Download as xlsx, pdf, or txt
You might also like
- School Standard Family Reunification Release PlanDocument1 pageSchool Standard Family Reunification Release PlanJose Gabriel PesebreNo ratings yet
- Grade 5 GST Answer SheetDocument3 pagesGrade 5 GST Answer SheetEnajHaraf OrravanNo ratings yet
- Sample Template Summary of GradesDocument1 pageSample Template Summary of GradesKrizza Mae De LeonNo ratings yet
- School Reading Assessment ResultDocument15 pagesSchool Reading Assessment ResultRhinalyn A. BarberanNo ratings yet
- Deworming ChecklistDocument1 pageDeworming ChecklistJewela AlbaoNo ratings yet
- ReferralDocument2 pagesReferralMajie MaraveNo ratings yet
- Introduce YourselfDocument6 pagesIntroduce YourselfNur Nazihah HaninNo ratings yet
- Master List of EmployeesDocument1 pageMaster List of EmployeesGlenn L. Ravanilla0% (1)
- Study Monitoring SheetsmsDocument4 pagesStudy Monitoring SheetsmsJessa BilaranNo ratings yet
- Summer Registration 2021Document2 pagesSummer Registration 2021skineater4thewinNo ratings yet
- Department of Education Division of Cebu City Masterlist of LearnersDocument2 pagesDepartment of Education Division of Cebu City Masterlist of LearnersSri RodNo ratings yet
- Attendance Chart of Pupils, Sy 2018-2019Document2 pagesAttendance Chart of Pupils, Sy 2018-2019Ivy Lynn TanNo ratings yet
- Elimu Scholarship Application Form 22apr21Document6 pagesElimu Scholarship Application Form 22apr21Kipkoech FrankNo ratings yet
- ABC EnrollmentDocument1 pageABC Enrollmentrebs7No ratings yet
- Elementary SchoolDocument2 pagesElementary SchoolDaryna KovalevaNo ratings yet
- Student ProfileDocument4 pagesStudent ProfileJessica Ocay100% (1)
- Youth Resiliency Registration FormDocument1 pageYouth Resiliency Registration Formfirstroundfamily53No ratings yet
- Aspire Life Skills and Awareness SocietyDocument1 pageAspire Life Skills and Awareness SocietyRizwan AliNo ratings yet
- Player ProfileDocument2 pagesPlayer ProfileJeffersonCountyNo ratings yet
- Answer SheetDocument1 pageAnswer Sheetsardor.mirodilovNo ratings yet
- Student'S Information: Domingo Lacson National High SchoolDocument3 pagesStudent'S Information: Domingo Lacson National High SchoolAnit Eiram OcramNo ratings yet
- RF Attendance-Star TwinklersDocument4 pagesRF Attendance-Star TwinklersmarivicbantilanpiodenaNo ratings yet
- Grade 7 Examiner Recruitment FormDocument2 pagesGrade 7 Examiner Recruitment Formaddy100% (1)
- Study Monitoring Sheet: Mathematics DepartmentDocument3 pagesStudy Monitoring Sheet: Mathematics DepartmentMariel AdelNo ratings yet
- Student ECell Member Sign-Up Form Edited March 2011Document1 pageStudent ECell Member Sign-Up Form Edited March 2011nivedita_h42404No ratings yet
- Family Mapping FormDocument1 pageFamily Mapping FormHardy MisagalNo ratings yet
- INTAKE SHEET FormDocument3 pagesINTAKE SHEET FormKim MacadangdangNo ratings yet
- School Vision Screening Form: School: District: Section: MunicipalityDocument2 pagesSchool Vision Screening Form: School: District: Section: MunicipalityjofredmartinezNo ratings yet
- Equity Wings To Fly - Application Form 2021Document6 pagesEquity Wings To Fly - Application Form 2021frank kipkoechNo ratings yet
