Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Bomag BMP8500Service Manual Complete - WatermarkDocument300 pagesBomag BMP8500Service Manual Complete - WatermarkGiovanni Cacciamani100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tae Evo 015 - 351 EnglDocument39 pagesTae Evo 015 - 351 EnglMantenimientoValdezGutierrezNo ratings yet
- Seguimiento Post Parto de Hipertension Gravie 2022Document24 pagesSeguimiento Post Parto de Hipertension Gravie 2022Andrés Gaviria CNo ratings yet
- Isuog: GuidelinesDocument17 pagesIsuog: GuidelinesAndrés Gaviria CNo ratings yet
- Elite Athletes and Pregnancy Outcomes: A Systematic Review and Meta-AnalysisDocument31 pagesElite Athletes and Pregnancy Outcomes: A Systematic Review and Meta-AnalysisAndrés Gaviria CNo ratings yet
- Tablas Complementarias Art CovidDocument6 pagesTablas Complementarias Art CovidAndrés Gaviria CNo ratings yet
- Asociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Document8 pagesAsociacion Funcion Renal Materna y Resultados Embarazo DM 1 y 2.seah.2020Andrés Gaviria CNo ratings yet
- The Reduction of Melatonin Levels Is Associated With The Development of Preeclampsia: A Meta-AnalysisDocument9 pagesThe Reduction of Melatonin Levels Is Associated With The Development of Preeclampsia: A Meta-AnalysisAndrés Gaviria CNo ratings yet
- Guideline No. 402 Diagnosis and Management of Placenta PreviaDocument13 pagesGuideline No. 402 Diagnosis and Management of Placenta PreviaAndrés Gaviria C100% (1)
- Resolucion 2014565689.0Document8 pagesResolucion 2014565689.0Andrés Gaviria CNo ratings yet
- Theory of Chemical BondingDocument36 pagesTheory of Chemical BondingI Putu Adi Surya MahardikaNo ratings yet
- NetworkingDocument20 pagesNetworkingJaspreetSingh0% (1)
- Fatima 121 ThesisDocument144 pagesFatima 121 ThesisNecesario BanaagNo ratings yet
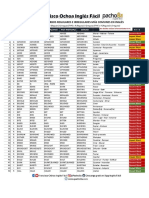
- Listado de Verbos Regulares E Irregulares Más Comunes en InglésDocument8 pagesListado de Verbos Regulares E Irregulares Más Comunes en InglésLogo DesingNo ratings yet
- Encyclopaedia of Popular Science (Steven N.shore)Document353 pagesEncyclopaedia of Popular Science (Steven N.shore)Muhammad Ali HaiderNo ratings yet
- 09 02ChapGereDocument12 pages09 02ChapGereAfoldo100% (1)
- Chemistry For Engineers 3Document34 pagesChemistry For Engineers 3Audrey VicenteNo ratings yet
- Chapter 17 - Transient Stability AnalysisDocument45 pagesChapter 17 - Transient Stability AnalysisPradeep_VashistNo ratings yet
- Be SRHDocument2 pagesBe SRHJanoNo ratings yet
- Chap016.ppt Materials Requirements PlanningDocument25 pagesChap016.ppt Materials Requirements PlanningSaad Khadur EilyesNo ratings yet
- 11 DeionizerDocument14 pages11 Deionizerfaiz faridNo ratings yet
- Science 3 TestDocument4 pagesScience 3 TestPatrick Jerome SilvanoNo ratings yet
- 02.06.2023 Actionable Points On TBM Commissioning and ExcavationDocument2 pages02.06.2023 Actionable Points On TBM Commissioning and ExcavationKiran KumarNo ratings yet
- Gillies Main MenuDocument2 pagesGillies Main MenugalgormNo ratings yet
- X-Cure WB90 PDFDocument2 pagesX-Cure WB90 PDFVirah Sammy ChandraNo ratings yet
- Food Fraud and Adulteration in ChinaDocument7 pagesFood Fraud and Adulteration in ChinaToroPolacoNo ratings yet
- Chiropractic: Name of Client Room Category Coverage ClientDocument6 pagesChiropractic: Name of Client Room Category Coverage ClientCh Raheel BhattiNo ratings yet
- Article 5Document10 pagesArticle 5frenlolmanNo ratings yet
- Argus Field Service Kit User Guide PDFDocument4 pagesArgus Field Service Kit User Guide PDFBeneDict Ben DNo ratings yet
- Zirconium and Zirconium Alloy Strip, Sheet, and Plate: Standard Specification ForDocument10 pagesZirconium and Zirconium Alloy Strip, Sheet, and Plate: Standard Specification ForTuanbk NguyenNo ratings yet
- Paradox Alarm - EVO Tech SheetDocument12 pagesParadox Alarm - EVO Tech SheetJulia MagnessNo ratings yet
- Electronics System Design Manufacturing ESDM May 2021Document35 pagesElectronics System Design Manufacturing ESDM May 2021wofedor973No ratings yet
- Fillet Welded JointsDocument4 pagesFillet Welded Jointsjocelyn beltranNo ratings yet
- Analysis and Modelling of CFT Members Moment Curvature AnalysisDocument10 pagesAnalysis and Modelling of CFT Members Moment Curvature AnalysisMahdi ValaeeNo ratings yet
- UsermanualDocument23 pagesUsermanualJagdish SinghNo ratings yet
- Quality Control of Ready Mixed Concrete Can Be Divided Into Three Convenient Areas LikeDocument11 pagesQuality Control of Ready Mixed Concrete Can Be Divided Into Three Convenient Areas Likeee iabNo ratings yet
- Sabrine Lure of The Expanse ExpansionDocument9 pagesSabrine Lure of The Expanse Expansionmalador99991% (11)
- MD (BD) - Lst-Cep-In-1001 Control System Io List Rev0 PDFDocument17 pagesMD (BD) - Lst-Cep-In-1001 Control System Io List Rev0 PDFKook PengNo ratings yet