Download as pdf or txt
You might also like
- Crash Course Psychiatry Xiu 5 Ed 2019Document355 pagesCrash Course Psychiatry Xiu 5 Ed 2019Shang100% (6)
- Isabel Clarke, Hazel Nicholls - Third Wave CBT Integration For Individuals and Teams - Comprehend, Cope and Connect (2017, Routledge)Document185 pagesIsabel Clarke, Hazel Nicholls - Third Wave CBT Integration For Individuals and Teams - Comprehend, Cope and Connect (2017, Routledge)Anna Thallita AraujoNo ratings yet
- Clinical Psychology Case Study AllisonDocument9 pagesClinical Psychology Case Study AllisonIoana VoinaNo ratings yet
- Sample Treatment Plan With Goals For Anxiety and DepressionDocument3 pagesSample Treatment Plan With Goals For Anxiety and Depressionمودة عثمان100% (1)
- Final Exam Question Bum2413 Applied StatisticsDocument9 pagesFinal Exam Question Bum2413 Applied StatisticsSyafiq MTNo ratings yet
- Professor Dr. Gerd Ludwig, Professor Dr. Julian Frick (Auth.) - Spermatology - Atlas and Manual-Springer Berlin Heidelberg (1990)Document169 pagesProfessor Dr. Gerd Ludwig, Professor Dr. Julian Frick (Auth.) - Spermatology - Atlas and Manual-Springer Berlin Heidelberg (1990)leandroNo ratings yet
- Psychiatric Mental Health Comprehensive Case StudyDocument14 pagesPsychiatric Mental Health Comprehensive Case Studyapi-546967314No ratings yet
- Kaplan Grade OverviewDocument5 pagesKaplan Grade Overviewapi-310875630No ratings yet
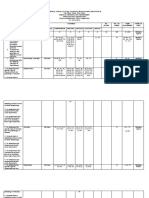
- TOS Preliminary Abnormal PsychologyDocument1 pageTOS Preliminary Abnormal PsychologyJeffreyNo ratings yet
- Arntz, Bpdsi Cut-Off ScoresDocument6 pagesArntz, Bpdsi Cut-Off ScoressunkissedchiffonNo ratings yet
- Cognitive Distortion QuestionnaireDocument7 pagesCognitive Distortion QuestionnaireagusNo ratings yet
- The Conners Adult ADHD Rating Scales ShoDocument25 pagesThe Conners Adult ADHD Rating Scales ShoitmarketingNo ratings yet
- Rating Scales and Safety Measurements in Bipolar Disorder and Schizophrenia - A Reference GuideDocument33 pagesRating Scales and Safety Measurements in Bipolar Disorder and Schizophrenia - A Reference GuideDM YazdaniNo ratings yet
- DMDDDocument10 pagesDMDDTaranpreet KaurNo ratings yet
- Appi Ajp 2017 16091037 ds001Document6 pagesAppi Ajp 2017 16091037 ds001goldfishxNo ratings yet
- PHQ 2 PDFDocument2 pagesPHQ 2 PDFnaufal12345No ratings yet
- Artigo Com Tabelas HVLT e BVMTDocument4 pagesArtigo Com Tabelas HVLT e BVMTMaria CristinaNo ratings yet
- Midterm Examination MGT 600 - Statistical Analysis in MGT and EducationDocument12 pagesMidterm Examination MGT 600 - Statistical Analysis in MGT and EducationJoseph Mark BaldomarNo ratings yet
- 527 Rating ScalesDocument25 pages527 Rating Scalescercuri pătrate de fum100% (1)
- Bondi Et Al.,2014Document15 pagesBondi Et Al.,2014Priscila SelingardiNo ratings yet
- Full Download Essentials of Psychology Concepts and Applications 3rd Edition Nevid Test BankDocument31 pagesFull Download Essentials of Psychology Concepts and Applications 3rd Edition Nevid Test Bankforagedipodysygv100% (37)
- Racaza CKL1 Laboratory3Document2 pagesRacaza CKL1 Laboratory3Jevan Monte RacazaNo ratings yet
