Download as pdf or txt
You might also like
- Animal Bite Module 2021Document20 pagesAnimal Bite Module 2021ERMED OFC R2TMCNo ratings yet
- Honda CRV CR-V Radio Connector PinsDocument17 pagesHonda CRV CR-V Radio Connector Pinsdonald nugrahaNo ratings yet
- George Green - 01 - Handbook For The New ParadigmDocument188 pagesGeorge Green - 01 - Handbook For The New Paradigmtyjc87100% (5)
- A Clinical Nurse Specialist-Led Interprofessional Quality Improvement Project To Reduce Hospital-Acquired Pressure Ulcers Clinical Nurse SpecialistDocument7 pagesA Clinical Nurse Specialist-Led Interprofessional Quality Improvement Project To Reduce Hospital-Acquired Pressure Ulcers Clinical Nurse SpecialistIhsan Nur MahmudiNo ratings yet
- Newborn ScreeningDocument22 pagesNewborn ScreeningSirc PatrickNo ratings yet
- Animal Bite GuildlinesDocument7 pagesAnimal Bite GuildlinesHari Pawan Kishore GarimellaNo ratings yet
- Cpm12th RabiesDocument15 pagesCpm12th RabiesKaren ArchesNo ratings yet
- CHN - Rabies Control ProgramDocument16 pagesCHN - Rabies Control ProgramJoseph KentNo ratings yet
- Symptoms of RabiesDocument47 pagesSymptoms of RabiesJuri GallosNo ratings yet
- Policies On InfectionDocument7 pagesPolicies On InfectionLino Marcus ViolaNo ratings yet
- Commitment FormDocument6 pagesCommitment FormaringkinkingNo ratings yet
- Category Type of Exposure ManagementDocument10 pagesCategory Type of Exposure ManagementDianne GalangNo ratings yet
- Malaria Control Program: Printer-Friendly PDFDocument3 pagesMalaria Control Program: Printer-Friendly PDFdaryl ann dep-asNo ratings yet
- Critical Overview of Municipal Food Protection and Inspection PracticesDocument18 pagesCritical Overview of Municipal Food Protection and Inspection PracticesSagar ParajuliNo ratings yet
- Dead Bodies PDFDocument24 pagesDead Bodies PDFRj Concepcion RrtNo ratings yet
- DM No. 2020-0229 Revised Criteria For Discharge and Recovered For COVID-19 CasesDocument3 pagesDM No. 2020-0229 Revised Criteria For Discharge and Recovered For COVID-19 CasesNovelyn MalaluanNo ratings yet
- NIP2Document52 pagesNIP2Angela Joy AmparadoNo ratings yet
- Anti-Rabies ActDocument9 pagesAnti-Rabies ActL You Eleunor LucinoNo ratings yet
- What Is Rabies? How Do People and Animals Get The Disease?Document14 pagesWhat Is Rabies? How Do People and Animals Get The Disease?lea nicole iglesiasNo ratings yet
- Iloilo City Regulation Ordinance 2015-029Document4 pagesIloilo City Regulation Ordinance 2015-029Iloilo City Council100% (1)
- Guidelines RabiesDocument26 pagesGuidelines RabiesPriya Chetri100% (1)
- Ambu License Ao-2018-0001Document39 pagesAmbu License Ao-2018-0001Pdrrmo Planning100% (1)
- Policies & Procedures On Infection Prevention and ControlDocument308 pagesPolicies & Procedures On Infection Prevention and ControlHawthorn ANo ratings yet
- Topic 3 - Disease Control StrategiesDocument25 pagesTopic 3 - Disease Control StrategiesKaey NiezamNo ratings yet
- Epidemiological Perspective of Dengue - Sagar ParajuliDocument31 pagesEpidemiological Perspective of Dengue - Sagar ParajuliSagar ParajuliNo ratings yet
- Surveillance System in The PhilippinesDocument38 pagesSurveillance System in The PhilippinesFred C. MirandaNo ratings yet
- Expanded Program On ImmunizationDocument7 pagesExpanded Program On ImmunizationVanessa Abboud100% (1)
- GHS Reproductive Health Strategic Plan FINALDocument109 pagesGHS Reproductive Health Strategic Plan FINALNana Adwoa Animah100% (2)
