Download as pdf or txt
You might also like
- IV Compatibility ChartDocument6 pagesIV Compatibility ChartMae Quenie Abadingo Tiro75% (4)
- Reconstitution and Stability of IntravenousMedicationsDocument3 pagesReconstitution and Stability of IntravenousMedicationsbibowiwiNo ratings yet
- Epidemiology of Neonatal Sepsis and Associated Factors Implicated: Observational Study at Neonatal Intensive Care Unit of Arsi University Teaching and Referral Hospital, South East Ethiopia PDFDocument10 pagesEpidemiology of Neonatal Sepsis and Associated Factors Implicated: Observational Study at Neonatal Intensive Care Unit of Arsi University Teaching and Referral Hospital, South East Ethiopia PDFSultan Rahmat SeptianNo ratings yet
- Sepsis Proposal1Document34 pagesSepsis Proposal1Appiah Peter OforiNo ratings yet
- Predictors of Positive Blood Culture and Deaths Among Neonates With Suspected Neonatal Sepsis in A Tertiary Hospital, Mwanza-TanzaniaDocument9 pagesPredictors of Positive Blood Culture and Deaths Among Neonates With Suspected Neonatal Sepsis in A Tertiary Hospital, Mwanza-Tanzaniafasya azzahraNo ratings yet
- IJN - Volume 11 - Issue 1 - Pages 1-11Document11 pagesIJN - Volume 11 - Issue 1 - Pages 1-11janaina nogueiraNo ratings yet
- Dr. Vona 12Document5 pagesDr. Vona 12Agustiawan ImronNo ratings yet
- Bacterial AgentDocument10 pagesBacterial AgentDyah Ayu Puspita AnggarsariNo ratings yet
- Review Article: Choice and Duration of Antimicrobial Therapy For Neonatal Sepsis and MeningitisDocument10 pagesReview Article: Choice and Duration of Antimicrobial Therapy For Neonatal Sepsis and MeningitisjessicacookNo ratings yet
- Fcimb 11 694093Document12 pagesFcimb 11 694093Marketable StudioNo ratings yet
- Background Changing Patterns of Neonatal Fungal Sepsis in A Developing CountryDocument5 pagesBackground Changing Patterns of Neonatal Fungal Sepsis in A Developing CountryNada AhmedNo ratings yet
- Prognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyDocument6 pagesPrognostic of Sepsis in A Congolese Pediatric Emergency Service Using PSOFA Score A Prospective StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 33 Sneha EtalDocument7 pages33 Sneha EtaleditorijmrhsNo ratings yet
- Community-Acquired Pneumonia in Children: Myths and FactsDocument4 pagesCommunity-Acquired Pneumonia in Children: Myths and FactsFranciscoDelgadoNo ratings yet
- Legba Et Al., 2023Document11 pagesLegba Et Al., 2023victorien.dougnonNo ratings yet
- Determinants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyDocument8 pagesDeterminants of Neonatal Sepsis Among Neonates in The Northwest Part of Ethiopia: Case-Control StudyNaman KhalidNo ratings yet
- Comparative Study of Intestinal Parasitic Infection Among Pregnant and Non-Pregnant Women in Owerri, Nigeria A Case Study of The Federal Medical Centre, OwerriDocument6 pagesComparative Study of Intestinal Parasitic Infection Among Pregnant and Non-Pregnant Women in Owerri, Nigeria A Case Study of The Federal Medical Centre, OwerriEgbuna ChukwuebukaNo ratings yet
- Neonatal Sepsis in S Asia - A Huge Burden and Spiralling AMRDocument5 pagesNeonatal Sepsis in S Asia - A Huge Burden and Spiralling AMRdrdrNo ratings yet
- ANJ - Volume 3 - Issue 1 - Pages 85-106Document22 pagesANJ - Volume 3 - Issue 1 - Pages 85-106tri jayaningratNo ratings yet
- Neonatal Sepsis in The Very Low Birth Weight Preterm Infants: Part 1: Review of Patho-PhysiologyDocument10 pagesNeonatal Sepsis in The Very Low Birth Weight Preterm Infants: Part 1: Review of Patho-PhysiologyjukunkNo ratings yet
