Download as pdf or txt
You might also like
- Governor's Study Group On Efficiency in State GovernmentDocument12 pagesGovernor's Study Group On Efficiency in State GovernmentMike Cason67% (3)
- Burton v. Regenass Complaint San DiegoDocument27 pagesBurton v. Regenass Complaint San DiegoFuzzy PandaNo ratings yet
- Genius 20 en Ver 1.2Document307 pagesGenius 20 en Ver 1.2Kristoffer BarkmanNo ratings yet
- Oversight Letter To AmeriCorpsDocument4 pagesOversight Letter To AmeriCorpsNick PopeNo ratings yet
- State House Facility Condition AssessmentDocument186 pagesState House Facility Condition AssessmentMike CasonNo ratings yet
- Steve Marshall V Ethics Commission ComplaintDocument17 pagesSteve Marshall V Ethics Commission ComplaintMike CasonNo ratings yet
- Final Summary Judgment OrderDocument20 pagesFinal Summary Judgment OrderinforumdocsNo ratings yet
- Genpharindictment 1Document22 pagesGenpharindictment 1jshpetriNo ratings yet
- LetterDocument5 pagesLetterChristina GiardinelliNo ratings yet
- Transcript of Audio Recording Between Attorney General and Gaming Control Board ChairmanDocument17 pagesTranscript of Audio Recording Between Attorney General and Gaming Control Board ChairmanMegan MesserlyNo ratings yet
- Nordberg MP Series Cone Crusher: Reference ManualDocument91 pagesNordberg MP Series Cone Crusher: Reference ManualJOSE CARRASCONo ratings yet
- Nova Prime ES Basic IFU PN57308A PDFDocument109 pagesNova Prime ES Basic IFU PN57308A PDFArmando AguilarNo ratings yet
- Tracie Todd Complaint From JICDocument144 pagesTracie Todd Complaint From JICMike CasonNo ratings yet
- Alabama Infant Mortality Report 2021Document31 pagesAlabama Infant Mortality Report 2021Mike CasonNo ratings yet
- AGB ReportDocument35 pagesAGB ReportThe State NewspaperNo ratings yet
- Morning Reception With Paul Ryan and The Republican Team For Romney Victory Inc.Document2 pagesMorning Reception With Paul Ryan and The Republican Team For Romney Victory Inc.Sunlight FoundationNo ratings yet
- Paxton V YelpDocument28 pagesPaxton V YelpChristopher HuttonNo ratings yet
- The Exclusive Spectrum News/Ipsos PollDocument11 pagesThe Exclusive Spectrum News/Ipsos PollDebbie HarbsmeierNo ratings yet
- Report On Riverside County Coroner's OfficeDocument15 pagesReport On Riverside County Coroner's OfficeThe Press-Enterprise / pressenterprise.comNo ratings yet
- Concurrent Authority Legislative Report Concurrent On Authority Regulating Farmed White-Tailed DeerDocument17 pagesConcurrent Authority Legislative Report Concurrent On Authority Regulating Farmed White-Tailed DeerSally Jo SorensenNo ratings yet
- Child Care in South Dakota ReportDocument8 pagesChild Care in South Dakota ReportErik KaufmanNo ratings yet
- Mississippi School Districts Currently Under Desegregation OrdersDocument2 pagesMississippi School Districts Currently Under Desegregation OrdersRuss LatinoNo ratings yet
- Lawsuit Against Val Verde District, PoliceDocument19 pagesLawsuit Against Val Verde District, PoliceThe Press-Enterprise / pressenterprise.comNo ratings yet
- Concrete Busters V Heebe, Ward, River Birch: Petition For DamagesDocument28 pagesConcrete Busters V Heebe, Ward, River Birch: Petition For DamagesnowdoucitNo ratings yet
