagesNeurosurgery PDFYuvraj ChauhanNo ratings yet
- BOAST GuidelinesDocument16 pagesBOAST GuidelinesSanju427No ratings yet
- Patient Preparations: Xial Mages OF THE ArynxDocument1 pagePatient Preparations: Xial Mages OF THE ArynxAli AlamsyahNo ratings yet
- Urethral Stricture Disease: Evaluation of The Male UrethraDocument5 pagesUrethral Stricture Disease: Evaluation of The Male UrethraCentanarianNo ratings yet
- PBC ClassifiDocument5 pagesPBC ClassifiParvathy R NairNo ratings yet
- Cervical Spine Clearance in Adult Trauma Patients.2Document5 pagesCervical Spine Clearance in Adult Trauma Patients.2Arun A MohanNo ratings yet
- 5-Level Spondylectomy For en Bloc Resection of Thoracic Chordoma: Case ReportDocument9 pages5-Level Spondylectomy For en Bloc Resection of Thoracic Chordoma: Case Reportholt linNo ratings yet
- Sem5 Protocol SCCDocument20 pagesSem5 Protocol SCCOlga Manco GuzmánNo ratings yet
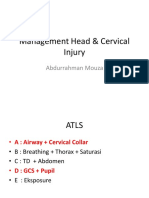
- Management Head & Cervical Injury: Abdurrahman MouzaDocument20 pagesManagement Head & Cervical Injury: Abdurrahman MouzaJohnNo ratings yet
- Paediatric RadiographyDocument75 pagesPaediatric RadiographyTapshi SohalNo ratings yet
- Tail Pull InjuryDocument10 pagesTail Pull InjuryClarissa NiciporciukasNo ratings yet
- Anesthesia For Cesarean Section in A Patient With AchondroplasiaDocument17 pagesAnesthesia For Cesarean Section in A Patient With AchondroplasiaFathin Amirah AminnuddinNo ratings yet
- Rangkuman ATLS 10 EditionDocument51 pagesRangkuman ATLS 10 EditionMalen SagaNo ratings yet
- Sci Acute ManagementDocument8 pagesSci Acute ManagementRyan Victor ManaloNo ratings yet
- 2020 To Applicant Handbook 1Document23 pages2020 To Applicant Handbook 1Marios GhobrialNo ratings yet
- 2020 Self AssessmentDocument4 pages2020 Self AssessmentMarios GhobrialNo ratings yet
- 2017 Article 528Document12 pages2017 Article 528Marios GhobrialNo ratings yet
- 290-TDPA-754 - Job Description & Person Specification - F3 - Locally Employed Doctor Programme Aug 22Document28 pages290-TDPA-754 - Job Description & Person Specification - F3 - Locally Employed Doctor Programme Aug 22Marios GhobrialNo ratings yet
- Oriel UserGuide Applicant V9Document48 pagesOriel UserGuide Applicant V9Marios GhobrialNo ratings yet
- Clinical Scenario 10 SummaryDocument1 pageClinical Scenario 10 SummaryMarios GhobrialNo ratings yet
- Queen's University Internal Medicine Simulation CourseDocument5 pagesQueen's University Internal Medicine Simulation CourseMarios GhobrialNo ratings yet
- P07-Fractures of The Pelvis and Acetabulum in Pediatric PatientsDocument46 pagesP07-Fractures of The Pelvis and Acetabulum in Pediatric PatientsMarios GhobrialNo ratings yet
- A Rather Yellow Looking LadyDocument6 pagesA Rather Yellow Looking LadyMarios GhobrialNo ratings yet
- Table 6-3 Management Overview of Traumatic Brain InjuryDocument1 pageTable 6-3 Management Overview of Traumatic Brain InjuryMarios GhobrialNo ratings yet
- Table 13-1 Rapid Triage and Transport GuidelinesDocument2 pagesTable 13-1 Rapid Triage and Transport GuidelinesMarios GhobrialNo ratings yet
- Simple ResumeDocument2 pagesSimple ResumeJessa AbadianoNo ratings yet
- Peter-Ji ResumeDocument13 pagesPeter-Ji Resumeapi-237132031No ratings yet
- Anna Liza R. Alfonso RN, RM, ManDocument13 pagesAnna Liza R. Alfonso RN, RM, ManAnnaAlfonsoNo ratings yet