- Age-Profile (SMAW-11) 2022Document2 pagesAge-Profile (SMAW-11) 2022ISAGANINo ratings yet
- Admission Form SE TE BEDocument1 pageAdmission Form SE TE BEganeshcr7777No ratings yet
- Flag Ceremony Attendance SheetDocument1 pageFlag Ceremony Attendance SheetjaninadotolloNo ratings yet
- VIVA 15 Sports Registration Forms 2023Document13 pagesVIVA 15 Sports Registration Forms 2023SuमनNo ratings yet
- Aspire Quiz & Debating SocietyDocument1 pageAspire Quiz & Debating SocietyRizwan AliNo ratings yet
- VS Monitoring SheetDocument2 pagesVS Monitoring SheetbagangsbNo ratings yet
- 3UB7b9T-GeeiKF8N1RYKwSb1b rZJP0A9rpwJC65jitlLqYsFSWLKxoKy0WsnBBzxNAsOX46hrk2YtmLXJnZZj5KX R9kSzocs0cCMES-NCFDocument2 pages3UB7b9T-GeeiKF8N1RYKwSb1b rZJP0A9rpwJC65jitlLqYsFSWLKxoKy0WsnBBzxNAsOX46hrk2YtmLXJnZZj5KX R9kSzocs0cCMES-NCFAbhay BaruahNo ratings yet
- CV For Wildlife Watcher PostDocument1 pageCV For Wildlife Watcher PostIjaz Ul HaqNo ratings yet
- Home Visitation FormDocument1 pageHome Visitation FormMARY ANN COÑADONo ratings yet
- For-Clinic-Teachers (1) DentalDocument8 pagesFor-Clinic-Teachers (1) DentalMARITESS JUMAO-ASNo ratings yet
- Attendance SheetDocument4 pagesAttendance SheetChristian FrutoNo ratings yet
- Learner's DiaryDocument11 pagesLearner's DiaryFor JunkNo ratings yet
- Individual Learners Record LRDocument1 pageIndividual Learners Record LRKreativNo ratings yet
- Maryland School Inc.: Personal InformationDocument1 pageMaryland School Inc.: Personal InformationCalvin DelicanoNo ratings yet
- Distribution of School Based Feeding Program Food CommodityDocument13 pagesDistribution of School Based Feeding Program Food CommodityPhey Ayson OlleroNo ratings yet
- Choral Audition Form: Isabela State University Ilagan Campus Rhythmic Society ChoralDocument1 pageChoral Audition Form: Isabela State University Ilagan Campus Rhythmic Society Choralflorante26No ratings yet
- Pride and Prejudice Original FormDocument2 pagesPride and Prejudice Original FormAlexander SladeNo ratings yet
- Grade/Section: Individual Inventory FormDocument1 pageGrade/Section: Individual Inventory FormDada Baraniano PandaanNo ratings yet
- College Individual Inventory SheetDocument2 pagesCollege Individual Inventory SheetjonaxxisthequeenNo ratings yet
- 48th SSEAYP Application Form - PDFDocument4 pages48th SSEAYP Application Form - PDFLinea Rose L. SolomonNo ratings yet
- Confidential Guidance and Counseling Services 2X2 Colored PictureDocument2 pagesConfidential Guidance and Counseling Services 2X2 Colored PictureJOHN RULF OMAYANNo ratings yet
- Frequency of Error/Least Learned Skills: Item NoDocument9 pagesFrequency of Error/Least Learned Skills: Item NoRomeo Jr Pacheco OpenaNo ratings yet
- School Based Immunization: Recording Form 1: Masterlist of Grade 1 StudentsDocument14 pagesSchool Based Immunization: Recording Form 1: Masterlist of Grade 1 StudentsDennisEstrellosoAlbisoNo ratings yet
- Deworming Masterlist TemplateDocument1 pageDeworming Masterlist TemplateAda Mae GeraldeNo ratings yet
- Phil-IRI Group Screening Answer Sheet (ENGLISH) Grade 3Document5 pagesPhil-IRI Group Screening Answer Sheet (ENGLISH) Grade 3Darien Tayag AloroNo ratings yet