- Neonatal Sepsis: Haematological PerspectivesDocument6 pagesNeonatal Sepsis: Haematological PerspectivesPUBLISHER JOURNALNo ratings yet
- International Journal of Infectious DiseasesDocument9 pagesInternational Journal of Infectious DiseasesHope ChrisNo ratings yet
- Neonatal SepsisDocument11 pagesNeonatal SepsisrezkadehaNo ratings yet
- Journal Pmed 1003787Document20 pagesJournal Pmed 1003787GAYATHIRINo ratings yet
- Neumonia Por InfluenzaDocument19 pagesNeumonia Por InfluenzaEdgar GavilanesNo ratings yet
- IJP Volume 8 Issue 9 Pages 12011-12021Document11 pagesIJP Volume 8 Issue 9 Pages 12011-12021rullyNo ratings yet
- NEonatal Sepsis PDFDocument11 pagesNEonatal Sepsis PDFMarielaTessyGonzalesParedesNo ratings yet
- Typhoid Review pntd.0004785 PDFDocument16 pagesTyphoid Review pntd.0004785 PDFKhotibul maulanaNo ratings yet
- 9 JurnalDocument83 pages9 JurnalWanda AndiniNo ratings yet
- JPNC-10-00404Document7 pagesJPNC-10-00404Tomas YeheisNo ratings yet
- Annotated Bibliography Aasha TurnerDocument8 pagesAnnotated Bibliography Aasha Turnerapi-644326339No ratings yet
- 2016 Article 645Document10 pages2016 Article 645Betharia TriayuNo ratings yet
- Neonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollDocument9 pagesNeonatal Sepsis: Progress Towards Improved Outcomes: Andi L. Shane, Barbara J. StollMarco Antonio Mendoza OjedaNo ratings yet
- Neonatal Sepsis Literature ReviewDocument8 pagesNeonatal Sepsis Literature Reviewfvgczbcy100% (1)
- Ajol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204Document6 pagesAjol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204ASK De OliveiraNo ratings yet
- Acinetobacter Neonatal Infection. Mortality Associated Risk FactorsDocument8 pagesAcinetobacter Neonatal Infection. Mortality Associated Risk FactorsAli Faisal SaleemNo ratings yet
- 5BJPCBS201005.195D20Holanda20et - Al .2C202019 PDFDocument15 pages5BJPCBS201005.195D20Holanda20et - Al .2C202019 PDFputri vinia /ilove cuteNo ratings yet
- Bacteriological Profile of Neonatal Sepsis and Antibiotic Susceptibility Pattern of Isolates Admitted at Kanti Children's Hospital, Kathmandu, NepalDocument6 pagesBacteriological Profile of Neonatal Sepsis and Antibiotic Susceptibility Pattern of Isolates Admitted at Kanti Children's Hospital, Kathmandu, NepalPSIK sarimuliaNo ratings yet
- Journal Pone 0207095Document16 pagesJournal Pone 0207095Vivi SinulinggaNo ratings yet
- Epidemiologi of HFMDDocument16 pagesEpidemiologi of HFMDJimmy AmbaritaNo ratings yet
- Hookworm-Related Anaemia Among Pregnant Women: A Systematic ReviewDocument10 pagesHookworm-Related Anaemia Among Pregnant Women: A Systematic ReviewAjay DNo ratings yet
- MAKALAH Keputusasan-1Document7 pagesMAKALAH Keputusasan-1ARINANo ratings yet
- TurquiaDocument8 pagesTurquiaanselmopesquisa2769No ratings yet
- Epidemiology of Invasive Early Onset Neonatal SepsisDocument11 pagesEpidemiology of Invasive Early Onset Neonatal SepsisLucas SalgadoNo ratings yet
- Estudio de CorteDocument9 pagesEstudio de CorteblanquishemNo ratings yet
- Impact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDocument9 pagesImpact of Malaria at The End of Pregnancy On Infant Mortality and MorbidityDebby Astasya AnnisaNo ratings yet
- Neonatal Infections PerspectiveDocument13 pagesNeonatal Infections PerspectiveYUDY LORENA GIRALDO ALFONSONo ratings yet
- Protective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsDocument5 pagesProtective Effect of Breast Milk On Urinary Tract Infection in Children Aged 0-3 YearsChika FebrianiNo ratings yet
