Download as pdf or txt
You might also like
- Cheatsheet 2Document1 pageCheatsheet 2Rick Frea86% (7)
- Vector - and Rodent-Borne Diseases in Europe and North America 2gfshDocument411 pagesVector - and Rodent-Borne Diseases in Europe and North America 2gfshRhyan ArfanNo ratings yet
- Anesthesiology Resident Manual of Procedures: A Step-by-Step GuideFrom EverandAnesthesiology Resident Manual of Procedures: A Step-by-Step GuideNo ratings yet
- RFH COVID-19 ICU Resource Pack FULL PDFDocument15 pagesRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNo ratings yet
- ACLSDocument17 pagesACLSms_lezah100% (4)
- Case Study PDFDocument57 pagesCase Study PDFShivanand Pegu100% (1)
- Ards Asmic 2018Document65 pagesArds Asmic 2018أسعد حسنانNo ratings yet
- ARDS Management Protocol: February 2018Document6 pagesARDS Management Protocol: February 2018soulstakers100% (1)
- Evidence Based Mechanical Ventilation Strategies ARS-Cortes-PuentesDocument23 pagesEvidence Based Mechanical Ventilation Strategies ARS-Cortes-PuentesAli AftabNo ratings yet
- Wevent Respiratory Management ProtocolDocument16 pagesWevent Respiratory Management ProtocolScribdTranslationsNo ratings yet
- Overview of Respiratory Failure & Use of Mechanical VentilationDocument89 pagesOverview of Respiratory Failure & Use of Mechanical VentilationsheharyarNo ratings yet
- COVIDDocument23 pagesCOVID24 Narong ReedNo ratings yet
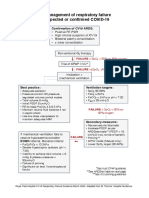
- ICU Management of Respiratory Failure in Suspected or Confirmed COVID-19Document2 pagesICU Management of Respiratory Failure in Suspected or Confirmed COVID-19Quique GarciaNo ratings yet
- Peds Clinical Cases (Egypt) 3-09 (Final Version)Document57 pagesPeds Clinical Cases (Egypt) 3-09 (Final Version)asupicuNo ratings yet
- 4-6 MV For ARDS (Basic Level)Document49 pages4-6 MV For ARDS (Basic Level)salwafathiNo ratings yet
- Ventilators For People Who Don'T Like ThemDocument14 pagesVentilators For People Who Don'T Like ThemJuanNo ratings yet
- Recomendations WeVent-6 PDFDocument16 pagesRecomendations WeVent-6 PDFJavier Enrique Barrera PachecoNo ratings yet
- COVID-19 Management of Critical Care Cases PDFDocument6 pagesCOVID-19 Management of Critical Care Cases PDFLubna AliNo ratings yet
- Contoh Kasus-Dr - TunjungDocument22 pagesContoh Kasus-Dr - TunjungYas EliasNo ratings yet
- Dead Space Analysis at Different Levels of Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome Patients. JCC 2018Document8 pagesDead Space Analysis at Different Levels of Positive End-Expiratory Pressure in Acute Respiratory Distress Syndrome Patients. JCC 2018Emiliano GogniatNo ratings yet
- Suspected or Confirmed Covid-19: Spo 92% Despite NRBM Urgent CRT Review WardDocument1 pageSuspected or Confirmed Covid-19: Spo 92% Despite NRBM Urgent CRT Review WardHAMMYER ALROKHAMINo ratings yet
- Weaning ProtocolDocument6 pagesWeaning ProtocolerwanNo ratings yet
- NPPVDocument29 pagesNPPVStephanie SusavageNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- Lecture Anwar Ventilation Managment COVIDDocument28 pagesLecture Anwar Ventilation Managment COVIDمحمدرزازالتبعيNo ratings yet
- Appendix 4b - NIV Algorithm (ICHT)Document1 pageAppendix 4b - NIV Algorithm (ICHT)Josi JeremiaNo ratings yet
- Advances and Alternatives in Respiratory Care DesktopDocument48 pagesAdvances and Alternatives in Respiratory Care DesktopAlex ChiuNo ratings yet
- 76 AcutePB840PAVPlusMgmtProtocolSS10VE5543 1316719265 PDFDocument2 pages76 AcutePB840PAVPlusMgmtProtocolSS10VE5543 1316719265 PDFNATHALIA MORENO PERILLANo ratings yet
- CRT Exam Review Guide Chapter 12Document29 pagesCRT Exam Review Guide Chapter 12Dharlyn MungcalNo ratings yet
- Bivent PittsDocument63 pagesBivent PittsFarook BaigNo ratings yet
