Download as pdf or txt
You might also like
- Foot Reflexology Complete How To Techniques & Step by Step Instructions!Document10 pagesFoot Reflexology Complete How To Techniques & Step by Step Instructions!Tony MickensNo ratings yet
- Cohen McqsDocument69 pagesCohen McqsSAEED69% (13)
- Pathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer PlayersDocument8 pagesPathogenic Factors Associated With Osgood-Schlatter Disease in Adolescent Male Soccer PlayersBreechesNo ratings yet
- Back To Sports After Arthroscopic Revision Bankart Repair: Original ResearchDocument7 pagesBack To Sports After Arthroscopic Revision Bankart Repair: Original ResearchMiftahul IlmiNo ratings yet
- Relationships Between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players PDFDocument11 pagesRelationships Between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players PDFOriol Ruiz PujolNo ratings yet
- Review of LiteratureDocument3 pagesReview of LiteratureArsynNo ratings yet
- Angoorani 2021Document9 pagesAngoorani 2021Jayne PereiraNo ratings yet
- Willems 2005Document9 pagesWillems 2005Johann Sebastian CruzNo ratings yet
- Dynamic Balance Performance and Noncontact Lower Extremity Injury in College Football Players: An Initial StudyDocument6 pagesDynamic Balance Performance and Noncontact Lower Extremity Injury in College Football Players: An Initial StudyFachrun SofiyahNo ratings yet
- 36 Physiological and Performance TestingDocument2 pages36 Physiological and Performance TestingWhooper GamestorNo ratings yet
- International Journal of Chemtech Research: Nabil .A. Mohamed and Maha. M. MohamedDocument11 pagesInternational Journal of Chemtech Research: Nabil .A. Mohamed and Maha. M. MohamedHari25885No ratings yet
- Alterations in Peak Ground-Reaction Force During 60-cm Drop Landings Caused by A Single Session of Repeated Wingate Anaerobic TestsDocument7 pagesAlterations in Peak Ground-Reaction Force During 60-cm Drop Landings Caused by A Single Session of Repeated Wingate Anaerobic TestsIlham MaulanaNo ratings yet
- Outcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact SportsDocument8 pagesOutcomes After Arthroscopic Bankart Repair in Adolescent Athletes Participating in Collision and Contact SportsIsmail Tidak Ada KepanjanganNo ratings yet
- 2016 Baseline Time To StabilizationDocument5 pages2016 Baseline Time To Stabilizationktan.lboroNo ratings yet
- Differences in Landing and Balance Deficits at The Ankle Joint On Stable and Unstable Surfaces in Inflexible and Flexible Handball PlayersDocument8 pagesDifferences in Landing and Balance Deficits at The Ankle Joint On Stable and Unstable Surfaces in Inflexible and Flexible Handball PlayersAJHSSR JournalNo ratings yet
- Parpa & Michaelides 2022Document7 pagesParpa & Michaelides 2022Taha IliasNo ratings yet
- Prevention of Shoulder Injuries in Overhead AthletesDocument26 pagesPrevention of Shoulder Injuries in Overhead AthletesAmeerah KhraisatNo ratings yet
- Nihms782171 PDFDocument15 pagesNihms782171 PDFjacknatalieNo ratings yet
- Relationship Between Training Load and Recovery in Collegiate American Football Players During Pre-Season TrainingDocument10 pagesRelationship Between Training Load and Recovery in Collegiate American Football Players During Pre-Season TrainingtayfunertebelNo ratings yet
- Research Article: Injury Risk Prediction of Aerobics Athletes Based On Big Data and Computer VisionDocument10 pagesResearch Article: Injury Risk Prediction of Aerobics Athletes Based On Big Data and Computer VisionYẾN TRẦN NGỌCNo ratings yet
- Prevention of Shoulder Injuries in Overhead AthletesDocument9 pagesPrevention of Shoulder Injuries in Overhead AthletesLeonardiniNo ratings yet
- SM October 2021 AbdallahDocument8 pagesSM October 2021 AbdallahQuenton CompasNo ratings yet
- Sports Injuries in Soccer According To Tactical Position: A Retrospective SurveyDocument9 pagesSports Injuries in Soccer According To Tactical Position: A Retrospective SurveyPlayboi JillNo ratings yet
- Physical Exercises For Preventing Injuries Among Adult Male Football Players PDFDocument8 pagesPhysical Exercises For Preventing Injuries Among Adult Male Football Players PDFInês AntunesNo ratings yet