- Advances in Neonatal InfectionsDocument5 pagesAdvances in Neonatal InfectionsElizabeth HendersonNo ratings yet
- Efficacy and Safety of Fluconazole Prophylaxis in Extremely Low Birth Weight Infants: Multicenter Pre-Post Cohort StudyDocument10 pagesEfficacy and Safety of Fluconazole Prophylaxis in Extremely Low Birth Weight Infants: Multicenter Pre-Post Cohort StudyAnry UmarNo ratings yet
- Antibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenDocument5 pagesAntibiotic Resistance Patterns of Urinary Tract Pathogens in Turkish ChildrenLavfy NjlaaNo ratings yet
- Prevalence and Associated Risk Factors of Sepsis Among Neonates Admitted Into Neonatal Intensive Care Units of Public Hospitals in DhakaDocument12 pagesPrevalence and Associated Risk Factors of Sepsis Among Neonates Admitted Into Neonatal Intensive Care Units of Public Hospitals in DhakaAnonymous SMLzNANo ratings yet
- Biomarkers Pediatric TBDocument9 pagesBiomarkers Pediatric TBPaulo MattosNo ratings yet
- Artikel Rotaviruses FinalDocument30 pagesArtikel Rotaviruses Finalsemangat pagiNo ratings yet
- Hand, Foot and Mouth Disease: Spatiotemporal Transmission and ClimateDocument10 pagesHand, Foot and Mouth Disease: Spatiotemporal Transmission and ClimateAisah AisahNo ratings yet
- Acute Gastroenteritis Associated With Rotavirus A Among Children Less Than 5 Years of Age in NepalDocument8 pagesAcute Gastroenteritis Associated With Rotavirus A Among Children Less Than 5 Years of Age in NepalSanaNo ratings yet
- Journal Reading AnakDocument19 pagesJournal Reading AnakPutra Priambodo WibowoNo ratings yet
- Respiratory in PakDocument10 pagesRespiratory in PakEman ShNo ratings yet
- 90532100Document5 pages90532100Devi PuspasariNo ratings yet
- Neonatal Sepsis and Its Associated Factors Among Neonates Admitted To Neonatal Intensive Care Units in Primary Hospitals in Central Gondar Zone NorthDocument12 pagesNeonatal Sepsis and Its Associated Factors Among Neonates Admitted To Neonatal Intensive Care Units in Primary Hospitals in Central Gondar Zone NorthDrAli SalemNo ratings yet
- Obstetric Infections and Clinical Characteristics of Maternal Sepsis: A Hospital Based Retrospective Cohort StudyDocument12 pagesObstetric Infections and Clinical Characteristics of Maternal Sepsis: A Hospital Based Retrospective Cohort StudyblanquishemNo ratings yet
- The Biology of Fungi Impacting Human Health: A Tropical Asia-Pacific PerspectiveFrom EverandThe Biology of Fungi Impacting Human Health: A Tropical Asia-Pacific PerspectiveRating: 5 out of 5 stars5/5 (1)
- Feeding of Healthy Newborn: NF-1 Teaching Aids: NNFDocument32 pagesFeeding of Healthy Newborn: NF-1 Teaching Aids: NNFSahil DhamijaNo ratings yet
- A Neonate With Acute Kidney Injury: Case PresentationDocument4 pagesA Neonate With Acute Kidney Injury: Case PresentationSahil DhamijaNo ratings yet
- 14860Document3 pages14860Sahil DhamijaNo ratings yet
- WP 28278 2019 FinalOrder 24-Jan-2020 PDFDocument8 pagesWP 28278 2019 FinalOrder 24-Jan-2020 PDFSahil DhamijaNo ratings yet
- COVID 19 Pediatric Treatment ProtocolDocument1 pageCOVID 19 Pediatric Treatment ProtocolSahil DhamijaNo ratings yet
- Abdominal Pain PDFDocument23 pagesAbdominal Pain PDFSahil DhamijaNo ratings yet
- (15th June - 21st June) Weekly Webinars ScheduleDocument1 page(15th June - 21st June) Weekly Webinars ScheduleSahil DhamijaNo ratings yet
- 16240Document2 pages16240Sahil DhamijaNo ratings yet
- II. Write Notes On:: Q.P. Code: 161452Document3 pagesII. Write Notes On:: Q.P. Code: 161452Sahil DhamijaNo ratings yet
- EnteralDocument5 pagesEnteralSahil DhamijaNo ratings yet