- Press Contact Policy EmailsDocument3 pagesPress Contact Policy EmailsWXMINo ratings yet
- NAGR v. Naperville - State of Illinois LetterDocument3 pagesNAGR v. Naperville - State of Illinois LetterMarcus Gilmer100% (1)
- Gov. Haley's Executive Order and Letter To The SC Inspector General To Look For Ways To Improve Cyber Security in State AgenciesDocument3 pagesGov. Haley's Executive Order and Letter To The SC Inspector General To Look For Ways To Improve Cyber Security in State AgenciesThe State NewspaperNo ratings yet
- September 27 Adeline Hambley Response To FY24 Budget ApprovalDocument3 pagesSeptember 27 Adeline Hambley Response To FY24 Budget ApprovalWXMINo ratings yet
- Nevada Republican Club LetterDocument2 pagesNevada Republican Club LetterJessica HillNo ratings yet
- Complaint Against Jay Jacobs and Nassau Democratic CommitteesDocument43 pagesComplaint Against Jay Jacobs and Nassau Democratic Committeesrebellando10100% (1)
- NAACP Letter of Support Jackson MS FINAL - Omnibus FY23Document2 pagesNAACP Letter of Support Jackson MS FINAL - Omnibus FY23Anthony WarrenNo ratings yet
- Riverside County Grand Jury Report On Short-Term RentalsDocument16 pagesRiverside County Grand Jury Report On Short-Term RentalsThe Press-Enterprise / pressenterprise.comNo ratings yet
- GEI Double Minority Presentation-WONGDocument43 pagesGEI Double Minority Presentation-WONGKate AndersonNo ratings yet
- Engrossed Second Substitute House Bill 1310Document7 pagesEngrossed Second Substitute House Bill 1310Katie CrolleyNo ratings yet
- Elizabeth Schultz and FriendsDocument55 pagesElizabeth Schultz and FriendsFairfaxWatchNo ratings yet
- Lawsuit Challenges Ohio Ban On Foreign Donations in Ballot IssuesDocument47 pagesLawsuit Challenges Ohio Ban On Foreign Donations in Ballot IssuesJessie BalmertNo ratings yet
- 115thCongressionalScorecard ReportDocument33 pages115thCongressionalScorecard ReportEvan HochsteinNo ratings yet
- Classified # I Mary Glass Civil Rights April 1Document10 pagesClassified # I Mary Glass Civil Rights April 1MARY GLASSNo ratings yet
- Urgent Concern - Constitutional Violations in Virginia (11.8.2021)Document1 pageUrgent Concern - Constitutional Violations in Virginia (11.8.2021)Activate VirginiaNo ratings yet
- Rogers LetterDocument3 pagesRogers Letterpgattis7719No ratings yet
- Becerra Hearing Miller QFRsDocument3 pagesBecerra Hearing Miller QFRsKristina WatrobskiNo ratings yet
- Second Letter To DOJ Re Victims 9.8.23 FinalDocument3 pagesSecond Letter To DOJ Re Victims 9.8.23 FinalAlexis LeonardNo ratings yet
- Book Review Committee Member RecommendationsDocument38 pagesBook Review Committee Member RecommendationsDan LehrNo ratings yet
- Complaint DJT FiledDocument36 pagesComplaint DJT FiledTony GarciaNo ratings yet
- (DAILY CALLER OBTAINED) - 9.12.22 - Letter To Garland Re AFPI Report - FINALDocument2 pages(DAILY CALLER OBTAINED) - 9.12.22 - Letter To Garland Re AFPI Report - FINALHenry RodgersNo ratings yet
- Board Warrant For Barlow's ArrestDocument2 pagesBoard Warrant For Barlow's ArrestKUTV 2NewsNo ratings yet
- Duke Realty RezoningDocument79 pagesDuke Realty RezoningZachary HansenNo ratings yet
- Letter Urging Vaccines v1!7!27-21Document3 pagesLetter Urging Vaccines v1!7!27-21USA TODAY NetworkNo ratings yet
