Download as doc, pdf, or txt
You might also like
- Cesarian Section Case PresentationDocument26 pagesCesarian Section Case PresentationMae Azores86% (51)
- Nebosh Idip Unit B: B1 Managing Occupational Health 2017Document44 pagesNebosh Idip Unit B: B1 Managing Occupational Health 2017francis100% (1)
- Cap 26 - 1Document26 pagesCap 26 - 1Nancy GuamanNo ratings yet
- Cesarean Delivery: History of The Procedure: The Exact Origin of The Term Cesarean Is Unclear. TheDocument18 pagesCesarean Delivery: History of The Procedure: The Exact Origin of The Term Cesarean Is Unclear. TheCaro Lina Lina100% (1)
- Case StudyDocument7 pagesCase Studymark kennethNo ratings yet
- Obstetricia Iii Placenta AcretaDocument22 pagesObstetricia Iii Placenta AcretaHugo GutiérrezNo ratings yet
- Complications of Caesarean Section: ReviewDocument8 pagesComplications of Caesarean Section: ReviewDesi Purnamasari YanwarNo ratings yet
- Elective Primary Cesarean Delivery: Sounding BoardDocument6 pagesElective Primary Cesarean Delivery: Sounding BoardNicole Grace VillegasNo ratings yet
- Cesarean SectionDocument110 pagesCesarean SectionyordiNo ratings yet
- Disease Intity CsDocument7 pagesDisease Intity CsMary Rose LinatocNo ratings yet
- IntroductionDocument13 pagesIntroductionpurityobotNo ratings yet
- Abnormal PlacentationDocument9 pagesAbnormal PlacentationJack BladeNo ratings yet
- Cesarean Section or Vaginal Delivery in The 21st CenturyDocument2 pagesCesarean Section or Vaginal Delivery in The 21st CenturyLailaNo ratings yet
- Identifying Risk Factors For Uterine RuptureDocument15 pagesIdentifying Risk Factors For Uterine RuptureSakena NurzaNo ratings yet
- Safe Prevention of The Primary CS DeliveryDocument19 pagesSafe Prevention of The Primary CS DeliveryCleoGomezNo ratings yet
- Chapter TwoDocument7 pagesChapter Twohanixasan2002No ratings yet
- Silver 2015Document15 pagesSilver 2015Farlinda AlyaNo ratings yet
- Articulo 8Document15 pagesArticulo 8Monica ReyesNo ratings yet
- Cesarean SectionDocument139 pagesCesarean SectionMisganaw WorkuNo ratings yet
- Caesareans Section Scar Ectopic Pregnancy: An Emerging ChallengeDocument24 pagesCaesareans Section Scar Ectopic Pregnancy: An Emerging Challengenighshift serialsleeperNo ratings yet
- History: Records of The Grand HistorianDocument7 pagesHistory: Records of The Grand HistorianMarienel FuertesNo ratings yet
- EArl Case StudyDocument35 pagesEArl Case StudyAna LuisaNo ratings yet
- Planned Elective Cesarean Section: A Reasonable Choice For Some Women?Document2 pagesPlanned Elective Cesarean Section: A Reasonable Choice For Some Women?miss betawiNo ratings yet
- Caesarian Section: Case PresentationDocument23 pagesCaesarian Section: Case PresentationRiza Angela BarazanNo ratings yet
- Indication For CsDocument20 pagesIndication For CsSandiNo ratings yet
- Caserian SectionDocument100 pagesCaserian SectionsindhujojoNo ratings yet
- Placenta Previa PDFDocument15 pagesPlacenta Previa PDFDamaris GonzálezNo ratings yet
- Cesarean Section Trends and Outcomes in Jinja Regional Referral Hospital A Retrospective AnalysisDocument12 pagesCesarean Section Trends and Outcomes in Jinja Regional Referral Hospital A Retrospective AnalysisKIU PUBLICATION AND EXTENSIONNo ratings yet
- Committee Opinion: Placenta AccretaDocument5 pagesCommittee Opinion: Placenta AccretaagungNo ratings yet
- Jurnal Plasenta Akreta PDFDocument5 pagesJurnal Plasenta Akreta PDFfatqur28No ratings yet