- Central Luzon Doctors' Hospital Educational Institution Medical Technology DepartmentDocument4 pagesCentral Luzon Doctors' Hospital Educational Institution Medical Technology Departmentangelina buenaNo ratings yet
- Locus Cueruleos. Trastorno Depresivo Mayor Tardío o Deterioro Cognitivo LeveDocument9 pagesLocus Cueruleos. Trastorno Depresivo Mayor Tardío o Deterioro Cognitivo LeveDORIS JANETHNo ratings yet
- Clinical Assessment TestDocument49 pagesClinical Assessment TestquibblerloverNo ratings yet
- Io TableDocument2 pagesIo TableRenella Mary MapaNo ratings yet
- Molecular Docking Analysis of Some Phytochemicals On Two SARS-CoV-2 Targets by Amaka Ubani, Francis Agwom, Nathan Yakubu ShehuDocument14 pagesMolecular Docking Analysis of Some Phytochemicals On Two SARS-CoV-2 Targets by Amaka Ubani, Francis Agwom, Nathan Yakubu ShehuHICHAM WAHNOUNo ratings yet
- NCLEX Study CalendarDocument1 pageNCLEX Study CalendarOlrac AgairdamNo ratings yet
- Communications and Research Notes: Three-Point Likert Scales Are Good EnoughDocument7 pagesCommunications and Research Notes: Three-Point Likert Scales Are Good EnoughYudiMeidiyansahNo ratings yet
- Letters: Damage To The Prefrontal Cortex Increases Utilitarian Moral JudgementsDocument4 pagesLetters: Damage To The Prefrontal Cortex Increases Utilitarian Moral JudgementsELIANARESTREPONo ratings yet
- Psychology 12Th Edition Wade Test Bank Full Chapter PDFDocument25 pagesPsychology 12Th Edition Wade Test Bank Full Chapter PDFmyquangcak93c100% (12)
- Montgomery-Asberg Depression Rating Scale in Clinical Practice: Psychometric Properties On Serbian PatientsDocument7 pagesMontgomery-Asberg Depression Rating Scale in Clinical Practice: Psychometric Properties On Serbian PatientsjhuNo ratings yet
- American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, Patient Self-Report Section: Reliability, Validity, and ResponsivenessDocument8 pagesAmerican Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form, Patient Self-Report Section: Reliability, Validity, and ResponsivenesstheorthopaedistNo ratings yet
- 3 Huang2015Document10 pages3 Huang2015kikoNo ratings yet
- 2022 Setyowibowo Psychoeducation For BrCa Meta AnalysisDocument16 pages2022 Setyowibowo Psychoeducation For BrCa Meta AnalysisAngélica Fernández PérezNo ratings yet
- Utilitarian MoraljudgmentsDocument4 pagesUtilitarian MoraljudgmentsCarlos Antonio Agurto GonzalesNo ratings yet
- 20th Anniversary Issue: Can Psychopathology and Neuroscience Coexist in Psychiatric Classifications?Document7 pages20th Anniversary Issue: Can Psychopathology and Neuroscience Coexist in Psychiatric Classifications?Sahâmia MartinsNo ratings yet
- Depression and Anxiety in Parkinson 'S Disease: Anette Schrag, Raquel N. TaddeiDocument33 pagesDepression and Anxiety in Parkinson 'S Disease: Anette Schrag, Raquel N. TaddeiMerari Lugo OcañaNo ratings yet
- Dwnload Full Essentials of Psychology Concepts and Applications 3rd Edition Nevid Test Bank PDFDocument36 pagesDwnload Full Essentials of Psychology Concepts and Applications 3rd Edition Nevid Test Bank PDFnoisefulrectrix.qn0x100% (11)
- Accurate Risk Estimation of - Amyloid Positivity To Identify - 2019 - AlzheimerDocument11 pagesAccurate Risk Estimation of - Amyloid Positivity To Identify - 2019 - AlzheimerPriscilla ChantalNo ratings yet
