Download as pdf or txt
You might also like
- Nebdn National Diploma in Dental Nursing Practical Experience Record SheetDocument8 pagesNebdn National Diploma in Dental Nursing Practical Experience Record SheetCamila Walton100% (6)
- Miracles From The Vault... More Than 90 Life Saving, Award Winning 'Underground Cures' (Health & Alternative Medicine) (Health Science Institute)Document6 pagesMiracles From The Vault... More Than 90 Life Saving, Award Winning 'Underground Cures' (Health & Alternative Medicine) (Health Science Institute)prakash0% (7)
- Acute Kidney Injury Concept MapDocument1 pageAcute Kidney Injury Concept MapKEn PilapilNo ratings yet
- Antihypertensive DrugsDocument2 pagesAntihypertensive DrugsJillary LlagunoNo ratings yet
- Hypokalemia 180813073624Document26 pagesHypokalemia 180813073624korotkofNo ratings yet
- Colloids and CrystalooidsDocument42 pagesColloids and Crystalooidsلؤي زعيترNo ratings yet
- 12.intraoperative Fluid ManagmentDocument54 pages12.intraoperative Fluid ManagmentyeabsraNo ratings yet
- Pocket Card - IV Fluids - September 2021Document6 pagesPocket Card - IV Fluids - September 2021NeweeJoonYowNo ratings yet
- Burns CH 25 n-7Document7 pagesBurns CH 25 n-7Jessica VargasNo ratings yet
- Isosmotic Volume ContractionDocument9 pagesIsosmotic Volume ContractionFlower100% (1)
- Dengue CaseDocument4 pagesDengue CaseHo Yong WaiNo ratings yet
- HypernatremiaDocument5 pagesHypernatremiaTrio San LuisNo ratings yet
- Management of Dengue FeverDocument16 pagesManagement of Dengue FeverSupriyati Rahayu0% (1)
- Steroids Drug ListDocument2 pagesSteroids Drug ListJezKagandahanNo ratings yet
- Nasal ObstructionDocument100 pagesNasal ObstructionVicky SankaranNo ratings yet
- Wound AssessmentDocument19 pagesWound Assessmentdrsonuchawla100% (1)
- HyponatremiaDocument6 pagesHyponatremiaJaymart Saclolo CostillasNo ratings yet
- HypokalemiaDocument7 pagesHypokalemiaNader SmadiNo ratings yet
- ShockDocument24 pagesShockYaacub IbrahimNo ratings yet
- Clinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Document13 pagesClinical Practice Guidelines: Management of Type 2 Diabetes Mellitus (5 Edition) 2015Azim Abd Razak100% (1)
- 2 Acute Myocardial InfarctionDocument15 pages2 Acute Myocardial InfarctionpauchanmnlNo ratings yet
- Drug Study Drug Name Classificatio N Dosage/ Prepatarion Indication Contraindication Side Effects Nursing ResponsibilitiesDocument4 pagesDrug Study Drug Name Classificatio N Dosage/ Prepatarion Indication Contraindication Side Effects Nursing ResponsibilitiesTheresa AbrilloNo ratings yet
- Anatomy of Trachea: Dr. Mohammed Mahmoud MosaedDocument14 pagesAnatomy of Trachea: Dr. Mohammed Mahmoud MosaedrayaimNo ratings yet
- DehydrationDocument2 pagesDehydrationJennyu YuNo ratings yet
- Deep Vein ThrombosisDocument9 pagesDeep Vein ThrombosisGladys YaresNo ratings yet
- Management of HypokalemiaDocument6 pagesManagement of HypokalemiaEsraa Abu elelaNo ratings yet
- Fluid and Electrolyte ImbalanceDocument27 pagesFluid and Electrolyte ImbalanceSimmi Sidhu100% (1)
- Traumatic Brain Injury (TBI) : Epidural Hematoma Subdural HematomaDocument62 pagesTraumatic Brain Injury (TBI) : Epidural Hematoma Subdural HematomaRey AlwiwikhNo ratings yet
- BitesDocument18 pagesBitesPriya SharmaNo ratings yet
- Simmond's Disease MSDocument22 pagesSimmond's Disease MSRocel Devilles100% (1)