- Approach To Short Stature (Autosaved)Document34 pagesApproach To Short Stature (Autosaved)Sahil Dhamija100% (1)
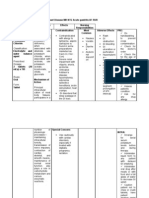
- Name of Drug Dosage and Route Indications Contra-Indications Side Effects Nursing ResponsibilitiesDocument7 pagesName of Drug Dosage and Route Indications Contra-Indications Side Effects Nursing ResponsibilitiesTon AgustinNo ratings yet
- Drug StudyDocument11 pagesDrug StudyKimberly Ann MendozaNo ratings yet
- Reconstitution, Stability and Sterility of Injectable DrugsDocument31 pagesReconstitution, Stability and Sterility of Injectable DrugsKevinNo ratings yet
- Cephalosporins Quick ReviewDocument19 pagesCephalosporins Quick ReviewErinson Custodio PlasenciaNo ratings yet
- Beta Lactam AntibioticsDocument1 pageBeta Lactam AntibioticsCourtney TownsendNo ratings yet
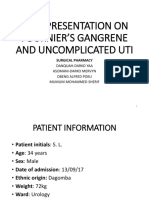
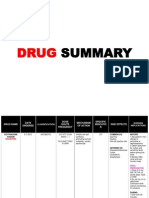
- Case Presentation On Fournier's GangreneDocument46 pagesCase Presentation On Fournier's GangreneYaa Danquah-Darko100% (1)
- Case Study GonorrheaDocument19 pagesCase Study GonorrheaErika ThereseNo ratings yet
- FDA Updates Guidance On Use of Ceftriaxone and CalciumDocument6 pagesFDA Updates Guidance On Use of Ceftriaxone and CalciumLathifaBidaraniNo ratings yet
- Guia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Document18 pagesGuia IDSA-Practice Guidelines For The Management of Bacterial Meningitis-2004Brenda Anali Pariona NapaNo ratings yet
- Paediatric Formulary16 and Final PDFDocument14 pagesPaediatric Formulary16 and Final PDFJenny WoodruffNo ratings yet
- Pharmacy Training Book 2022 YAQEEN SHQIRATDocument362 pagesPharmacy Training Book 2022 YAQEEN SHQIRATshafiqah hamdan100% (1)
- 1) Cephalosporins: Generation Common Dosages/Regimens Spectrum of Activity 1 Cephalexin (Keflex) 250-500mg PO q6hDocument1 page1) Cephalosporins: Generation Common Dosages/Regimens Spectrum of Activity 1 Cephalexin (Keflex) 250-500mg PO q6hjoe thomasNo ratings yet
- Update On Community-Acquired Bacterial Meningitis Guidance andDocument6 pagesUpdate On Community-Acquired Bacterial Meningitis Guidance andDaniel Martínez CruzNo ratings yet
- Medication Calculations 2Document26 pagesMedication Calculations 2loglesb1100% (2)
- Las 5Document26 pagesLas 5kateNo ratings yet
- DRUG STUDY: Rocephin - Ceftriaxone SodiumDocument1 pageDRUG STUDY: Rocephin - Ceftriaxone SodiumYum C100% (1)
- Pharm II Exam 1 - Abx I HintsDocument3 pagesPharm II Exam 1 - Abx I HintsNhung NguyenNo ratings yet
- DRUG STUDY CeftriaxoneDocument2 pagesDRUG STUDY CeftriaxoneBRYCE WILLIAM GONo ratings yet
- Drug of Choices PDFDocument10 pagesDrug of Choices PDFRavi Amin100% (1)
- CeftriaxoneDocument2 pagesCeftriaxoneFlora Angeli PastoresNo ratings yet
- Drug Study2Document8 pagesDrug Study2zbestgurlNo ratings yet
- Drug Study 2Document9 pagesDrug Study 2Justin PasaronNo ratings yet
- Intertrigo and Secondary Skin InfectionsDocument5 pagesIntertrigo and Secondary Skin Infectionskhalizamaulina100% (1)
- Feverish Illnessin ChildrenDocument310 pagesFeverish Illnessin Children1411731No ratings yet
- Ceftriaxone SodiumDocument3 pagesCeftriaxone SodiumjohannakatebellyNo ratings yet
- Mapping Disaster Research Ethics Scenarios: The Case StudiesDocument16 pagesMapping Disaster Research Ethics Scenarios: The Case StudiesBence KlusóczkiNo ratings yet
- Pharmacology Notes: EliminationDocument14 pagesPharmacology Notes: EliminationHaifa ibrahimNo ratings yet
- Meningitis Pediatrics in Review Dic 2015Document15 pagesMeningitis Pediatrics in Review Dic 2015Edwin VargasNo ratings yet