- Epidemiological Perspective of Malaria - Sagar ParajuliDocument27 pagesEpidemiological Perspective of Malaria - Sagar ParajuliSagar Parajuli100% (1)
- dm2021 0327 Surge Response Plan For HFDocument11 pagesdm2021 0327 Surge Response Plan For HFMonica Lowinski100% (1)
- Proposed Ordinace - Birthing FacilityDocument44 pagesProposed Ordinace - Birthing FacilityRichard C. AmoguisNo ratings yet
- Malaria: Lyndon L. Lee Suy, MD, MPHDocument30 pagesMalaria: Lyndon L. Lee Suy, MD, MPHPurplesmilezNo ratings yet
- Complete Manual MOP - 20150323Document250 pagesComplete Manual MOP - 20150323Angkol TuyorNo ratings yet
- Coronavirus Disease 2019-Situation Report 51Document9 pagesCoronavirus Disease 2019-Situation Report 51CityNewsTorontoNo ratings yet
- MalariaDocument8 pagesMalariaJovelyn BucsitNo ratings yet
- At A Glance: The Philippine Health Care System: MedicinesDocument15 pagesAt A Glance: The Philippine Health Care System: MedicinesEdrea Aquino MendezNo ratings yet
- Immunization in Children: Mary Beth F. Tanco, MD, FPPS Active Consultant Institute of Pediatrics and Child HealthDocument92 pagesImmunization in Children: Mary Beth F. Tanco, MD, FPPS Active Consultant Institute of Pediatrics and Child HealthPolychase Magaoay100% (1)
- Guidelines On Medical Equipment Management in NigeriaDocument8 pagesGuidelines On Medical Equipment Management in NigeriaBALANo ratings yet
- Malaria 1. Who and How?: P. Falciparum P. VivaxDocument6 pagesMalaria 1. Who and How?: P. Falciparum P. VivaxAdriana del RioNo ratings yet
- Doh Community Health ProgramsDocument48 pagesDoh Community Health ProgramsHope CarenaNo ratings yet
- Policies-Tb Dots in The WorkplaceDocument5 pagesPolicies-Tb Dots in The WorkplaceAngelique ThomasNo ratings yet
- RA6675 - Generics Act of 1988Document5 pagesRA6675 - Generics Act of 1988rollaninisNo ratings yet
- Marikina RHU For ADB PDFDocument26 pagesMarikina RHU For ADB PDFKristine PresbiteroNo ratings yet
- 2StandardOperatingProceduresforHospitals PDFDocument62 pages2StandardOperatingProceduresforHospitals PDFJoseph JordanNo ratings yet
- Ra 8504Document6 pagesRa 8504Kaycee Daya-MagosNo ratings yet
- Basic Information RabiesDocument32 pagesBasic Information RabiesdrkhalidfcpsNo ratings yet
- National Rabies Prevention and Control Program: Printer-Friendly PDFDocument3 pagesNational Rabies Prevention and Control Program: Printer-Friendly PDFdaryl ann dep-asNo ratings yet
- Cavite Readiness Assessment Tools - HC-RHU-BHS - MR SIA 2023Document10 pagesCavite Readiness Assessment Tools - HC-RHU-BHS - MR SIA 2023Christean Val Bayani ValezaNo ratings yet
- Infection: BascisDocument66 pagesInfection: Bascistummalapalli venkateswara raoNo ratings yet
- Form 3 - HPV Masterlistingv Form - UECSDocument6 pagesForm 3 - HPV Masterlistingv Form - UECSJEROMENo ratings yet
- NVBDCP 2014Document53 pagesNVBDCP 2014Aditya NairNo ratings yet
- COMMUNICABLE AND NCDsDocument147 pagesCOMMUNICABLE AND NCDschristine gisembaNo ratings yet
- VRH History and Vission MissionDocument2 pagesVRH History and Vission MissiondellcyberNo ratings yet
- Tropical Med Int Health - 2009 - Mendis - From Malaria Control To Eradication The WHO PerspectiveDocument8 pagesTropical Med Int Health - 2009 - Mendis - From Malaria Control To Eradication The WHO PerspectiveDircia D'silvaNo ratings yet
- Doh Policies and GuidelinesDocument48 pagesDoh Policies and GuidelinesMigz Mendez100% (1)
- Guidelines South African Guidelines For The Prevention of Malaria 2017 Final - zp135472Document43 pagesGuidelines South African Guidelines For The Prevention of Malaria 2017 Final - zp135472Sudhakar Kuppireddy100% (1)