- Orthop J Sports Med 2021 9 7 23259671211013394Document6 pagesOrthop J Sports Med 2021 9 7 23259671211013394Fernando SousaNo ratings yet
- Paper 4Document5 pagesPaper 4Sting RayNo ratings yet
- Cartilage Sports16Document19 pagesCartilage Sports16scribidubiduNo ratings yet
- LCA Psicologico 2Document6 pagesLCA Psicologico 2MarianoNo ratings yet
- Newton2006 PDFDocument7 pagesNewton2006 PDFAlexandre FerreiraNo ratings yet
- 2Document6 pages2Rashmi GodeshwerNo ratings yet
- Epidemiology of InjuriesDocument15 pagesEpidemiology of InjuriesAlexandru ChivaranNo ratings yet
- 435185blkkgs - Reliability and Factorial Validity of Flexibility.401Document9 pages435185blkkgs - Reliability and Factorial Validity of Flexibility.401Hari25885No ratings yet
- Hip & Groin Pain DD PDFDocument15 pagesHip & Groin Pain DD PDFagniosaiNo ratings yet
- Development of Screening Test Battery For Volleyball Players A Mixed Method StudyDocument12 pagesDevelopment of Screening Test Battery For Volleyball Players A Mixed Method StudyScott_PTNo ratings yet
- Sports-Related Injuries in Athletes With Disabilities: ReviewDocument12 pagesSports-Related Injuries in Athletes With Disabilities: Reviewangelica barrazaNo ratings yet
- Pre-Tournament ScreenDocument9 pagesPre-Tournament ScreenHussain MirzaNo ratings yet
- 10 (2) Return To Play After Shoulder Instability in National Football League Athletes (Andi Ainun Zulkiah Surur) IIDocument6 pages10 (2) Return To Play After Shoulder Instability in National Football League Athletes (Andi Ainun Zulkiah Surur) IIainunNo ratings yet
- Dynamic Taping Improves Landing Biomechanics in YoungDocument12 pagesDynamic Taping Improves Landing Biomechanics in YoungArthur CalegariNo ratings yet
- Ijerph 19 13716 v2Document11 pagesIjerph 19 13716 v2allfit.davidNo ratings yet
- 2008-Croisier-Strength Imbalances and Prevention of Hamstring Injury in Professional Soccer Players - Isokinetic HQ RatioDocument7 pages2008-Croisier-Strength Imbalances and Prevention of Hamstring Injury in Professional Soccer Players - Isokinetic HQ RatioFederico BristotNo ratings yet
- Lower Back Injuries in National Collegiate Athletic Association Football PlayersDocument7 pagesLower Back Injuries in National Collegiate Athletic Association Football PlayersirmarizkyyNo ratings yet
- International Journal of Sports Science & MedicineDocument5 pagesInternational Journal of Sports Science & MedicineSciresNo ratings yet
- Injury Patterns, Risk Factors, and Return To Sport in Brazilian Jiu Jitsu A Cross Sectional Study of 1140 AthletesDocument9 pagesInjury Patterns, Risk Factors, and Return To Sport in Brazilian Jiu Jitsu A Cross Sectional Study of 1140 Athletesvr9vwbbx9hNo ratings yet
- Healthcare 10 01822Document18 pagesHealthcare 10 01822David HaluliNo ratings yet
- Technique and Ankle-Dorsiflexion Range of Motion Are Not With The History of Lower Limb Injuries Among Youth AthletesDocument10 pagesTechnique and Ankle-Dorsiflexion Range of Motion Are Not With The History of Lower Limb Injuries Among Youth AthletesJamie DavisNo ratings yet
- Rehabilitation of The Ankle After Acute Sprain or Chronic InstabilityDocument17 pagesRehabilitation of The Ankle After Acute Sprain or Chronic InstabilityAndres Ignacio Lastra MillanNo ratings yet
- SEBT As A Predictor of Lower Extremity Injury in High School Basketball PlayersDocument9 pagesSEBT As A Predictor of Lower Extremity Injury in High School Basketball PlayersFebryLasantiNo ratings yet
- Patellar Tendon Structure Responds To Load Over A 7 Week Preseason in Elite Male Volleyball PlayersDocument8 pagesPatellar Tendon Structure Responds To Load Over A 7 Week Preseason in Elite Male Volleyball PlayersVicente Ignacio Ormazábal MedinaNo ratings yet
- Apiv1articles27975 The Neuromuscular Effects of The Copenhagen Adductor Exercise A SystematicDocument12 pagesApiv1articles27975 The Neuromuscular Effects of The Copenhagen Adductor Exercise A SystematicItamar CarvalhoNo ratings yet
- Fundamental Movement and DynamicDocument9 pagesFundamental Movement and DynamicYoh ChenNo ratings yet
- Anterior Cruciate Ligament Reconstruction Increases The Risk of Hamstring Strain Injury Across Football Codes in AustraliaDocument10 pagesAnterior Cruciate Ligament Reconstruction Increases The Risk of Hamstring Strain Injury Across Football Codes in AustraliaYassir EL YAKHLOUFINo ratings yet