- Mechanical Ventilation: Marc Charles ParentDocument53 pagesMechanical Ventilation: Marc Charles ParentarckelcNo ratings yet
- Basic Pediatric Ventilation: A 10 Slide Production by James Rubino USAF RTDocument10 pagesBasic Pediatric Ventilation: A 10 Slide Production by James Rubino USAF RTjcrubinoNo ratings yet
- NIPPVDocument23 pagesNIPPVFrances BituinNo ratings yet
- Protocolo LOVDocument6 pagesProtocolo LOVV ANo ratings yet
- Managing A Mechanically Ventilated PatientDocument51 pagesManaging A Mechanically Ventilated PatientPeony03No ratings yet
- Covid-19 Respiratory Failure Guide 112020.1Document2 pagesCovid-19 Respiratory Failure Guide 112020.1Anna JuniedNo ratings yet
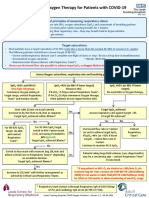
- Guidance On Oxygen Therapy For Patients With COVID-19: General Principles of Assessing Respiratory StatusDocument1 pageGuidance On Oxygen Therapy For Patients With COVID-19: General Principles of Assessing Respiratory StatusAsh mohamedNo ratings yet
- Kerry GomesDocument23 pagesKerry GomesAbegail IbañezNo ratings yet
- Anaesthetics NotesDocument15 pagesAnaesthetics NotesnaNo ratings yet
- Critical Event Checklists PDFDocument27 pagesCritical Event Checklists PDFMateas ZsoltNo ratings yet
- Potential Conflicts of InterestDocument8 pagesPotential Conflicts of InterestLina GuerraNo ratings yet
- Ards Pocket Card 4.7 QRDocument1 pageArds Pocket Card 4.7 QRGenghis SupnetNo ratings yet
- NIV ProformaDocument10 pagesNIV ProformaWael N Sh GadallaNo ratings yet
- Management of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Document7 pagesManagement of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Abhishek GoelNo ratings yet
- Practical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingDocument24 pagesPractical Considerations and Management of Multi-Organ Failure of in Pre-ICU SettingyusNo ratings yet
- CRT Exam Review Guide Chapter 15Document27 pagesCRT Exam Review Guide Chapter 15Dharlyn MungcalNo ratings yet
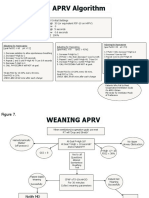
- APRV ModeqDocument19 pagesAPRV Modeqdr.rrajesh92No ratings yet
- Mechanical Ventilatory Support Series: Weaning & Liberation From Mechanical VentilationDocument41 pagesMechanical Ventilatory Support Series: Weaning & Liberation From Mechanical VentilationWasuchon ChaichanNo ratings yet
- Nippv Revisi Final Picu Nicu MaretDocument51 pagesNippv Revisi Final Picu Nicu MaretJulian Ammar Zaidan GunawanNo ratings yet
- ARDSnet Protocols PDFDocument2 pagesARDSnet Protocols PDFvbfisioNo ratings yet
- PPP Reading Test 11 Part A TextsDocument4 pagesPPP Reading Test 11 Part A TextsDaniah Marwan Dawood DAWOODNo ratings yet
- Respiratory Management Protocol of Patients With Sars-Cov-2 (COVID-19)Document17 pagesRespiratory Management Protocol of Patients With Sars-Cov-2 (COVID-19)Gastón MendozaNo ratings yet
- Aprv DiagramDocument2 pagesAprv DiagramMaine AsuncionNo ratings yet
- Medical Scenario 1Document42 pagesMedical Scenario 1murphy 1087No ratings yet
- UK - BTS - Respiratory Support of Patients On Medical WardsDocument5 pagesUK - BTS - Respiratory Support of Patients On Medical WardsAlexRázuriNo ratings yet
- Comprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference TipsDocument3 pagesComprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference Tipshyukkie minnieNo ratings yet
- Covid 19 Ventilator and Critical Care ManagementDocument41 pagesCovid 19 Ventilator and Critical Care ManagementFasil kariNo ratings yet
- Respiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsFrom EverandRespiratory Monitoring in Mechanical Ventilation: Techniques and ApplicationsJian-Xin ZhouNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- The Effects of Counterpressure Massage in Reducing Labor Pain in Mother Maternity Firs Stage Systematic Literature ReviewDocument2 pagesThe Effects of Counterpressure Massage in Reducing Labor Pain in Mother Maternity Firs Stage Systematic Literature ReviewNabila SyafirahNo ratings yet