- 1123 Special Pension BriefingDocument17 pages1123 Special Pension BriefingAnn DwyerNo ratings yet
- In The Supreme Court of Ohio Bria BennettDocument52 pagesIn The Supreme Court of Ohio Bria BennettKaren KaslerNo ratings yet
- American Accountability Foundation Letter To Senators On Gigi SohnDocument2 pagesAmerican Accountability Foundation Letter To Senators On Gigi SohnGabe KaminskyNo ratings yet
- Minnesota Deer Farmers Association V The State of Minnesota Et Al Mndce-23-03907 0001.0Document60 pagesMinnesota Deer Farmers Association V The State of Minnesota Et Al Mndce-23-03907 0001.0Sally Jo SorensenNo ratings yet
- Synagogue Sues Over Florida's 15-Week Abortion RestrictionsDocument35 pagesSynagogue Sues Over Florida's 15-Week Abortion RestrictionsWTSP 10No ratings yet
- Brown County DA Statement On GOTV EffortDocument2 pagesBrown County DA Statement On GOTV EffortJonathan KrauseNo ratings yet
- 7/26/23 Letter From America First Legal To PWC On DiscriminationDocument6 pages7/26/23 Letter From America First Legal To PWC On DiscriminationAdrienne GonzalezNo ratings yet
- 11 3 20 Barnett V Lawrence ComplaintDocument14 pages11 3 20 Barnett V Lawrence ComplaintLaw&CrimeNo ratings yet
- Parchman Emergency MotionDocument62 pagesParchman Emergency MotionLuke R100% (1)
- Response and Emails Re Efforts To Terminate Ottawa County Health Public Health Officer Adeline HambleyDocument14 pagesResponse and Emails Re Efforts To Terminate Ottawa County Health Public Health Officer Adeline HambleyWXMINo ratings yet
- Research Paper On Medical CannabisDocument8 pagesResearch Paper On Medical Cannabisegyr68dw100% (1)
- Logan Walker - Argumentative EssayDocument5 pagesLogan Walker - Argumentative Essayapi-569152883No ratings yet
- Medical Marijuana Research Paper ThesisDocument7 pagesMedical Marijuana Research Paper Thesissuw1vadibys2100% (1)
- Medicinal Cannabis Thesis StatementDocument5 pagesMedicinal Cannabis Thesis Statementbsrf4d9d100% (2)
- Legalization of Marijuana For Medical Use in The PhilippinesDocument5 pagesLegalization of Marijuana For Medical Use in The PhilippinesRey Emerson EscuetaNo ratings yet
- Legalization of Medical Marijuana in The United StatesDocument12 pagesLegalization of Medical Marijuana in The United StatesTeresa SmithNo ratings yet
- Economic Impact Study SummaryDocument40 pagesEconomic Impact Study SummaryMike CasonNo ratings yet
- Congressional Districts Livingston PlanDocument1 pageCongressional Districts Livingston PlanMike CasonNo ratings yet
- LTR ADAH Legislators FFT 230714Document4 pagesLTR ADAH Legislators FFT 230714Craig MongerNo ratings yet
- Minority Representation ReportDocument108 pagesMinority Representation ReportMike CasonNo ratings yet
- Clergy Letter To Governor IveyDocument8 pagesClergy Letter To Governor IveyMike CasonNo ratings yet
- Clergy Letter To Governor IveyDocument8 pagesClergy Letter To Governor IveyMike CasonNo ratings yet
- Aaron Cody Smith Case Supreme Court Denies WritDocument17 pagesAaron Cody Smith Case Supreme Court Denies WritMike CasonNo ratings yet
- Alabama Infant Mortality Report 2021Document31 pagesAlabama Infant Mortality Report 2021Mike CasonNo ratings yet
