Download as pdf or txt
You might also like
- Normas NES M1019Document12 pagesNormas NES M1019Margarita Torres FloresNo ratings yet
- NUTR - 150 - Final - Dietary - Analysis - 2-Day - NutritionCalc Plus Final-1Document12 pagesNUTR - 150 - Final - Dietary - Analysis - 2-Day - NutritionCalc Plus Final-1Benjamín EcharryNo ratings yet
- Hypertension and Cardiovascular Disease - Nutritional Case StudyDocument9 pagesHypertension and Cardiovascular Disease - Nutritional Case StudySociedad AlumnosNo ratings yet
- PES Statement Exercise Practice Activity 1Document1 pagePES Statement Exercise Practice Activity 1FalguniNo ratings yet
- Case Study Adime NoteDocument2 pagesCase Study Adime Noteapi-240616135No ratings yet
- Case Study 30Document6 pagesCase Study 30api-276551783No ratings yet
- Adime NoteDocument2 pagesAdime Noteapi-384503305100% (1)
- Metabolic Stress Case StudyDocument10 pagesMetabolic Stress Case StudydakotaNo ratings yet
- Nutrition 401 ReflectionDocument1 pageNutrition 401 Reflectionapi-339569858No ratings yet
- Nutrition Diagnosis Etiology Matrix PDFDocument16 pagesNutrition Diagnosis Etiology Matrix PDFLaura BrownNo ratings yet
- Richard Goldman Case StudyDocument8 pagesRichard Goldman Case Studyapi-484960148No ratings yet
- Bullying, Stalking and ExtortionDocument17 pagesBullying, Stalking and ExtortionJLafge83% (6)
- The Soul of An Octopus - Favorite QuotesDocument7 pagesThe Soul of An Octopus - Favorite QuotesTanya RodmanNo ratings yet
- Lab2 PDFDocument3 pagesLab2 PDFMd.Arifur RahmanNo ratings yet
- Gout: What To Eat/What Not To EatDocument3 pagesGout: What To Eat/What Not To EatazharsaleemkhanNo ratings yet
- Case Study 3Document10 pagesCase Study 3api-271185611No ratings yet
- ESPEN Guidelines On Parenteral Nutrition. Intensive Care 2009Document38 pagesESPEN Guidelines On Parenteral Nutrition. Intensive Care 2009ERINSONNo ratings yet
- Functional Foods: Presented by Nupur Agarwal Amity Institute of Food Technology, NoidaDocument9 pagesFunctional Foods: Presented by Nupur Agarwal Amity Institute of Food Technology, NoidaNupur AgarwalNo ratings yet
- Medicine and Nutrition Case StudyDocument5 pagesMedicine and Nutrition Case Studyapi-384113918No ratings yet
- Nutrition Care Process WorksheetDocument7 pagesNutrition Care Process Worksheetapi-338119904No ratings yet
- A S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildDocument56 pagesA S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildPaulina Kristiani BangunNo ratings yet
- Medical Nutrition Therapy For Renal Disease 2021Document39 pagesMedical Nutrition Therapy For Renal Disease 2021Oktaviani Karo SekaliNo ratings yet
- fshn420 - Cancer Case StudiesDocument5 pagesfshn420 - Cancer Case Studiesapi-703153445No ratings yet
- CVD HTN Case Study AssignmentDocument7 pagesCVD HTN Case Study Assignmentapi-353723892No ratings yet
- MNT 1 DM Case Study Due 11 29 2016Document3 pagesMNT 1 DM Case Study Due 11 29 2016api-340581896No ratings yet
- Nutritional Issues in The ICU Case FileDocument2 pagesNutritional Issues in The ICU Case Filehttps://medical-phd.blogspot.com100% (1)
- Cole Kelby Nutrition Database Form 042018 4Document11 pagesCole Kelby Nutrition Database Form 042018 4api-381003133100% (1)
- Type 2 Diabetes Mellitus Case StudyDocument9 pagesType 2 Diabetes Mellitus Case StudyMike CoolNo ratings yet
- Nutri LEC AssignmentDocument3 pagesNutri LEC AssignmentJohnNo ratings yet
- Case Study 2 2018Document6 pagesCase Study 2 2018jigsawNo ratings yet
- Final MNT Ostomy 1Document11 pagesFinal MNT Ostomy 1api-366154535100% (1)
