Download as pdf or txt
You might also like
- Case 3 QuestionsDocument8 pagesCase 3 Questionsapi-532124328No ratings yet
- Case Study 3 MalnutritionDocument21 pagesCase Study 3 Malnutritionrohayatjohn100% (3)
- 1 s2.0 S0085253815560973 MainDocument12 pages1 s2.0 S0085253815560973 MainTri Veny AfreNo ratings yet
- NOT Duplicate: The Diabetic Foot Ulcer - Can Diet Make A Difference?Document3 pagesNOT Duplicate: The Diabetic Foot Ulcer - Can Diet Make A Difference?Vivi Evita DewiNo ratings yet
- Nutritional Support of Children in The Intensive Care Unit: ProfessorDocument24 pagesNutritional Support of Children in The Intensive Care Unit: ProfessorJuan Luis RuizNo ratings yet
- Nutrition Management in The Intensive Care UnitDocument17 pagesNutrition Management in The Intensive Care UnitIbnu ZakiNo ratings yet
- 2.2.3 MalnutritionDocument26 pages2.2.3 MalnutritionMichael JuliusNo ratings yet
- Nutritional Support in ICU PatientsDocument24 pagesNutritional Support in ICU PatientsRisma Abdul WarisNo ratings yet
- Nutritionalproblems Affectingolderadults: Neva L. CroganDocument13 pagesNutritionalproblems Affectingolderadults: Neva L. CroganALBERTO LUIS LIZCANO GONZALEZ ESTUDIANTENo ratings yet
- Persistent Diarrhea With Severe Malnutrition Type MarasmusDocument47 pagesPersistent Diarrhea With Severe Malnutrition Type MarasmusAkash KhannaNo ratings yet
- Protein Energy Wasting What Is It and What Can We Do To Prevent ItDocument8 pagesProtein Energy Wasting What Is It and What Can We Do To Prevent ItLú VillalobosNo ratings yet
- Novel Insights On Nutrient Management of Sarcopenia in ElderlyDocument15 pagesNovel Insights On Nutrient Management of Sarcopenia in ElderlyMario Ociel MoyaNo ratings yet
- Clinical NutritionDocument9 pagesClinical NutritionAnnisa NoviliaNo ratings yet
- Malnutrition: Practice EssentialsDocument13 pagesMalnutrition: Practice EssentialsIda WilonaNo ratings yet
- Moore Et Al-2018-Clinical Liver DiseaseDocument4 pagesMoore Et Al-2018-Clinical Liver DiseaseCarlos Francisco Enciso MartinezNo ratings yet
- MLS 111B Endterm LectureDocument41 pagesMLS 111B Endterm LectureJohanna MarieNo ratings yet
- 13 SureDocument11 pages13 SureSamuel Kyei-BoatengNo ratings yet
- Nutrition in The Critically Ill PatientDocument13 pagesNutrition in The Critically Ill PatientnainazahraNo ratings yet
- Nutritional Support of Children With Chronic LiverDocument5 pagesNutritional Support of Children With Chronic LiverVianNo ratings yet
- Article Review Nutrition in Critically Ill ChildDocument6 pagesArticle Review Nutrition in Critically Ill ChildkhairachungNo ratings yet
- NUTRITIONAL NEEDS OF CRITICALLY ILL CHILD SanthoshDocument21 pagesNUTRITIONAL NEEDS OF CRITICALLY ILL CHILD SanthoshSanthosh.S.U100% (1)
- Protein-Calories, Malnutrition & Nutritional DeficienciesDocument14 pagesProtein-Calories, Malnutrition & Nutritional DeficienciesChino Paolo SamsonNo ratings yet
- Nutricion PerioperatoriaDocument11 pagesNutricion PerioperatoriaAndres Neira QuezadaNo ratings yet
- Jcp0617review StefanacciDocument6 pagesJcp0617review StefanacciIzlam Ing TyazNo ratings yet
- Nutrients: Nutrition in Sepsis: A Bench-to-Bedside ReviewDocument16 pagesNutrients: Nutrition in Sepsis: A Bench-to-Bedside ReviewAdiel OjedaNo ratings yet
- Critical Ill PDFDocument5 pagesCritical Ill PDFAnish H DaveNo ratings yet
- Protein-Calories, Malnutrition & Nutritional DeficienciesDocument15 pagesProtein-Calories, Malnutrition & Nutritional DeficienciesChino Paolo SamsonNo ratings yet
- PIIS0085253815550461Document10 pagesPIIS0085253815550461KatNo ratings yet