- Bioteknologi B2-24 RapportDocument70 pagesBioteknologi B2-24 RapportPeter Nørgaard MortensenNo ratings yet
- Evaluation Report - Lifotronic H9Document4 pagesEvaluation Report - Lifotronic H9Michael Tanglao100% (1)
- A Brief Cognitive Assessment Tool For SchizophreniaDocument8 pagesA Brief Cognitive Assessment Tool For SchizophreniaRatriningdyah DewiNo ratings yet
- Animal Models in Psychiatric Research The RDoC System As A NewDocument10 pagesAnimal Models in Psychiatric Research The RDoC System As A Newselina hahnNo ratings yet
- Article RAADS 14 ScreenDocument11 pagesArticle RAADS 14 ScreenBoubchir Salah EddineNo ratings yet
- Assessment of Depressive Symptoms People With Diabetic Foot UlcerDocument21 pagesAssessment of Depressive Symptoms People With Diabetic Foot UlcerDjoko PriyonoNo ratings yet
- Statexer#5Document6 pagesStatexer#5Ghost31No ratings yet
- Comprehensive Psychiatry: C. Van Der Merwe, R. Passchier, M. Mufford, R. Ramesar, S. Dalvie, D.J. SteinDocument6 pagesComprehensive Psychiatry: C. Van Der Merwe, R. Passchier, M. Mufford, R. Ramesar, S. Dalvie, D.J. Steinlosviajesdeyora76No ratings yet
- Franieck - L - Günter - M 2010 - On LatencyDocument139 pagesFranieck - L - Günter - M 2010 - On LatencyLuis HernándezNo ratings yet
- Barr2018Document12 pagesBarr2018febrinaNo ratings yet
- Chapter IvDocument18 pagesChapter Ivdenny alfiranggaNo ratings yet
- Semantic Diffrential ScaleDocument3 pagesSemantic Diffrential ScaleSwati SharmaNo ratings yet
- Validation of The French Version of The Auditory Hallucination Rating Scale in A Sample of Hallucinating Patients With SchizophreniaDocument8 pagesValidation of The French Version of The Auditory Hallucination Rating Scale in A Sample of Hallucinating Patients With SchizophreniaAdjali MohamedNo ratings yet
- IO-Miase-Performance Task 2Document14 pagesIO-Miase-Performance Task 2Bea Clarisse MiaseNo ratings yet
- Stijn Vanheule (Auth.) - Psychiatric Diagnosis Revisited - From DSM To Clinical Case Formulation-Palgrave Macmillan (2017)Document252 pagesStijn Vanheule (Auth.) - Psychiatric Diagnosis Revisited - From DSM To Clinical Case Formulation-Palgrave Macmillan (2017)Nicolas GomesNo ratings yet
- ScoliosisDocument5 pagesScoliosisleanhngocumpNo ratings yet
- Plausible ValuesDocument25 pagesPlausible ValuesAbdulla AlshehhiNo ratings yet
- Validación Española ADHD-RSDocument7 pagesValidación Española ADHD-RSCristina Andreu NicuesaNo ratings yet
- General Hospital Psychiatry: Review ArticleDocument10 pagesGeneral Hospital Psychiatry: Review Articlehevi_tarsumNo ratings yet
- Student Version LSD and Problem Solving: Brian Winkel, Director Simiode Cornwall NY USADocument2 pagesStudent Version LSD and Problem Solving: Brian Winkel, Director Simiode Cornwall NY USAPedro DuvanNo ratings yet
- Emotional Indicatores in Children Human Figure PDFDocument275 pagesEmotional Indicatores in Children Human Figure PDFLuciano LeonNo ratings yet
- Reading Comprehension - Decoded '11-'23Document1 pageReading Comprehension - Decoded '11-'23Mohamed ForukNo ratings yet
- Clinical Proteomics: From Diagnosis to TherapyFrom EverandClinical Proteomics: From Diagnosis to TherapyJennifer E. Van EykNo ratings yet