- Trial of Labor After Cesarean (TOLAC)Document16 pagesTrial of Labor After Cesarean (TOLAC)Ricko Handen UriaNo ratings yet
- Sutura CesareasDocument10 pagesSutura CesareasalexNo ratings yet
- Committee Opinion: Placenta AccretaDocument5 pagesCommittee Opinion: Placenta AccretabebetteryesyoucanNo ratings yet
- VBACDocument3 pagesVBACAileen GoNo ratings yet
- Case Study Placenta AccretaDocument6 pagesCase Study Placenta AccretaBecca MirandaNo ratings yet
- Premature Rupture ofDocument4 pagesPremature Rupture ofEllyna EkaNo ratings yet
- Committee Opinion: Scheduled Cesarean Delivery and The Prevention of Vertical Transmission of HIV InfectionDocument4 pagesCommittee Opinion: Scheduled Cesarean Delivery and The Prevention of Vertical Transmission of HIV InfectionHerry SasukeNo ratings yet
- Thesis On Ectopic Pregnancy in IndiaDocument7 pagesThesis On Ectopic Pregnancy in Indiaynwtcpwff100% (2)
- Cesarean Scar Ectopic Pregnancies: Etiology, Diagnosis, and ManagementDocument9 pagesCesarean Scar Ectopic Pregnancies: Etiology, Diagnosis, and ManagementDinorah MarcelaNo ratings yet
- 11 Abnormal PlacentationDocument29 pages11 Abnormal PlacentationMaria Gabriela CristanchoNo ratings yet
- Society For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyDocument13 pagesSociety For Maternal-Fetal Medicine (SMFM) Consult Series #49: Cesarean Scar PregnancyTandyo TriasmoroNo ratings yet
- Acreta 2014Document12 pagesAcreta 2014pshz92No ratings yet
- Managing Placenta Accreta: Incidence and PathophysiologyDocument9 pagesManaging Placenta Accreta: Incidence and PathophysiologyAslesa Wangpathi PagehgiriNo ratings yet
- EctopicwDocument9 pagesEctopicwdrnunungNo ratings yet
- Predicting Cesarean Section AnDocument5 pagesPredicting Cesarean Section AnKEANNA ZURRIAGANo ratings yet
- IOSRPHRDocument3 pagesIOSRPHRIOSR Journal of PharmacyNo ratings yet
- C-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Document7 pagesC-Obs 38 Planned Vaginal Birth After C-Section New Jul 10Aris SugiatnoNo ratings yet
- Reading Part A CaesareanDocument6 pagesReading Part A Caesareanfernanda1rondelliNo ratings yet
- Cesarean Section Vbac: January, 2009Document43 pagesCesarean Section Vbac: January, 2009DanduuNo ratings yet
- The Back Alley Revisited: Sepsis After Attempted Self-Induced AbortionDocument3 pagesThe Back Alley Revisited: Sepsis After Attempted Self-Induced Abortionmila nurmalaNo ratings yet
- Prevencion CesareaDocument19 pagesPrevencion CesareaNatalia MartínezNo ratings yet
- Khing Journal...Document5 pagesKhing Journal...Khing AbatNo ratings yet
- Caesarean Section at Full Dilatation: Incidence, Impact and Current ManagementDocument20 pagesCaesarean Section at Full Dilatation: Incidence, Impact and Current ManagementAbdur RaheemNo ratings yet
- Vaginal Birth After Caeserean Section: BY Seun ODocument24 pagesVaginal Birth After Caeserean Section: BY Seun OOlaiya OluwaseunNo ratings yet
- Article 262063-PrintDocument15 pagesArticle 262063-PrintAhsan AuliyaNo ratings yet
- Moxibustion To Correct A Breech Presentation of The Fetus Author IDEASSDocument13 pagesMoxibustion To Correct A Breech Presentation of The Fetus Author IDEASSVraciul din VeciniNo ratings yet
- Vesico-Vaginal Fistulas in Developing Countries: P.HiltonDocument11 pagesVesico-Vaginal Fistulas in Developing Countries: P.HiltonRakha Sulthan SalimNo ratings yet