- MNT pt1Document5 pagesMNT pt1api-339312954No ratings yet
- Bs NCPDocument10 pagesBs NCPapi-340851914No ratings yet
- Adime Note 1 415b 2Document3 pagesAdime Note 1 415b 2api-287399108No ratings yet
- DigestiveDocument18 pagesDigestivekimberlynNo ratings yet
- Lesson 2 - Principles of Nutrition TherapyDocument15 pagesLesson 2 - Principles of Nutrition TherapyJoddie LoplopNo ratings yet
- NA NME TerminologyDocument3 pagesNA NME TerminologyVha AmalaNo ratings yet
- NCM 105 Lec: Nutriton and Diet Therapy Project On Therapeutic DietsDocument15 pagesNCM 105 Lec: Nutriton and Diet Therapy Project On Therapeutic DietsVinz OñoNo ratings yet
- TPN Protocol HandoutDocument2 pagesTPN Protocol Handoutapi-610233914No ratings yet
- Hypocaloric Enteral NutritionDocument10 pagesHypocaloric Enteral NutritionMario TGNo ratings yet
- Approach To Managing Increased Risk For Cardiovascular Disease in Patients With Severe Mental Illness - UpToDateDocument18 pagesApproach To Managing Increased Risk For Cardiovascular Disease in Patients With Severe Mental Illness - UpToDateBillis ParaschouNo ratings yet
- Sample Case StudyDocument10 pagesSample Case Studyapi-702059884No ratings yet
- Human Nutrition QuizDocument6 pagesHuman Nutrition QuizMattMattTv JapanNo ratings yet
- Healthy Vegetarian Part 1Document2 pagesHealthy Vegetarian Part 1Frank BradshawNo ratings yet
- Community Nutrition Intervention PDFDocument2 pagesCommunity Nutrition Intervention PDFBarbara100% (1)
- NCPT For EALDocument61 pagesNCPT For EALAsri SubarjatiNo ratings yet
- Nutrition Therapy For Cardiovascular DisordersDocument10 pagesNutrition Therapy For Cardiovascular DisorderspeytonNo ratings yet
- Medical Nutrition TherapyDocument4 pagesMedical Nutrition TherapycjgregoryNo ratings yet
- Nutrition Support Case StudyDocument6 pagesNutrition Support Case StudydakotaNo ratings yet
- Adime For Ic1Document3 pagesAdime For Ic1api-368616568No ratings yet
- ESPEN - Guideline On Clinical Nutrition in The Intensive Care Unit PDFDocument32 pagesESPEN - Guideline On Clinical Nutrition in The Intensive Care Unit PDFМаксим ДорошкевичNo ratings yet
- Diet For CancerDocument28 pagesDiet For CancerCherlotte TbNo ratings yet
- Obesity and Iron Metabolism PDFDocument6 pagesObesity and Iron Metabolism PDFAhmed SobhNo ratings yet
- Nutri-Quiz ReviewerDocument2 pagesNutri-Quiz ReviewerCrystal Ann Monsale TadiamonNo ratings yet
- Case Study FinalDocument2 pagesCase Study Finalapi-307578607No ratings yet
- Neutropenic DietDocument6 pagesNeutropenic DietJohn Bryan JamisonNo ratings yet
- 08 - Indications, Contraindications, Complications and Monitoring of enDocument13 pages08 - Indications, Contraindications, Complications and Monitoring of enbocah_britpopNo ratings yet
- PDF Nutrition CM 1 CU 1 LEC WEEK 1Document27 pagesPDF Nutrition CM 1 CU 1 LEC WEEK 1Zharm MayNo ratings yet
- Medical Nutrition Therapy For Diseases of The MusculoskeletalDocument55 pagesMedical Nutrition Therapy For Diseases of The MusculoskeletalSie ningsih100% (1)
- Adult Module 3 - Increasing Fruits and Vegetable Intake Powerpoint (English) PDFDocument25 pagesAdult Module 3 - Increasing Fruits and Vegetable Intake Powerpoint (English) PDFKennedy FadriquelanNo ratings yet
- Guidelines for Measuring Household and Individual Dietary DiversityFrom EverandGuidelines for Measuring Household and Individual Dietary DiversityNo ratings yet
