Download as pdf or txt
You might also like
- Hinman Atlas of Urologic Surgery 2ndDocument1,189 pagesHinman Atlas of Urologic Surgery 2ndScott Caesar100% (12)
- Coronary Artery Bypass Graph Concept MapDocument5 pagesCoronary Artery Bypass Graph Concept Mapnursing concept maps100% (1)
- CCRN-PCCN-CMC Review Cardiac Part 2Document21 pagesCCRN-PCCN-CMC Review Cardiac Part 2Giovanni Mictil100% (1)
- Heart FailureDocument16 pagesHeart FailureLogadarshini VeerasamyNo ratings yet
- Penatalaksanaan Penyulit Gagal JantungDocument17 pagesPenatalaksanaan Penyulit Gagal JantungarumNo ratings yet
- Cme HFDocument30 pagesCme HFTze SiangNo ratings yet
- HF PresentationDocument62 pagesHF Presentationapi-552486649No ratings yet
- 9 - Role of Non InvasiveDocument46 pages9 - Role of Non InvasiveHavara Kausar AkbarNo ratings yet
- Episode 163 Acute Heart Failure Part 1Document8 pagesEpisode 163 Acute Heart Failure Part 1Dk YadavNo ratings yet
- Monitoring PerioperatipDocument54 pagesMonitoring Perioperatipjavajavu100% (1)
- Lecture 12 Cardio Intensive CasesDocument32 pagesLecture 12 Cardio Intensive Casesraul0% (1)
- Post Op Care PH Yogya-Ok - SipDocument29 pagesPost Op Care PH Yogya-Ok - SipTaufik KurniawanNo ratings yet
- Acute HF-IAIDocument49 pagesAcute HF-IAIAndita ListyannisaNo ratings yet
- Chronic Heart FailureDocument25 pagesChronic Heart FailureNeilavery WindaNo ratings yet
- Kuliah Pakar HF FKUMMDocument46 pagesKuliah Pakar HF FKUMMOkta Dwi Kusuma AyuNo ratings yet
- Dr.M.Kannan MD DA Professor and HOD of Anaesthesiology Tirunelveli Medical CollegeDocument26 pagesDr.M.Kannan MD DA Professor and HOD of Anaesthesiology Tirunelveli Medical CollegeAlina CiubotariuNo ratings yet
- Review of Advancements in Heart Failure 81220Document65 pagesReview of Advancements in Heart Failure 81220Dr MustafaNo ratings yet
- How To Deal With Acute Dyspneu in ER: Acute Heart Failure OR Pulmonary Problem?Document36 pagesHow To Deal With Acute Dyspneu in ER: Acute Heart Failure OR Pulmonary Problem?tyasNo ratings yet
- Complete Cardiology Revision Part 3 - B107b8e3 0692 4e9c 80a0 90c4dbd98754Document59 pagesComplete Cardiology Revision Part 3 - B107b8e3 0692 4e9c 80a0 90c4dbd98754KumarNo ratings yet
- Hypertensive Urgency: PGI Jorge John III P. QuilalaDocument32 pagesHypertensive Urgency: PGI Jorge John III P. QuilalaJerome GeronimoNo ratings yet
- Heart FailureDocument49 pagesHeart FailureJabraan Jamil100% (1)
- Medicine High YieldDocument213 pagesMedicine High Yield5jqr2r7z2hNo ratings yet
- Chronic Heart Failure: I. Brief Definition Iv. Disease ProcessDocument12 pagesChronic Heart Failure: I. Brief Definition Iv. Disease ProcessJennifer BeguinwaNo ratings yet
- Ehw128 AddendaDocument6 pagesEhw128 AddendaClement ThansNo ratings yet
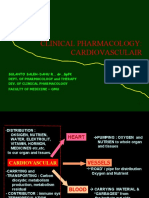
- Cardiovasc Farmakologi Klinik0908Document49 pagesCardiovasc Farmakologi Klinik0908deka saputraNo ratings yet
- PUD KeymessageDocument13 pagesPUD Keymessagenando baehaNo ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- Post COVID ManagementDocument4 pagesPost COVID ManagementReddy VaniNo ratings yet
- Updated PE and FESDocument35 pagesUpdated PE and FESNg AliceNo ratings yet
- Hypertension HHZ Oct20Document58 pagesHypertension HHZ Oct20m.najmi29No ratings yet
- HypertensionDocument35 pagesHypertensionMuhammad ZubairNo ratings yet
- Heart Failure & Cardiac Arrest: Rony YuliwansyahDocument92 pagesHeart Failure & Cardiac Arrest: Rony YuliwansyahSasha ManoNo ratings yet
