Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Disease Detectives NotesDocument5 pagesDisease Detectives NotesErica Weng0% (1)
- Fppe Focused EvaluationDocument1 pageFppe Focused EvaluationLOVI KRISSADINo ratings yet
- Gastric CancerDocument25 pagesGastric CancerAndreea SubcinschiNo ratings yet
- Ramsay Sedation Scale and How To Use ItDocument10 pagesRamsay Sedation Scale and How To Use ItAdinda Putra PradhanaNo ratings yet
- Glanders in HorseDocument43 pagesGlanders in HorseWerner AlbuquerqueNo ratings yet
- Yoshida - EVAPORATION OF WATER IN HUMID AIRDocument8 pagesYoshida - EVAPORATION OF WATER IN HUMID AIRMoody MoodyNo ratings yet
- Evaporation of Water Into A Laminar Air and Superheated Steam Stream ofDocument8 pagesEvaporation of Water Into A Laminar Air and Superheated Steam Stream ofMoody MoodyNo ratings yet
- Fadail e Hajj-Pdfbooksfree - PK PDFDocument266 pagesFadail e Hajj-Pdfbooksfree - PK PDFMoody MoodyNo ratings yet
- TRG Program SPR 2022 Final 4 2 22Document7 pagesTRG Program SPR 2022 Final 4 2 22Moody MoodyNo ratings yet
- Wall Mounted Split Type Air Conditioner: ManualDocument8 pagesWall Mounted Split Type Air Conditioner: ManualMoody MoodyNo ratings yet
- Questionnaire Survey of Working Relationships Between Nurses and Doctors in University Teaching Hospitals in Southern NigeriaDocument22 pagesQuestionnaire Survey of Working Relationships Between Nurses and Doctors in University Teaching Hospitals in Southern NigeriaMin MinNo ratings yet
- History of Spine InstrumentationDocument35 pagesHistory of Spine InstrumentationSyarifNo ratings yet
- Journal Reading OrtopedDocument14 pagesJournal Reading OrtopedSarrah Kusuma DewiNo ratings yet
- Health Screening ChecklistDocument1 pageHealth Screening ChecklistRominaPulvermüllerSalvatierraNo ratings yet
- Myocardial Infarction With ST Segment ElevationDocument27 pagesMyocardial Infarction With ST Segment ElevationRika Yulizah GobelNo ratings yet
- Electro Cardiograph yDocument215 pagesElectro Cardiograph yToufique KaziNo ratings yet
- Ultrasound Evaluation of Abnormal Ovarian Cysts and Solid MassesDocument43 pagesUltrasound Evaluation of Abnormal Ovarian Cysts and Solid MassesibmreadywriterNo ratings yet
- A Case of Patient AI, Who Came in Due To Sore ThroatDocument16 pagesA Case of Patient AI, Who Came in Due To Sore ThroatLovelle LopezNo ratings yet
- XS-1000 Automated Hematology Analyzer: Small Footprint. Big DifferenceDocument4 pagesXS-1000 Automated Hematology Analyzer: Small Footprint. Big Differencerizal_aspanNo ratings yet
- PHICS 29th Annual Convention InvitationDocument7 pagesPHICS 29th Annual Convention InvitationsomarjnovagenNo ratings yet
- Gonioscopy Focal PointsDocument16 pagesGonioscopy Focal PointsRamesh BabuNo ratings yet
- ETT SUCTION DEWASA ACI14 - Suction - 2-2 PDFDocument46 pagesETT SUCTION DEWASA ACI14 - Suction - 2-2 PDFAde Rahmah YuliaNo ratings yet
- PPT Referat ADHD - Kevin LukitoDocument22 pagesPPT Referat ADHD - Kevin LukitonoviaNo ratings yet
- Thyroid Disease Anesthetic ConsiderationsDocument30 pagesThyroid Disease Anesthetic ConsiderationsmirzaoctaNo ratings yet
- Braun Neurology Endoscope SystemDocument132 pagesBraun Neurology Endoscope SystemMārcis RancānsNo ratings yet
- J Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeDocument7 pagesJ Esthet Restor Dent - 2020 - Vargas - A Systematic Approach To Contouring and Polishing Anterior Resin CompositeScarleth Stephania Perez CastilloNo ratings yet
- Amputee Physiotherapy Assessment FormDocument8 pagesAmputee Physiotherapy Assessment FormHari25885100% (1)
- Jurnal Farmakokinetik Dan Farmakodinamik Polimiksin BDocument11 pagesJurnal Farmakokinetik Dan Farmakodinamik Polimiksin BWildan Setyo RayandiNo ratings yet
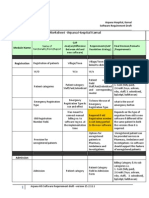
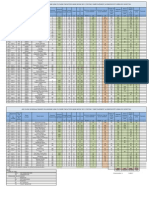
- Finalized Requirements-Worksheet - Arpana Hospital KarnalDocument11 pagesFinalized Requirements-Worksheet - Arpana Hospital KarnalMahesh PatilNo ratings yet
- PHYSIOTHERAPY BELLS PALSY (Dr.L.RAMADASS - PT 9500333960)Document62 pagesPHYSIOTHERAPY BELLS PALSY (Dr.L.RAMADASS - PT 9500333960)Ram DeekshaNo ratings yet
- Presentation2 BREAST IMAGING - LatestDocument53 pagesPresentation2 BREAST IMAGING - LatestLadipo Temitope AyodejiNo ratings yet
- The RADICAL Framework For Implementing and Monitoring Healthcare Risk ManagementDocument11 pagesThe RADICAL Framework For Implementing and Monitoring Healthcare Risk ManagementRangga PradanaNo ratings yet
- Drug StudyDocument4 pagesDrug Studysuperhuman_mabz100% (2)
- Load Estimate For Ahu-7Document4 pagesLoad Estimate For Ahu-7khaledmiNo ratings yet
- Impaired Urinary EliminationDocument3 pagesImpaired Urinary EliminationDenise Republika100% (1)