- Latest Consensus and Update On Protein Energy-Wasting - 2015Document19 pagesLatest Consensus and Update On Protein Energy-Wasting - 2015Lú VillalobosNo ratings yet
- Handout 1 Intro 2018Document57 pagesHandout 1 Intro 2018Cezhille BattadNo ratings yet
- PDF Philippine-CONSENSUS-STATEMENT-FINAL-BJMeditsDocument21 pagesPDF Philippine-CONSENSUS-STATEMENT-FINAL-BJMeditsElly JoyNo ratings yet
- All About Anorexia in The Elderly: Czeresna H. SoejonoDocument5 pagesAll About Anorexia in The Elderly: Czeresna H. SoejonoJalu PanjongkoNo ratings yet
- Nutritional Assessment and Management in Paediatric ChronicDocument7 pagesNutritional Assessment and Management in Paediatric ChronicmpcponceNo ratings yet
- Ismail 2021Document11 pagesIsmail 2021neeraj bishtNo ratings yet
- Jurnal Nutrisi 4Document16 pagesJurnal Nutrisi 4agung suprasthaNo ratings yet
- Artigo 4 Kasti interrupção da TNE 2023Document14 pagesArtigo 4 Kasti interrupção da TNE 2023SuzaneNo ratings yet
- Nelson's Hour - 58-60Document51 pagesNelson's Hour - 58-60Josselle Sempio CalientaNo ratings yet
- 2014 The Science and Practice of Micronutrient Supplementations in Nutritional Anemia - An Evidence-Based ReviewDocument17 pages2014 The Science and Practice of Micronutrient Supplementations in Nutritional Anemia - An Evidence-Based ReviewMario Ivan De la Cruz LaraNo ratings yet
- Nutrition in Critical CareDocument6 pagesNutrition in Critical CareSusanita RamirezNo ratings yet
- AED 2020-Gruidebook For Nutritionat Treatment of Eating DisordersDocument63 pagesAED 2020-Gruidebook For Nutritionat Treatment of Eating DisordersNaiaraNo ratings yet
- Rees-Shaw2007 Article NutritionInChildrenWithCRFAndODocument14 pagesRees-Shaw2007 Article NutritionInChildrenWithCRFAndOannur printNo ratings yet
- Clinical Nutrition Volume 67 Issue 2013 Bell Nutritional Management of Children With Cerebral PalsyDocument4 pagesClinical Nutrition Volume 67 Issue 2013 Bell Nutritional Management of Children With Cerebral PalsyCamila FigueroaNo ratings yet
- Dieta Na Causa e No Manejo Do SII 2014Document11 pagesDieta Na Causa e No Manejo Do SII 2014Priscilla Ferreira Crespo GutierrezNo ratings yet
- Journal of Diabetes - 2022 - Ratiner - Time Limited Diets and The Gut Microbiota in Cardiometabolic DiseaseDocument17 pagesJournal of Diabetes - 2022 - Ratiner - Time Limited Diets and The Gut Microbiota in Cardiometabolic DiseaseRenė RuizNo ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos SurDocument8 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos SurJewel Ramos GalinatoNo ratings yet
- Cachexia and Protein-Energy Wasting in Children With Chronic Kidney DiseaseDocument9 pagesCachexia and Protein-Energy Wasting in Children With Chronic Kidney Diseaseratna ardianaNo ratings yet
- Nutritional Management in The Intensive Care Unit: Inderpaul S Sehgal, Navneet SinghDocument19 pagesNutritional Management in The Intensive Care Unit: Inderpaul S Sehgal, Navneet SinghRida MehmoodNo ratings yet
- Parenteral Nutrition in Infants and ChildrenDocument47 pagesParenteral Nutrition in Infants and Childrenj.escobarNo ratings yet
- EssayDocument16 pagesEssayLorenz Sagayaga ListaNo ratings yet
- Nutrition in Critically Ill PatientDocument10 pagesNutrition in Critically Ill PatientMiras PtNo ratings yet
- Nutritional Support of The Critically Ill Small AnDocument12 pagesNutritional Support of The Critically Ill Small AnTactvisNo ratings yet
- Set-Point Theory and ObesityDocument6 pagesSet-Point Theory and ObesityDouglas MarinNo ratings yet
- Review Article: Hormonal Regulators of AppetiteDocument9 pagesReview Article: Hormonal Regulators of AppetiteREKSNo ratings yet
- JMedNutrNutraceut2277-5417572 150255Document7 pagesJMedNutrNutraceut2277-5417572 150255jufranNo ratings yet
- Ketogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4Document21 pagesKetogenic Diet IF-Philippine Lipid Society Consensus-Statement-20191108v4donmd98No ratings yet
- 1 s2.0 S1043661823001366 MainDocument12 pages1 s2.0 S1043661823001366 MainBBD BBDNo ratings yet
- Gille2010 Article OverviewOfThePhysiologicalChanDocument10 pagesGille2010 Article OverviewOfThePhysiologicalChanramzan aliNo ratings yet
- Malnutrition in the ElderlyFrom EverandMalnutrition in the ElderlyW.O. SeilerNo ratings yet
- Obesity - Short Scientific Findings to Ameliorate the Body WeightFrom EverandObesity - Short Scientific Findings to Ameliorate the Body WeightNo ratings yet
- Anatomically Corrected Malposition of Great Arteries - (I, L, D) Type: First ContactDocument2 pagesAnatomically Corrected Malposition of Great Arteries - (I, L, D) Type: First ContactanhiramdhaniNo ratings yet
- Hypokalemic Periodic Paralysis PDFDocument2 pagesHypokalemic Periodic Paralysis PDFanhiramdhaniNo ratings yet
- E773 FullDocument6 pagesE773 FullanhiramdhaniNo ratings yet
- Interleukin-17 and Its Expanding Biological Functions: ReviewDocument11 pagesInterleukin-17 and Its Expanding Biological Functions: ReviewanhiramdhaniNo ratings yet
- Pediatric Critical Care and COVID19: Pre-Publication ReleaseDocument14 pagesPediatric Critical Care and COVID19: Pre-Publication ReleaseanhiramdhaniNo ratings yet
- Nutritional Status Characteristics of Infants Presenting With Neonatal CholestasisDocument5 pagesNutritional Status Characteristics of Infants Presenting With Neonatal CholestasisanhiramdhaniNo ratings yet
- Education PracticeDocument5 pagesEducation PracticeanhiramdhaniNo ratings yet
- Soymilk As Source of Nutrient For Malnourished Population of Developing Country: A ReviewDocument13 pagesSoymilk As Source of Nutrient For Malnourished Population of Developing Country: A ReviewanhiramdhaniNo ratings yet
- NIH Public Access: Author ManuscriptDocument13 pagesNIH Public Access: Author ManuscriptanhiramdhaniNo ratings yet
- 1 s2.0 S1875957218302754 MainDocument8 pages1 s2.0 S1875957218302754 MainanhiramdhaniNo ratings yet
- NIH Public Access: "Complementary and Alternative Medicine Treatments ForDocument15 pagesNIH Public Access: "Complementary and Alternative Medicine Treatments ForanhiramdhaniNo ratings yet
- Clinical Characteristics of 19 Neonates Born To Mothers With COVID-19Document6 pagesClinical Characteristics of 19 Neonates Born To Mothers With COVID-19anhiramdhaniNo ratings yet
- Patients With Juvenile Psoriatic Arthritis Comprise Two Distinct PopulationsDocument9 pagesPatients With Juvenile Psoriatic Arthritis Comprise Two Distinct PopulationsanhiramdhaniNo ratings yet
- Classroom Interventions For Attention Deficit/Hyperactivity DisorderDocument10 pagesClassroom Interventions For Attention Deficit/Hyperactivity DisorderanhiramdhaniNo ratings yet
- COVID-19 and Neonatal Resuscitation: Editorial NoteDocument1 pageCOVID-19 and Neonatal Resuscitation: Editorial NoteanhiramdhaniNo ratings yet
- 388Document6 pages388anhiramdhaniNo ratings yet
- Article 2194Document9 pagesArticle 2194anhiramdhani100% (1)
- Growth and Nutrition in Pediatric Chronic Kidney Disease: Douglas M. SilversteinDocument10 pagesGrowth and Nutrition in Pediatric Chronic Kidney Disease: Douglas M. SilversteinanhiramdhaniNo ratings yet
- Panel Punch Points Report-06!08!2019Document165 pagesPanel Punch Points Report-06!08!2019Kamesh MarwadeNo ratings yet
- LatexDocument27 pagesLatexYuxdar ContellNo ratings yet
- Paper Chromatography: A Review: Mukta Gupta, Bhupinder Kapoor, Reena GuptaDocument8 pagesPaper Chromatography: A Review: Mukta Gupta, Bhupinder Kapoor, Reena GuptaYonas AlexandryNo ratings yet