- 2.02 - Quality and Bioequivalence Guideline - Jul19 - v7 1Document35 pages2.02 - Quality and Bioequivalence Guideline - Jul19 - v7 1vinayNo ratings yet
- Author (Year) 2014 Title: Alian, Sitti Alrana SDocument8 pagesAuthor (Year) 2014 Title: Alian, Sitti Alrana SErcel ArellanoNo ratings yet
- Drug Study On CloxacillinDocument2 pagesDrug Study On CloxacillinRoanne LaguaNo ratings yet
- Common Worm Infestations in Children: DR Nishant Verma Department of PediatricsDocument25 pagesCommon Worm Infestations in Children: DR Nishant Verma Department of PediatricsJosephine TungoeNo ratings yet
- Preoperative Anxiety and Its Associated Factors Among Surgical Patients in MalaysiaDocument6 pagesPreoperative Anxiety and Its Associated Factors Among Surgical Patients in MalaysiaVel MuruganNo ratings yet
- Holistic DentistryDocument13 pagesHolistic DentistrydnybellNo ratings yet
- MedDRA Coding in Pharmacovigilance PDFDocument42 pagesMedDRA Coding in Pharmacovigilance PDFDr Monika24No ratings yet
- EASL HepBDocument42 pagesEASL HepBmutiara dewiNo ratings yet
- "May Mga Sugat Ako.": As Verbalized by The PatientDocument6 pages"May Mga Sugat Ako.": As Verbalized by The Patientedifier_moonNo ratings yet
- (6-22) DR Takele ManuscriptDocument17 pages(6-22) DR Takele Manuscriptchernet bekeleNo ratings yet
- Infection Control Committee: Date: June 11, 2020 TO: Federico N. Eleazar, MDDocument1 pageInfection Control Committee: Date: June 11, 2020 TO: Federico N. Eleazar, MDCris GalendezNo ratings yet
- Modeling Infectious Diseases in Humans and Animals: BookreviewsDocument3 pagesModeling Infectious Diseases in Humans and Animals: BookreviewsMORA CUEVAS NICOLE EDITHNo ratings yet
- New York Office of Children and Family Services Maximus Training Plan 2004 - TBDDocument6 pagesNew York Office of Children and Family Services Maximus Training Plan 2004 - TBDBeverly TranNo ratings yet
- Community Acquired Pneumonia - AdultDocument13 pagesCommunity Acquired Pneumonia - Adultmits98No ratings yet
- MicrobiologyDocument6 pagesMicrobiologynoreplyneet46No ratings yet
- Nurses in Implementation of National Rural Health Mission: Dr. Pratima Mittra Sr. Consultant, RCH - Ii / NRHM NihfwDocument32 pagesNurses in Implementation of National Rural Health Mission: Dr. Pratima Mittra Sr. Consultant, RCH - Ii / NRHM NihfwPabhat KumarNo ratings yet
- The Who Surgical ChecklistDocument8 pagesThe Who Surgical ChecklistKaren SánchezNo ratings yet
- Ficha Tecnica Gelificante PDFDocument1 pageFicha Tecnica Gelificante PDFHarold EscobarNo ratings yet
- Pertanyaan JurnalDocument4 pagesPertanyaan JurnalgithaastarikaNo ratings yet
- MRI Safety Checklist English 032220Document1 pageMRI Safety Checklist English 032220phucNo ratings yet
- Laporan Eling PKM Pandean Juni 2022-Feb 2023Document321 pagesLaporan Eling PKM Pandean Juni 2022-Feb 2023ayuviantoroNo ratings yet
- Sudden Cardiac ArrestDocument20 pagesSudden Cardiac ArrestwindaNo ratings yet
- Legal and Ethical IssuesDocument22 pagesLegal and Ethical IssuesUdaya Sree100% (4)
- BenlystaDocument21 pagesBenlystaChrisNo ratings yet
- GEHA Connection Dental Federal: A National Dental PPO PlanDocument60 pagesGEHA Connection Dental Federal: A National Dental PPO PlanErdeli StefaniaNo ratings yet
- Clinical Teaching ON Geriatric AssessmentDocument9 pagesClinical Teaching ON Geriatric AssessmentANITTA SNo ratings yet
- Health Technology ManagementDocument26 pagesHealth Technology Managementhaseeb JuttNo ratings yet