- Amateur and Recreational Athletes Return To Sport at A High Rate Following Hip Arthroscopy For Femoroacetabular ImpingementDocument8 pagesAmateur and Recreational Athletes Return To Sport at A High Rate Following Hip Arthroscopy For Femoroacetabular ImpingementMiguel Antonio Arce ParedesNo ratings yet
- YENER 2022 - The Association Between Sport-Related Concussion and Musculoskeletal Injury in University Rugby AthletesDocument7 pagesYENER 2022 - The Association Between Sport-Related Concussion and Musculoskeletal Injury in University Rugby AthletesMauricio ZeniNo ratings yet
- A Rare Soccer Related Injury Traumatic PosteriorDocument6 pagesA Rare Soccer Related Injury Traumatic PosteriorDr. Andre Lopes PhD.No ratings yet
- Relationship Between The Y Balance Test Scores and Soft Tissue Injury Incidence in A Soccer TeamDocument12 pagesRelationship Between The Y Balance Test Scores and Soft Tissue Injury Incidence in A Soccer TeamBelva EdinaNo ratings yet
- Efficacy of Moist Heat Pack ApplicationDocument4 pagesEfficacy of Moist Heat Pack ApplicationDaniel Garcia del PinoNo ratings yet
- Watkins Et Al. (2022)Document9 pagesWatkins Et Al. (2022)DANIA NAJUA BINTI ZAINALNo ratings yet
- Risk and Protective Factors For Shoulder Complaints in Indoor Volleyball PlayersDocument6 pagesRisk and Protective Factors For Shoulder Complaints in Indoor Volleyball PlayersVlad TomaNo ratings yet
- Volleyball InjuryDocument7 pagesVolleyball InjuryAnggia PNo ratings yet
- Copenhagen ExsDocument10 pagesCopenhagen ExsHajra Bai RasheedNo ratings yet
- Research Article Are Sprint Accelerations Related To Groin Injuries? A Biomechanical Analysis of Adolescent Soccer PlayersDocument14 pagesResearch Article Are Sprint Accelerations Related To Groin Injuries? A Biomechanical Analysis of Adolescent Soccer PlayerskevinNo ratings yet
- Muscle Damage and Its Relationship With Muscle Fatigue During A Half-Iron TriathlonDocument7 pagesMuscle Damage and Its Relationship With Muscle Fatigue During A Half-Iron TriathlonNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- The Effects of Massage On Delayed Onset Muscle Soreness: Original ArticleDocument4 pagesThe Effects of Massage On Delayed Onset Muscle Soreness: Original ArticleNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- The Cross-Bridge Cycle and Skeletal Muscle Fatigue: Fatigue Mechanisms Determining Exercise PerformanceDocument8 pagesThe Cross-Bridge Cycle and Skeletal Muscle Fatigue: Fatigue Mechanisms Determining Exercise PerformanceNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Congenital Indifference To Pain: An Illustrated Case Report and Literature ReviewDocument8 pagesCongenital Indifference To Pain: An Illustrated Case Report and Literature ReviewNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- The Prevention of Ankle Sprains in Sports. A Systematic Review of The LiteratureDocument9 pagesThe Prevention of Ankle Sprains in Sports. A Systematic Review of The LiteratureNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Effects of Reduced Muscle Ca2+ Release and Contractile Protein Function Intact Skeletal MuscleDocument13 pagesEffects of Reduced Muscle Ca2+ Release and Contractile Protein Function Intact Skeletal MuscleNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Hammami 2016Document33 pagesHammami 2016NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Interaction Between Pain, Movement, and Physical ActivityDocument11 pagesInteraction Between Pain, Movement, and Physical ActivityNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Mechanisms of Insulin Action and Insulin Resistance (Petersen y Shulman, 2018)Document91 pagesMechanisms of Insulin Action and Insulin Resistance (Petersen y Shulman, 2018)NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Volleyball/Basketball Return To Play Protocol - Ankle SprainDocument1 pageVolleyball/Basketball Return To Play Protocol - Ankle SprainNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Polzer 201Document12 pagesPolzer 201NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Returntoplayfollowing Anklesprainandlateral LigamentreconstructionDocument13 pagesReturntoplayfollowing