- Complete The Form Below With Your DetailsDocument1 pageComplete The Form Below With Your Detailscarina_chan_7No ratings yet
- Home Visitation (Checklist)Document1 pageHome Visitation (Checklist)KarlNo ratings yet
- More Minute Math Drills, Grades 3 - 6: Multiplication and DivisionFrom EverandMore Minute Math Drills, Grades 3 - 6: Multiplication and DivisionRating: 5 out of 5 stars5/5 (1)
- Aringin High School: Area of Concern Objectives Strategies Activities Persons Involved Resources Means of VerificationDocument2 pagesAringin High School: Area of Concern Objectives Strategies Activities Persons Involved Resources Means of VerificationAngie GunsNo ratings yet
- 11bepartment of Lebucatton: Llepubhc of Tbe BilippinesDocument14 pages11bepartment of Lebucatton: Llepubhc of Tbe BilippinesAngie GunsNo ratings yet
- Aringin High School: Swot AnalysisDocument2 pagesAringin High School: Swot AnalysisAngie Guns100% (2)
- Aringin High School: Individual Workweek PlanDocument3 pagesAringin High School: Individual Workweek PlanAngie GunsNo ratings yet
- Aringin High School Moncada, Tarlac Ipcrf E-Tool Part 4: Development PlansDocument2 pagesAringin High School Moncada, Tarlac Ipcrf E-Tool Part 4: Development PlansAngie GunsNo ratings yet
- Aringin High School: Individual Daily Log and Accomplishment ReportDocument2 pagesAringin High School: Individual Daily Log and Accomplishment ReportAngie GunsNo ratings yet
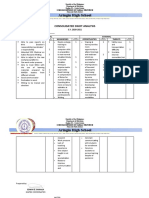
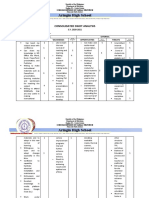
- Aringin High School: Consolidated Swot AnalysisDocument2 pagesAringin High School: Consolidated Swot AnalysisAngie GunsNo ratings yet
- San Roque National High School History Month & National Heroes Day CelebrationDocument12 pagesSan Roque National High School History Month & National Heroes Day CelebrationAngie GunsNo ratings yet
- Aringin High School: Actual Days of Attendance To Work Actual Time Log Actual Accomplishment/OutputDocument2 pagesAringin High School: Actual Days of Attendance To Work Actual Time Log Actual Accomplishment/OutputAngie GunsNo ratings yet
- Training MatrixDocument1 pageTraining MatrixAngie GunsNo ratings yet
- Aringin High School: Consolidated Swot AnalysisDocument3 pagesAringin High School: Consolidated Swot AnalysisAngie GunsNo ratings yet
- Aringin High School: Individual Workweek PlanDocument3 pagesAringin High School: Individual Workweek PlanAngie GunsNo ratings yet
- Aringin High School: Actual Days of Attendance Actual Accomplishments/ OutputDocument2 pagesAringin High School: Actual Days of Attendance Actual Accomplishments/ OutputAngie GunsNo ratings yet
- DTRDocument13 pagesDTRAngie GunsNo ratings yet
- AIS Consolidated Accomplishment Report 2017Document74 pagesAIS Consolidated Accomplishment Report 2017Angie GunsNo ratings yet
- KRADocument7 pagesKRAAngie GunsNo ratings yet
- Aringin High School: Curriculum Audit Plan Tool (Cap Tool) 1 Quarter Subject: Araling Panlipunan 10Document2 pagesAringin High School: Curriculum Audit Plan Tool (Cap Tool) 1 Quarter Subject: Araling Panlipunan 10Angie GunsNo ratings yet
- School Vision Screening Tally FormDocument1 pageSchool Vision Screening Tally FormAngie GunsNo ratings yet