- The Child With Hematologic DisordersDocument149 pagesThe Child With Hematologic DisordersNics FranciscoNo ratings yet
- RBC AliquotsDocument1 pageRBC AliquotsARIF AHAMMEDNo ratings yet
- CKDDocument35 pagesCKDgailNo ratings yet
- Narrative PathophysiologyDocument18 pagesNarrative PathophysiologyNica Georgelle Maniego SamonteNo ratings yet
- Supraventricular TachycardiaDocument9 pagesSupraventricular TachycardiaclubsanatateNo ratings yet
- Management of Acute Gastroenteritis in ChildrenDocument14 pagesManagement of Acute Gastroenteritis in ChildrenYayaNo ratings yet
- Choosing Between Colloids and Crystalloids For IV InfusionDocument4 pagesChoosing Between Colloids and Crystalloids For IV InfusionFamily Prepper100% (1)
- 8a) Chronic DacryocystitisDocument5 pages8a) Chronic DacryocystitisDasNo ratings yet
- Anaphylaxis CEACCP 2004Document3 pagesAnaphylaxis CEACCP 2004kuruppukarlNo ratings yet
- 100 Beats Per Minute. Many DifferentDocument4 pages100 Beats Per Minute. Many Differentjovan teopizNo ratings yet
- Clinical Manifestations and Treatment of HypokalemiaDocument16 pagesClinical Manifestations and Treatment of Hypokalemiagerontogeria100% (2)
- Alpha Adrenergic BlockersDocument7 pagesAlpha Adrenergic BlockersNadine BacalangcoNo ratings yet
- Dysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1onDocument4 pagesDysrhythmias 1: Cardiac Conduc1on System Rhythm Strip Recogni1ontantalizin marieNo ratings yet
- Case Study Renal NursingDocument33 pagesCase Study Renal NursingZURAINI BT HARON (ILKKMKUBANGKERIAN)100% (1)
- Blood Glucose LogBookDocument48 pagesBlood Glucose LogBooksteveroe_77No ratings yet
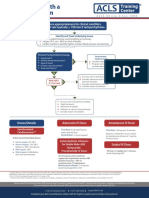
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- Diabetes MellitusDocument15 pagesDiabetes Mellitusfayeniwa100% (1)
- Syndrome of Inappropriate Antidiuretic Hormone (Siadh) : Reported by Jo Jo AleDocument9 pagesSyndrome of Inappropriate Antidiuretic Hormone (Siadh) : Reported by Jo Jo Ale8hg100% (3)
- Drug StudyDocument7 pagesDrug Studyanne009No ratings yet
- Electrolyte AbnormalitiesDocument74 pagesElectrolyte Abnormalitiesbluecrush1No ratings yet
- Right Bundle Branch BlockDocument13 pagesRight Bundle Branch BlockKweenie QueenieNo ratings yet
- Valvularheart Diseases: PathophysiologyDocument9 pagesValvularheart Diseases: PathophysiologyVoid LessNo ratings yet
- Anemia IntroductionDocument15 pagesAnemia IntroductionNitesh Kotian100% (1)
- Anaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangDocument15 pagesAnaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangTeguh PambudiNo ratings yet
- Cretenism Case StudyDocument8 pagesCretenism Case StudyMonica Marie MoralesNo ratings yet
- SuturesDocument62 pagesSuturesShanmuga PriyaNo ratings yet
- Iv Fluids: Beneficial or More Harm?Document20 pagesIv Fluids: Beneficial or More Harm?NinaNo ratings yet
- Intravenous FluidsDocument19 pagesIntravenous Fluidsblack pink in ur area 21100% (1)
- Fluid Management in ICUDocument37 pagesFluid Management in ICUمحمد قاسمNo ratings yet
- 1.1a Fluid Management 6th Seminar GRP AaDocument40 pages1.1a Fluid Management 6th Seminar GRP AahalearnNo ratings yet
- Refreshing " Fluid Therapy"Document28 pagesRefreshing " Fluid Therapy"Bangun Cholifa nusantaraNo ratings yet
- The Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?From EverandThe Spectrum of Amniotic Fluid Embolism: Is Intralipid the solution ?No ratings yet