Anklesprainandlateral LigamentreconstructionNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Online First Online First: Proprioceptive Training For The Prevention of Ankle Sprains: An Evidence-Based ReviewDocument3 pagesOnline First Online First: Proprioceptive Training For The Prevention of Ankle Sprains: An Evidence-Based ReviewNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Konor Et Al 2012 PDFDocument9 pagesKonor Et Al 2012 PDFNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Functional Movement Screen and Y-Balance Test: Validity in Hamstring Injury Risk Prediction?Document74 pagesFunctional Movement Screen and Y-Balance Test: Validity in Hamstring Injury Risk Prediction?NICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Peroneal Reaction Time Instability of The Ankle in Treated FunctionalDocument8 pagesPeroneal Reaction Time Instability of The Ankle in Treated FunctionalNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Hernia Discal en Atletas de EliteDocument8 pagesHernia Discal en Atletas de EliteNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Acta Medica Mediterranea, 2017, 33: 651: Igdem UlganDocument6 pagesActa Medica Mediterranea, 2017, 33: 651: Igdem UlganNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Functional Screening enDocument19 pagesFunctional Screening enNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Kenco Press The Small Press Specialist - MaintenanceDocument2 pagesKenco Press The Small Press Specialist - MaintenancexyzNo ratings yet
- Case Study of Head Injury SijiDocument30 pagesCase Study of Head Injury SijiJinal PatelNo ratings yet
- OH&SDocument19 pagesOH&SDwin RoscoNo ratings yet
- AmbulationDocument28 pagesAmbulationding dutollo100% (1)
- Dead Walk Again 3.03Document52 pagesDead Walk Again 3.03pimpy3No ratings yet
- Tema 4 - Standing, Sitting PosDocument18 pagesTema 4 - Standing, Sitting PosAndreea ProdescuNo ratings yet
- Multi OrganDocument10 pagesMulti OrganthyinkslingerNo ratings yet
- Trauma and OrthopedicsDocument134 pagesTrauma and OrthopedicsAdebisiNo ratings yet
- 01lowback PDFDocument2 pages01lowback PDFkotza100% (1)
- Work SimplificationDocument2 pagesWork SimplificationShahriar Hasan100% (1)
- Tumble Action Washer: Use & Care GuideDocument11 pagesTumble Action Washer: Use & Care GuidetheussatNo ratings yet
- 11 Suturing21012015Document30 pages11 Suturing21012015Putri Sari SeptirianiNo ratings yet
- Corrective Exercise The Lumbo Pelvic GirdleDocument9 pagesCorrective Exercise The Lumbo Pelvic GirdlealmaformaNo ratings yet
- Acetabular FractureDocument37 pagesAcetabular FractureSandeep Gurung Nepali100% (1)
- The Wordsley Step Incision For Axillary Lymph-Node DissectionDocument1 pageThe Wordsley Step Incision For Axillary Lymph-Node DissectionVlad GrigoreNo ratings yet
- Research Paper 1 2Document12 pagesResearch Paper 1 2api-549249381No ratings yet
- Crim QuizzleerDocument4 pagesCrim QuizzleerJoanne Rosaldes AlaNo ratings yet
- Pinza 2Document2 pagesPinza 2Carlos Andres Cuaquira CandiaNo ratings yet
- Repetitive Strain InjuryDocument8 pagesRepetitive Strain InjurynyamuhungujeanNo ratings yet
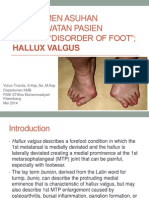
- Manajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREEDocument29 pagesManajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREENovita DamaiyantiNo ratings yet
- Lets Talk About ACCIDENTSDocument3 pagesLets Talk About ACCIDENTSnareff1975No ratings yet
- Unhappy Triad of O'DonahueDocument14 pagesUnhappy Triad of O'DonahueGuadalupe GuzmánNo ratings yet
- Pme PT Apps Dec 2022Document6 pagesPme PT Apps Dec 2022Carlo NiñoNo ratings yet
- Localization of Function in The BrainDocument17 pagesLocalization of Function in The BrainEsaïe GreñaNo ratings yet
- Safety Program: Sic Code 7342Document24 pagesSafety Program: Sic Code 7342kamran100% (1)
- Bone TumorDocument36 pagesBone TumorMoch NizamNo ratings yet
- List of Incidents at Walt Disney World - WikipediaDocument1 pageList of Incidents at Walt Disney World - WikipediaDanna MirandaNo ratings yet
- Experiments and Observations On The Gastric Juice, and The Physiology of Digestion PDFDocument290 pagesExperiments and Observations On The Gastric Juice, and The Physiology of Digestion PDFjmishevskiNo ratings yet