- NYHA Class IV HFrEF With Hypertension - 06 Feb 2023Document28 pagesNYHA Class IV HFrEF With Hypertension - 06 Feb 2023Pragnesh ShahNo ratings yet
- HeartFailure Nursing FIK 2014Document101 pagesHeartFailure Nursing FIK 2014Putri NurlaeliNo ratings yet
- Heart Failure 1aDocument54 pagesHeart Failure 1aFredericka QuayeNo ratings yet
- Incidence Pathophysiology Classification Causes Diagnosis Assessing Cardiovascular Disability Treatment MessagesDocument67 pagesIncidence Pathophysiology Classification Causes Diagnosis Assessing Cardiovascular Disability Treatment MessagesAhmed ElshewiNo ratings yet
- Hipertensi - SMT 6 2017 - 1Document101 pagesHipertensi - SMT 6 2017 - 1yussikafernandaNo ratings yet
- PSMA411 Clinical Pharmacy and Pharmacotherapeutics (Part 1)Document104 pagesPSMA411 Clinical Pharmacy and Pharmacotherapeutics (Part 1)Aubrey MadelaineNo ratings yet
- Lecture 3Document54 pagesLecture 3HazaNo ratings yet
- Diagnosis Dan Tatalaksana Gagal Jantung - 2Document30 pagesDiagnosis Dan Tatalaksana Gagal Jantung - 2Rumah Sunat TasikNo ratings yet
- Heart Failure 5ADocument86 pagesHeart Failure 5AK Praful KumarNo ratings yet
- Syncope: DR - Boyke Marthin Simbolon, Mked (An), SpanDocument18 pagesSyncope: DR - Boyke Marthin Simbolon, Mked (An), SpanMiftahThariqNo ratings yet
- Pulmonary HTN Topic DiscussionDocument2 pagesPulmonary HTN Topic Discussionapi-648401824No ratings yet
- Autonomic Neuropathy DMDocument49 pagesAutonomic Neuropathy DMJaskaran SinghNo ratings yet
- Sabina Week 3 STEMI Case Study 4Document11 pagesSabina Week 3 STEMI Case Study 4sapanjeet kourNo ratings yet
- IM CASE RTR - Myocardial InfarctionDocument47 pagesIM CASE RTR - Myocardial InfarctionTrisNo ratings yet
- Innovation in Clinical Care in Heart FailureDocument107 pagesInnovation in Clinical Care in Heart FailureSebastian Henao ErazoNo ratings yet
- Approach To Patient With Dyspnea & Ankle Swellling: Dr. Mudhafar Barzani MBCHB, DM, PHD, FRCP Ass. Prof. in CardiologyDocument55 pagesApproach To Patient With Dyspnea & Ankle Swellling: Dr. Mudhafar Barzani MBCHB, DM, PHD, FRCP Ass. Prof. in CardiologyDarawan MirzaNo ratings yet
- Adhf PDFDocument18 pagesAdhf PDFRatnaSuryatiNo ratings yet
- Kegawatdaruratan Bidang Nefrologi Dan Gastrointestinal: Dr. Ni Wayan Sri Wardani, SP - PD, K-GH, FINASIMDocument47 pagesKegawatdaruratan Bidang Nefrologi Dan Gastrointestinal: Dr. Ni Wayan Sri Wardani, SP - PD, K-GH, FINASIMWahyu SuryadinigratNo ratings yet
- Sinkop Dan SyokDocument39 pagesSinkop Dan SyokRosalin Ma'rufNo ratings yet
- Heart FailureDocument47 pagesHeart Failureedry901No ratings yet
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDocument34 pagesHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiNo ratings yet
- Heart FailureDocument80 pagesHeart Failuregalemayehu471No ratings yet
- Secondary Arterial HypertensionDocument32 pagesSecondary Arterial HypertensionAndi SusiloNo ratings yet
- PENYAKIT JANTUNG DAN KEGAWATANNYA PADA BAYI DAN ANAK ... Prof - TeddyDocument101 pagesPENYAKIT JANTUNG DAN KEGAWATANNYA PADA BAYI DAN ANAK ... Prof - TeddyFebriyantiNo ratings yet
- Tabel Kewenangan KlinisDocument243 pagesTabel Kewenangan Klinisfitri evitaNo ratings yet
- Evidence-Based Principles OF Stroke ManagementDocument61 pagesEvidence-Based Principles OF Stroke ManagementBenjamin PrabhuNo ratings yet
- DDX For Oral BoardsDocument10 pagesDDX For Oral BoardshufxllholmbjxwwotmNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- NCLEX RN Practice Questions 17Document6 pagesNCLEX RN Practice Questions 17RI NANo ratings yet