- C Cection 8Document43 pagesC Cection 8blatchujosephNo ratings yet
- Jurnal Obgyn 2018 2Document15 pagesJurnal Obgyn 2018 2aulNo ratings yet
- 2015 Sep Embarazo Múltiple - Vía Del Parto.Document13 pages2015 Sep Embarazo Múltiple - Vía Del Parto.Alexander Gonzalez BarturenNo ratings yet
- Atypical Breast Proliferative Lesions and Benign Breast DiseaseFrom EverandAtypical Breast Proliferative Lesions and Benign Breast DiseaseFarin AmersiNo ratings yet
- Tabel Perhitungan McuaDocument8 pagesTabel Perhitungan McuacesaliapNo ratings yet
- Part IX: Vascular Surgery: Renal and Spinal Cord ProtectionDocument1 pagePart IX: Vascular Surgery: Renal and Spinal Cord ProtectioncesaliapNo ratings yet
- Diagnostic Management of The Clinically Localized Ovarian MassDocument1 pageDiagnostic Management of The Clinically Localized Ovarian MasscesaliapNo ratings yet
- Vertebral Arteries: Common Carotid, Internal Carotid, and External Carotid ArteriesDocument1 pageVertebral Arteries: Common Carotid, Internal Carotid, and External Carotid ArteriescesaliapNo ratings yet
- Generations of The Plug-and-Patch Repair: Its Development and Lessons From HistoryDocument1 pageGenerations of The Plug-and-Patch Repair: Its Development and Lessons From HistorycesaliapNo ratings yet
- Results of A Personal Series: Femoral VesselsDocument1 pageResults of A Personal Series: Femoral VesselscesaliapNo ratings yet
- Part VIII: Nongastrointestinal Transabdominal Surgery: Intraperitoneal Mesh RepairDocument1 pagePart VIII: Nongastrointestinal Transabdominal Surgery: Intraperitoneal Mesh RepaircesaliapNo ratings yet
- Been Abandoned in Favor of Hetero-/ortho-Topic Pouches.: Heterotopic Continent DiversionDocument1 pageBeen Abandoned in Favor of Hetero-/ortho-Topic Pouches.: Heterotopic Continent DiversioncesaliapNo ratings yet
- Chapter 193: Surgical Management of Ovarian Carcinoma: Sup. Rectal A. and VDocument1 pageChapter 193: Surgical Management of Ovarian Carcinoma: Sup. Rectal A. and VcesaliapNo ratings yet
- Part VIII: Nongastrointestinal Transabdominal SurgeryDocument1 pagePart VIII: Nongastrointestinal Transabdominal SurgerycesaliapNo ratings yet
- Cooper Ligament Repair of Groin Hernias: Robb H. RutledgeDocument1 pageCooper Ligament Repair of Groin Hernias: Robb H. RutledgecesaliapNo ratings yet
- Part VIII: Nongastrointestinal Transabdominal SurgeryDocument1 pagePart VIII: Nongastrointestinal Transabdominal SurgerycesaliapNo ratings yet
- Ileal Pouches: Chapter 189: Supravesical Urinary DiversionDocument1 pageIleal Pouches: Chapter 189: Supravesical Urinary DiversioncesaliapNo ratings yet
- Remove Them Within A Week. Mainz Neobladder: Chapter 189: Supravesical Urinary DiversionDocument1 pageRemove Them Within A Week. Mainz Neobladder: Chapter 189: Supravesical Urinary DiversioncesaliapNo ratings yet
- Page 2087Document1 pagePage 2087cesaliapNo ratings yet
- Page 2089Document1 pagePage 2089cesaliapNo ratings yet
- Supravesical Urinary Diversion: Badrinath Konety and Sean P. ElliottDocument1 pageSupravesical Urinary Diversion: Badrinath Konety and Sean P. ElliottcesaliapNo ratings yet
- Pencarian Bukti IlmiahDocument2 pagesPencarian Bukti IlmiahcesaliapNo ratings yet
- Cagayan de Oro CityDocument6 pagesCagayan de Oro CityRaymond AbejuelaNo ratings yet
- How Physical Education Contribute To Young People's Physical Activity Level?Document2 pagesHow Physical Education Contribute To Young People's Physical Activity Level?Jessica Alcala Dela TorreNo ratings yet