- GSQMDocument48 pagesGSQMisolongNo ratings yet
- Enhancing Performance With Super StiffnessDocument4 pagesEnhancing Performance With Super Stiffnessval_ohalloran100% (1)
- Columbine Report Pgs 7901-8000Document100 pagesColumbine Report Pgs 7901-8000columbinefamilyrequest100% (1)
- Cplol, 2015Document4 pagesCplol, 2015nanuflorinaNo ratings yet
- Tooth Ankylosis: Clinical, Radiographic and HistologicalDocument9 pagesTooth Ankylosis: Clinical, Radiographic and HistologicalJuan Carlos MeloNo ratings yet
- Msds ManganDocument6 pagesMsds ManganLaely N AfidaNo ratings yet
- Palagiang Talaan Sa Mababang Paaralan: North Bay Boulevard North E/SDocument5 pagesPalagiang Talaan Sa Mababang Paaralan: North Bay Boulevard North E/SAnonymous 0TP7QfNo ratings yet
- NCP Myocardial InfarctionDocument1 pageNCP Myocardial InfarctionjamieboyRN88% (8)
- Root Cause Analysis Example Slurry Pump - FULLDocument11 pagesRoot Cause Analysis Example Slurry Pump - FULLTommyCasillas-GerenaNo ratings yet
- Scanning Electron Microscope (SEM) (The Analysis of Enamel Remineralization Increase in Pure Soy Milk (Glycine Max (L.) Merill) Immersion Using Scanning Electron Microscope (SEM) )Document5 pagesScanning Electron Microscope (SEM) (The Analysis of Enamel Remineralization Increase in Pure Soy Milk (Glycine Max (L.) Merill) Immersion Using Scanning Electron Microscope (SEM) )Sarah Ariefah SantriNo ratings yet
- PFEER GuidanceDocument56 pagesPFEER GuidanceKenmillicanNo ratings yet
- Four Handed Dentistry: An Indispensable Part For Efficient Clinical PracticeDocument6 pagesFour Handed Dentistry: An Indispensable Part For Efficient Clinical PracticeDevi NingrumNo ratings yet
- Identifying Assumptions and Conclusi Ons Test: SearchDocument3 pagesIdentifying Assumptions and Conclusi Ons Test: SearchLhena EstoestaNo ratings yet
- Tiqqun - 1999 - Machine-Men - User's GuideDocument15 pagesTiqqun - 1999 - Machine-Men - User's Guidesleslie100% (2)
- National Physician Fee Schedule Relative Value File Calendar Year 2016Document21 pagesNational Physician Fee Schedule Relative Value File Calendar Year 2016Budi KusumaNo ratings yet
- 33 Deeksheetha Prostho ATMPHDocument14 pages33 Deeksheetha Prostho ATMPHDhea FerraniNo ratings yet
- Group 2 Final DraftDocument19 pagesGroup 2 Final Draftapi-428300261No ratings yet
- INTELLICARE - DNC Available Dentists As of December 1, 2022Document38 pagesINTELLICARE - DNC Available Dentists As of December 1, 2022Mang InasalNo ratings yet
- Varnham - Seed Oil - Biological Properties, Health Benefits and Commercial Applications 2015Document178 pagesVarnham - Seed Oil - Biological Properties, Health Benefits and Commercial Applications 2015Cerasela BasaneteNo ratings yet
- ADEC HofT2ndEd Intro PDFDocument3 pagesADEC HofT2ndEd Intro PDFFranciscoNo ratings yet
- Treatment, Prevention and Control of Intestinal Parasitic InfectionDocument49 pagesTreatment, Prevention and Control of Intestinal Parasitic InfectiononilaNo ratings yet
- Research Paper of Deep Learning Based Frameworks by IIT GuwahatiDocument18 pagesResearch Paper of Deep Learning Based Frameworks by IIT GuwahatiPrasad SangameshwaranNo ratings yet
- Introduction To Prosthetic DentistryDocument28 pagesIntroduction To Prosthetic Dentistrysamar yousif mohamedNo ratings yet