- Cambridge IGCSE™: Combined Science 0653/42 May/June 2022Document12 pagesCambridge IGCSE™: Combined Science 0653/42 May/June 2022Thelma MusvotaNo ratings yet
- Design of Telemonitoring Medical Record of Cardiac Arrhythmia Patients Based On RFID and WEBDocument4 pagesDesign of Telemonitoring Medical Record of Cardiac Arrhythmia Patients Based On RFID and WEBRahul SharmaNo ratings yet
- UsmleDocument3 pagesUsmleuwandfaNo ratings yet
- Atkinson Et Al 2017 Cardiovascular and Ventilatory Consequences of Laparoscopic SurgeryDocument11 pagesAtkinson Et Al 2017 Cardiovascular and Ventilatory Consequences of Laparoscopic Surgeryedu.b.marqueNo ratings yet
- 18Document18 pages18karan_shah_51No ratings yet
- 9 Transport in AnimalssDocument59 pages9 Transport in AnimalssFathmath JameelNo ratings yet
- ShockDocument177 pagesShockISMAIL100% (1)
- Anatomi Organ DR - Siti Rafiah HusainDocument73 pagesAnatomi Organ DR - Siti Rafiah HusainfitrahfajrianihamingNo ratings yet
- Skor Resiko TIMI Untuk UADocument1 pageSkor Resiko TIMI Untuk UAGusnella IswardhaniNo ratings yet
- PPP v3Document771 pagesPPP v3Steven Lam100% (1)
- Nursing Care Plans For Activity IntoleranceDocument4 pagesNursing Care Plans For Activity IntolerancethebigtwirpNo ratings yet
- Breaking News English: Ready-to-Use English Lessons by Sean BanvilleDocument26 pagesBreaking News English: Ready-to-Use English Lessons by Sean BanvilleprofemartaNo ratings yet
- Electric Shocks and Electrocution, Clinical Effects and PathologyDocument9 pagesElectric Shocks and Electrocution, Clinical Effects and PathologyYosuaNo ratings yet
- Second Trimester: Accepting The BabyDocument4 pagesSecond Trimester: Accepting The BabyCharmaine BautistaNo ratings yet
- NGN Case Study 1Document11 pagesNGN Case Study 1api-650043935No ratings yet
- Echocardiography in Congenital Heart Disease - Expert Consult - Online and Print, 1e (Practical Echocardiography)Document239 pagesEchocardiography in Congenital Heart Disease - Expert Consult - Online and Print, 1e (Practical Echocardiography)Sofia OliveiraNo ratings yet
- AngioplastyDocument45 pagesAngioplastym maskNo ratings yet
- 199 Questions-Fcps Part 1 Medicine Paper - PDF 16 November 2011-By PimaDocument13 pages199 Questions-Fcps Part 1 Medicine Paper - PDF 16 November 2011-By PimaServantof Islam100% (5)
- Heart Failure NCLEX QuestionsDocument5 pagesHeart Failure NCLEX QuestionsMelodia Turqueza GandezaNo ratings yet
- WLL-LS1EnglishJHS-Q3W3M5L1-I See, Yet I Don't SeeDocument4 pagesWLL-LS1EnglishJHS-Q3W3M5L1-I See, Yet I Don't SeeAlhena ValloNo ratings yet
- Anatomy & Physiology II Exam #1 Practicum ReviewDocument1 pageAnatomy & Physiology II Exam #1 Practicum ReviewLucyNgoNo ratings yet
- Concept Map Atrial-TachycardiaDocument1 pageConcept Map Atrial-TachycardiaBea Mae DeocampoNo ratings yet
- Rsov CaseDocument41 pagesRsov CaseGajanan GuptaNo ratings yet
- Coronary Heart DiseaseDocument17 pagesCoronary Heart DiseaseAdeliaNo ratings yet
- Slide-Uri Sesiune Fiziologie Pt. StudentiDocument19 pagesSlide-Uri Sesiune Fiziologie Pt. StudentiRaluca Andreea PetcuNo ratings yet
- Exercise Stress TestingDocument54 pagesExercise Stress TestingSaranya R S100% (2)
- Cambridge Assessment International Education: Physical Education 0413/13 October/November 2018Document17 pagesCambridge Assessment International Education: Physical Education 0413/13 October/November 2018Eka AdjieNo ratings yet
- Questions - Homework - 10th - Science - 2021-11-24T05 - 44Document12 pagesQuestions - Homework - 10th - Science - 2021-11-24T05 - 44Saurabh BhattacharyaNo ratings yet