- Javi ProgrammingDocument8 pagesJavi ProgrammingJoseNo ratings yet
- Seminar Report On Power Quality MonitoringDocument23 pagesSeminar Report On Power Quality MonitoringBhaargava Rama kodumuriNo ratings yet
- Raoult's LawDocument8 pagesRaoult's LawHARSH DHOLAKIYANo ratings yet
- Theory - Module 3Document11 pagesTheory - Module 3Darish TrinidadNo ratings yet
- Chemistry PG 2015 Admn On05sept2015Document96 pagesChemistry PG 2015 Admn On05sept2015ZiyadNo ratings yet
- Object-Relational Features in Oracle Database!: View of The Database World!Document14 pagesObject-Relational Features in Oracle Database!: View of The Database World!جيم جيمNo ratings yet
- Product Data Sheet Powernics 9701 Black Lead Free: Berger Nippon Paint Automotive Coatings Private LimitedDocument2 pagesProduct Data Sheet Powernics 9701 Black Lead Free: Berger Nippon Paint Automotive Coatings Private LimitedSamNo ratings yet
- Creating Hello World Web Widget With HTML CSS and JavascriptDocument10 pagesCreating Hello World Web Widget With HTML CSS and Javascriptrajeshlal100% (1)
- Emergency Lights Central Battery System Testing and Commissioning Method of StatementDocument12 pagesEmergency Lights Central Battery System Testing and Commissioning Method of StatementAleen Gamal Al-DinjiNo ratings yet
- HP Laser 103a PrinterDocument2 pagesHP Laser 103a PrinterIsaac Musiwa BandaNo ratings yet
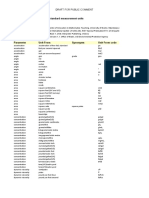
- Multipliers Used To Convert To Standard Measurement Units ReferencesDocument18 pagesMultipliers Used To Convert To Standard Measurement Units Referencesira huttNo ratings yet
- Engineering Economic: Bhesh R Kanel, CoordinatorDocument21 pagesEngineering Economic: Bhesh R Kanel, Coordinatorharry potterNo ratings yet
- ISOMARDocument5 pagesISOMARscribd405No ratings yet
- (Fracturing of Dormansi and Viability of Sugar Palm Seed (Arenga Pinnata Merr) On Various Media Plant and Physical Treatment)Document8 pages(Fracturing of Dormansi and Viability of Sugar Palm Seed (Arenga Pinnata Merr) On Various Media Plant and Physical Treatment)Cintami FatmarayaNo ratings yet
- Chapter9 Mathlinks8 UnitplanDocument10 pagesChapter9 Mathlinks8 Unitplanapi-271785617No ratings yet
- SIEMENS S7-1500 Power Module Ps 60w 24-48-60vdc Manual en US en-USDocument28 pagesSIEMENS S7-1500 Power Module Ps 60w 24-48-60vdc Manual en US en-USl1f3b00kNo ratings yet
- BS en 00059-2016Document14 pagesBS en 00059-2016anurag yadavNo ratings yet
- Unit-4 Blood Pressure Measurement: M F Pimentel August 26, 2019 Blood Pressure - Biomedical Signal ProcessingDocument59 pagesUnit-4 Blood Pressure Measurement: M F Pimentel August 26, 2019 Blood Pressure - Biomedical Signal Processingpriya dharshiniNo ratings yet
- VMC - SOSE JEE MAINS - 4 (Question Paper)Document14 pagesVMC - SOSE JEE MAINS - 4 (Question Paper)Gunjan SinghNo ratings yet
- Thales TheoremDocument3 pagesThales Theoremgitongajohn253No ratings yet
- ButterflyMX - Elevator Control Wiring DiagramDocument1 pageButterflyMX - Elevator Control Wiring DiagramSyed iliyasNo ratings yet
- Lecture24 25 SubnettingDocument46 pagesLecture24 25 SubnettingFiroz kumar100% (2)
- Project NoteDocument37 pagesProject NoteHimel HossainNo ratings yet
- Bc4157 Course ProfileDocument5 pagesBc4157 Course ProfileMan HongNo ratings yet
- English Premier League: DatasetDocument1 pageEnglish Premier League: DatasetDilshadNo ratings yet
- CH 1 Part 2 Add ProblemsDocument2 pagesCH 1 Part 2 Add Problemstarek ahmedNo ratings yet
- Monthly Test (April) - Igcse Maths: Marks %Document6 pagesMonthly Test (April) - Igcse Maths: Marks %Aqilah AbdullahNo ratings yet