- Malaria: Key FactsDocument7 pagesMalaria: Key FactseenNo ratings yet
- Animal Bite Traetment CenterDocument5 pagesAnimal Bite Traetment CenterPaul Cenabre100% (1)
- VaccinationDocument28 pagesVaccinationM AQIB ASLAMNo ratings yet
- Chapter 4 Notes HIV LawsDocument20 pagesChapter 4 Notes HIV LawsjvlarragaNo ratings yet
- Interim Guideline For Prevention and Control of Human Rabies in Malaysia PDFDocument17 pagesInterim Guideline For Prevention and Control of Human Rabies in Malaysia PDFvcweeNo ratings yet
- AO RabiesDocument21 pagesAO RabiesChristopher Owen T. JOCSONNo ratings yet
- Management of Animal Bite PatientsDocument26 pagesManagement of Animal Bite PatientsMary Grace Ogatis0% (1)
- What You Need To Know InfographicDocument1 pageWhat You Need To Know InfographicBitcoDavidNo ratings yet
- Faircrete SB (L)Document2 pagesFaircrete SB (L)Binoy Sankar SarkerNo ratings yet
- Chatrapati Shivaji TurminusDocument6 pagesChatrapati Shivaji TurminusshrutiNo ratings yet
- Tutorial 1Document3 pagesTutorial 1Chong Cherng WongNo ratings yet
- Garden City University College: Department of I.C.TDocument3 pagesGarden City University College: Department of I.C.Trichardmawuli3593No ratings yet
- Lesson Plan For DramaDocument6 pagesLesson Plan For DramaMerve MutluNo ratings yet
- COMESADocument15 pagesCOMESAchesca macaraigNo ratings yet
- Idol Remote Instruction For Copying Face To Face - Product NumberDocument3 pagesIdol Remote Instruction For Copying Face To Face - Product NumberMarcNo ratings yet
- AL6061 SiCDocument36 pagesAL6061 SiCmayankNo ratings yet
- LeafletsDocument2 pagesLeafletsAmir FarajiNo ratings yet
- Resume - Alexis GibsonDocument1 pageResume - Alexis Gibsonapi-521009603No ratings yet
- Chapter 1Document10 pagesChapter 1Pranjal jainNo ratings yet
- Oops QuesBankDocument20 pagesOops QuesBanksantoshsugur628No ratings yet
- Donald Redford - Akhenaten - New Theories and Old FactsDocument27 pagesDonald Redford - Akhenaten - New Theories and Old FactsDjatmiko TanuwidjojoNo ratings yet
- Botanical Inks Plant-to-Print DyesDocument276 pagesBotanical Inks Plant-to-Print DyesNoémi Gyimóthy100% (3)
- PT Foundations-1Document5 pagesPT Foundations-1YNNo ratings yet
- Branches of Forensic ScienceDocument19 pagesBranches of Forensic ScienceSriram ShirkeNo ratings yet
- DRRR Module 8 Concept of Disaster Risk Reduction and ManagementDocument22 pagesDRRR Module 8 Concept of Disaster Risk Reduction and ManagementJodie CabreraNo ratings yet
- BiochipDocument11 pagesBiochipnaani_sNo ratings yet
- Show Me The WayDocument1 pageShow Me The WayEdison EvangelistaNo ratings yet
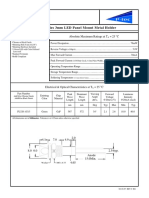
- PL320 Series 3mm LED Panel Mount Metal Holder: Features Absolute Maximum Ratings at T 25 °CDocument1 pagePL320 Series 3mm LED Panel Mount Metal Holder: Features Absolute Maximum Ratings at T 25 °CJajang JajaNo ratings yet
- The Complete Poetry and Prose of William BlakeDocument855 pagesThe Complete Poetry and Prose of William BlakeNey Alencar67% (3)
- Fig. 4. X-Ray Diffraction Pattern of Bio-SynthesizedDocument3 pagesFig. 4. X-Ray Diffraction Pattern of Bio-SynthesizedAfrah MNo ratings yet
- Slide Presentation For Literature ReviewDocument8 pagesSlide Presentation For Literature Reviewfvg7vpte100% (1)
- Butts Spatial DiDDocument35 pagesButts Spatial DiDpvaibhyNo ratings yet
- Gurukul Hindi e Book by Sirhud KalraDocument17 pagesGurukul Hindi e Book by Sirhud KalraPARVANo ratings yet
- Ale Cop CatalogDocument244 pagesAle Cop CatalogabyzenNo ratings yet