- Drowning PhysDocument1 pageDrowning Physmentor67No ratings yet
- Autism and Juvenile Justice SystemDocument9 pagesAutism and Juvenile Justice SystemJames Michael HannahNo ratings yet
- Fading Kitten ProtocolDocument1 pageFading Kitten ProtocolSittie Alnaifa AnginNo ratings yet
- Kardex: Mental Status: Activities: Diet: Tubes: Special InfoDocument3 pagesKardex: Mental Status: Activities: Diet: Tubes: Special InfoJanelle Cabida SupnadNo ratings yet
- Management of Acute Gouty Arthritis With A Polyherbal Unani FormulationDocument148 pagesManagement of Acute Gouty Arthritis With A Polyherbal Unani Formulationadilnnj100% (1)
- Role of Albumin in Cirrhosis: From A Hospitalist's PerspectiveDocument8 pagesRole of Albumin in Cirrhosis: From A Hospitalist's PerspectivePutri PitalokaNo ratings yet
- What Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Document2 pagesWhat Is Osteopenia?: What Are Causes and Risk Factors For Osteopenia?Jeremy EvansNo ratings yet
- Overlap Syn AniDocument59 pagesOverlap Syn AniAnimesh AryaNo ratings yet
- Proofed Nurs 2020 LearnDocument5 pagesProofed Nurs 2020 Learnapi-313199824No ratings yet
- Ascaris LumbricoidesDocument33 pagesAscaris LumbricoidesBio SciencesNo ratings yet
- What Is The Digestive System?Document5 pagesWhat Is The Digestive System?SlaheddineNo ratings yet
- California DENTALDocument13 pagesCalifornia DENTALAnheliqaNo ratings yet
- Adenocarcinoma PulmonarDocument75 pagesAdenocarcinoma PulmonarLigia Micaela García XitamulNo ratings yet
- Application For LicenseDocument11 pagesApplication For LicenseSadaf RizwanhumayoonNo ratings yet
- Physiologic Changes in ElderlyDocument6 pagesPhysiologic Changes in ElderlyAngelie PantajoNo ratings yet
- Chapter 21 Male ReproDocument34 pagesChapter 21 Male ReproIsfahan MasulotNo ratings yet
- Infectious Diseases EpidemiologyDocument28 pagesInfectious Diseases EpidemiologySarad Chand YadavNo ratings yet
- Assessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportDocument4 pagesAssessment of Alveolar Bone Augmentation in Intrabony Defects Employing Platelet-Rich Fibrin (PRF) Membrane and Sticky Bone (Injectable-PRF & Demineralized Freeze-Dried Bone Graft) - A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- UKPAR COVID 19 Vaccine AstraZeneca 23.02.2021Document58 pagesUKPAR COVID 19 Vaccine AstraZeneca 23.02.2021SelenaNo ratings yet
- Radio Immuno As SayDocument35 pagesRadio Immuno As SayDawlat SalamaNo ratings yet
- Ecg PDFDocument38 pagesEcg PDFKeerthana BalachandiranNo ratings yet
- ImagingDocument2 pagesImagingFitri WirastamiNo ratings yet
- What Happens During and After A ColonosDocument4 pagesWhat Happens During and After A ColonosAhmed Abd El AzizNo ratings yet
- The Cardiovascular System: The Heart: Anatomy and PhysiologyDocument30 pagesThe Cardiovascular System: The Heart: Anatomy and PhysiologyZachary CohenNo ratings yet
- DEATH I .Ppt1Document219 pagesDEATH I .Ppt1AttiqaQureshi100% (1)
- Effect of Corona Pandemic On Hospitality and Tourism IndustryDocument3 pagesEffect of Corona Pandemic On Hospitality and Tourism IndustryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Immune Thrombocytopenic Purpura in A Patient With Covid-19: CorrespondenceDocument2 pagesImmune Thrombocytopenic Purpura in A Patient With Covid-19: CorrespondencextineNo ratings yet
- Blood ConservationDocument7 pagesBlood ConservationbobbykrishNo ratings yet