- Mediterranean Diet Cookbook for Beginners: Unlock the Health Benefits of the Mediterranean Diet with Easy and Delicious Recipes for Everyday Eating!From EverandMediterranean Diet Cookbook for Beginners: Unlock the Health Benefits of the Mediterranean Diet with Easy and Delicious Recipes for Everyday Eating!No ratings yet
- IPD Rolando AtaDocument2 pagesIPD Rolando AtaMarcela RamosNo ratings yet
- Emu LinesDocument22 pagesEmu LinesRahul MehraNo ratings yet
- Environmental Protection: "We Never Know The Worth of Water Till The Wellis Dry."Document14 pagesEnvironmental Protection: "We Never Know The Worth of Water Till The Wellis Dry."Mary Jane BuaronNo ratings yet
- Academic Calendar Fall 19-Spring 20 & Summer 20-Final-1 PDFDocument3 pagesAcademic Calendar Fall 19-Spring 20 & Summer 20-Final-1 PDFAhmadNo ratings yet
- Clinical Emergency Management Program: Advanced WorkshopDocument4 pagesClinical Emergency Management Program: Advanced WorkshopNataraj ThambiNo ratings yet
- Practical Research 2: Sampling and Probability SamplingDocument11 pagesPractical Research 2: Sampling and Probability SamplingJohn Joseph JalandoniNo ratings yet
- Grade 5 CommentsDocument17 pagesGrade 5 Commentsreza anggaNo ratings yet
- Pioneer Car Video AVD-W6210Document50 pagesPioneer Car Video AVD-W6210calinp72No ratings yet
- APPLICATION FOR REGISTRATION/ACCREDITATION AS AN ECOZONE SERVICE ENTERPRISE (For Customs Broker, Freight Forwarder/Trucker and Security Agency)Document7 pagesAPPLICATION FOR REGISTRATION/ACCREDITATION AS AN ECOZONE SERVICE ENTERPRISE (For Customs Broker, Freight Forwarder/Trucker and Security Agency)Albert YsegNo ratings yet
- Babst Vs CA PDFDocument17 pagesBabst Vs CA PDFJustin YañezNo ratings yet
- Greece Education Foundation Courses and Gces 10 2010Document6 pagesGreece Education Foundation Courses and Gces 10 2010Stamatios KarapournosNo ratings yet
- Phd:304 Lab Report Advanced Mathematical Physics: Sachin Singh Rawat 16PH-06 (Department of Physics)Document12 pagesPhd:304 Lab Report Advanced Mathematical Physics: Sachin Singh Rawat 16PH-06 (Department of Physics)sachin rawatNo ratings yet
- Artificial Intelligence and Patent LawDocument4 pagesArtificial Intelligence and Patent LawSaksham TyagiNo ratings yet
- Belgian Carrier PigeonDocument145 pagesBelgian Carrier PigeonstepathcNo ratings yet
- SB KarbonDocument3 pagesSB KarbonAbdul KarimNo ratings yet
- Rat ModelDocument1 pageRat Modelapi-483276188No ratings yet
- Minimal Stimulation IVF Vs Conventional IVFDocument8 pagesMinimal Stimulation IVF Vs Conventional IVFpolygoneNo ratings yet
- Trial in AbsentiaDocument12 pagesTrial in AbsentiaNahid hossainNo ratings yet
- Agustin Vs Edu - DigestDocument2 pagesAgustin Vs Edu - Digestcmv mendozaNo ratings yet
- LEARNING THEORIES Ausubel's Learning TheoryDocument17 pagesLEARNING THEORIES Ausubel's Learning TheoryCleoNo ratings yet
- Government of Karnataka: Only For Birth Verification PurposeDocument1 pageGovernment of Karnataka: Only For Birth Verification PurposeAmit VantagodiNo ratings yet
- RecipesDocument7 pagesRecipesIndira UmareddyNo ratings yet
- Diagnostic Exam 2Document5 pagesDiagnostic Exam 2Tomzki Cornelio50% (2)
- Iii Iihiiiiiiiiiiii 111111: Does User-Oriented Gas Turbine Research Pay Off?Document7 pagesIii Iihiiiiiiiiiiii 111111: Does User-Oriented Gas Turbine Research Pay Off?Morteza YazdizadehNo ratings yet
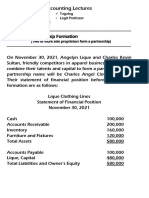
- 8 Lec 03 - Partnership Formation With BusinessDocument2 pages8 Lec 03 - Partnership Formation With BusinessNathalie GetinoNo ratings yet
- Company Feasibility StudyDocument21 pagesCompany Feasibility StudyDesiree Raot RaotNo ratings yet