- English Research PaperDocument6 pagesEnglish Research Paperapi-390838152No ratings yet
- COVID-19-Return To Work-Workplace Hygiene PolicyDocument2 pagesCOVID-19-Return To Work-Workplace Hygiene PolicyNilamSanjeev Kumar SinghNo ratings yet
- Time Table FCCS OB 13 - 14 Maret SbyDocument4 pagesTime Table FCCS OB 13 - 14 Maret SbyLina SusantiNo ratings yet
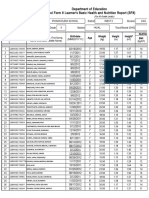
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Document4 pagesDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Roxan DosdosNo ratings yet
- Tribal Health in IndiaDocument14 pagesTribal Health in IndiaGautam G JNo ratings yet
- Sharfaa Ahmad Current ResumeDocument2 pagesSharfaa Ahmad Current Resumeapi-302596118No ratings yet
- Preparing Military Installations For Pandemic Infl Uenza Through Tabletop ExercisesDocument7 pagesPreparing Military Installations For Pandemic Infl Uenza Through Tabletop ExercisesEduardo Sousa SantosNo ratings yet
- Maternal Death Review: Need For Taking It UpDocument18 pagesMaternal Death Review: Need For Taking It UpPrabir Kumar ChatterjeeNo ratings yet
- RubelaDocument11 pagesRubelaMuhammad YusriNo ratings yet
- 2020 Article 363Document8 pages2020 Article 363RIAN NUGRAHANo ratings yet
- Task 11 EQUIPMENT MAINTENANCE SCHEDULEDocument1 pageTask 11 EQUIPMENT MAINTENANCE SCHEDULEMary Mel GarciaNo ratings yet
- Data Individu 1033017Document14 pagesData Individu 1033017Setyowati DwiNo ratings yet
- Criteria Donor of BloodDocument3 pagesCriteria Donor of Bloodapi-269388039No ratings yet
- Nurse Np1 Board CramsheetDocument8 pagesNurse Np1 Board CramsheetZero TwoNo ratings yet
- Infant and Young Child Feeding (IYCF) Practices in Udupi District, KarnatakaDocument7 pagesInfant and Young Child Feeding (IYCF) Practices in Udupi District, KarnatakaANna Laila Mardiana RNo ratings yet
- Neonatal SepsisDocument10 pagesNeonatal SepsisClaudelí GonzalezNo ratings yet
- Knowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalDocument4 pagesKnowledge and Practices of Nurses in Infection Prevention and Control Within A Tertiary Care HospitalAnonymous TzvMOnNo ratings yet
- Cermin Dunia Kedokteran, No 151. 2006. P: 14-17: Daftar PustakaDocument2 pagesCermin Dunia Kedokteran, No 151. 2006. P: 14-17: Daftar PustakaLaila Kurnia PramonoNo ratings yet
- Cosh CERT - FACILITATORDocument7 pagesCosh CERT - FACILITATORRedentor B. Rayla100% (1)
- Sex EducationDocument2 pagesSex EducationPatricia Bawiin †No ratings yet
- 11 - Recurrent UTI TOG 2020Document7 pages11 - Recurrent UTI TOG 2020Anna JuniedNo ratings yet
- ICD 10 CM Official Coding Gudance Interim Advice Coronavirus Feb 20 2020 PDFDocument3 pagesICD 10 CM Official Coding Gudance Interim Advice Coronavirus Feb 20 2020 PDFSumiwaty PanNo ratings yet
- Syndromic Management of STDsDocument13 pagesSyndromic Management of STDsMeenachi S100% (1)
- 15-17 - 7-PDF - Community Medicine With Recent Advances - 3 PDFDocument3 pages15-17 - 7-PDF - Community Medicine With Recent Advances - 3 PDFdwimahesaputraNo ratings yet
- Folder 10 BNAPDocument5 pagesFolder 10 BNAPRUDIRICK SIMBILINGNo ratings yet
- Hamilton County Infant Mortality RatesDocument3 pagesHamilton County Infant Mortality RatesWCPO 9 NewsNo ratings yet
- Standard Precautions 1Document34 pagesStandard Precautions 1Melody LandichoNo ratings yet