- Ecstatic SuicideDocument20 pagesEcstatic SuicideMarielaNo ratings yet
- NRNP PRAC 6635 Comprehensive Psychiatric Evaluation Template 2Document6 pagesNRNP PRAC 6635 Comprehensive Psychiatric Evaluation Template 2superbwriters10No ratings yet
- Bipolar DisorderDocument19 pagesBipolar Disorderhatem alsrourNo ratings yet
- CHAPTER 3 WordDocument20 pagesCHAPTER 3 WordAubrey RamiloNo ratings yet
- Abnormal Psychology 15th Edition Butcher Test Bank Full Chapter PDFDocument62 pagesAbnormal Psychology 15th Edition Butcher Test Bank Full Chapter PDFDouglasRubiopger100% (14)
- Abnormal Psychology in A Changing World 10th Edition Nevid Test Bank Full Chapter PDFDocument68 pagesAbnormal Psychology in A Changing World 10th Edition Nevid Test Bank Full Chapter PDFannerobinsonebnxfojmza100% (17)
- Antidepressants (ME216) 20 5Document40 pagesAntidepressants (ME216) 20 5Dineish MurugaiahNo ratings yet
- Poverty, Social Inequality and Mental HealthDocument10 pagesPoverty, Social Inequality and Mental HealthMichael PearsonNo ratings yet
- Gender and PsychopathologyDocument333 pagesGender and PsychopathologyMaisa Hormazabal100% (2)
- Assignment 2 PSYC3102Document4 pagesAssignment 2 PSYC3102lisavansetersNo ratings yet
- International Classification of DiseasesDocument10 pagesInternational Classification of DiseasesJona AddatuNo ratings yet
- Case StudyDocument12 pagesCase Studyapi-662613408No ratings yet
- Cambridge III Classification - and - Explanation - of - Depression PDFDocument15 pagesCambridge III Classification - and - Explanation - of - Depression PDFdilaNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- Introduction To DSM 5 2Document61 pagesIntroduction To DSM 5 2denfan100% (1)
- Mental Health AssignmentDocument6 pagesMental Health AssignmentjohnaaaNo ratings yet
- Internship Report 2239361Document15 pagesInternship Report 2239361Reeya RaiNo ratings yet
- Social Support and Self-Esteem Predict Changes in Bipolar Depression But Not ManiaDocument8 pagesSocial Support and Self-Esteem Predict Changes in Bipolar Depression But Not ManiaVia YatalaNo ratings yet
- WPA Educational Programme On Depressive Disorders PDFDocument98 pagesWPA Educational Programme On Depressive Disorders PDFGe NomNo ratings yet
- Grade 11 Qualitative Research DEPRESSIONDocument25 pagesGrade 11 Qualitative Research DEPRESSIONRose Marie100% (1)
- Depression PowerpointDocument25 pagesDepression PowerpointLiezl Salatan AbuzoNo ratings yet
- Northeastern Mindanao CollegesDocument58 pagesNortheastern Mindanao CollegesGliese Grace BuhiaNo ratings yet
- Bipolar Versus Borderline Difference Matter Acta PsychDocument2 pagesBipolar Versus Borderline Difference Matter Acta PsychSalud Mental SantiagoNo ratings yet
- Michael W. Passer, Ronald E Smith - Psychology - The Science of Mind and Behavior-McGraw-Hill Education (2010)Document816 pagesMichael W. Passer, Ronald E Smith - Psychology - The Science of Mind and Behavior-McGraw-Hill Education (2010)ETIKA PATIALNo ratings yet
- Psychology - Case Study of Amy Winehouse - EditedDocument7 pagesPsychology - Case Study of Amy Winehouse - EditedJane SamNo ratings yet
- Psychology Chapter 4 - Psychological DisorderDocument71 pagesPsychology Chapter 4 - Psychological DisorderkhushiNo ratings yet