- Statehouse To Prison Pipeline ReportDocument25 pagesStatehouse To Prison Pipeline ReportMike CasonNo ratings yet
- COJ Judgment in Tracie Todd CaseDocument5 pagesCOJ Judgment in Tracie Todd CaseMike CasonNo ratings yet
- Gov. Kay Ivey State Vehicle MemorandumDocument1 pageGov. Kay Ivey State Vehicle MemorandumMike CasonNo ratings yet
- Senate Bill 184Document11 pagesSenate Bill 184Mike CasonNo ratings yet
- Letter To John Merrill On Polling Place ListDocument9 pagesLetter To John Merrill On Polling Place ListMike CasonNo ratings yet
- Alabama Prison Bond TermsDocument33 pagesAlabama Prison Bond TermsMike CasonNo ratings yet
- Letter Seeking Clarity On Abortion LawDocument4 pagesLetter Seeking Clarity On Abortion LawMike Cason100% (1)
- Letter To Gov. Ivey On Judgeship TransferDocument4 pagesLetter To Gov. Ivey On Judgeship TransferMike CasonNo ratings yet
- Alabama Medical Cannabis Law SummaryDocument38 pagesAlabama Medical Cannabis Law SummaryJohn SharpNo ratings yet
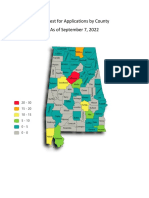
- Alabama Medical Cannabis Commission Map of License Application RequestsDocument1 pageAlabama Medical Cannabis Commission Map of License Application RequestsMike CasonNo ratings yet
- Spreadsheet For Proposed Alabama General Fund Budget For 2023Document14 pagesSpreadsheet For Proposed Alabama General Fund Budget For 2023Mike CasonNo ratings yet
- FactsheetDocument4 pagesFactsheetapi-356827363No ratings yet
- Lynda Blanchard LawsuitDocument47 pagesLynda Blanchard LawsuitMike CasonNo ratings yet
- Judge Tracie Todd Final Judgment by Alabama Court of The JudiciaryDocument6 pagesJudge Tracie Todd Final Judgment by Alabama Court of The JudiciaryMike CasonNo ratings yet
- Alabama Sentencing Commission Prison Population ReportDocument12 pagesAlabama Sentencing Commission Prison Population ReportMike CasonNo ratings yet
- Merrill Vs MilliganDocument21 pagesMerrill Vs Milliganstreiff at redstate100% (1)
- Alabama Senate Race Poll by McLaughlin & AssociatesDocument7 pagesAlabama Senate Race Poll by McLaughlin & AssociatesMike CasonNo ratings yet
- Appeal To Supreme Court Over OSHA COVID-19 Vaccine MandateDocument54 pagesAppeal To Supreme Court Over OSHA COVID-19 Vaccine MandateWMBF News100% (1)
- Pardons and Paroles Statistical ReportDocument13 pagesPardons and Paroles Statistical ReportMike CasonNo ratings yet
- S+ Engineering: Composer Harmony 6.1: View and Monitor ManualDocument45 pagesS+ Engineering: Composer Harmony 6.1: View and Monitor ManualvodanhNo ratings yet
- Ai - Unit IiDocument126 pagesAi - Unit IiAbhinaya ChavaliNo ratings yet
- 2003 Crisis Management and Tourism Beyond The RhetoricDocument24 pages2003 Crisis Management and Tourism Beyond The RhetoricPantazis PastrasNo ratings yet
- Battery MSDSDocument3 pagesBattery MSDSAnkitNo ratings yet
- Tutorial 2.3Document3 pagesTutorial 2.3Ho Fung ChernNo ratings yet
- Belief and Conditions in Environmental AwarenessDocument28 pagesBelief and Conditions in Environmental AwarenessDanielle Kate MadridNo ratings yet
- Person Involved in The Incident Full Name: Designation: Office: Incident Information Date: October 6, 2020 Location of Incident: Incident DescriptionDocument3 pagesPerson Involved in The Incident Full Name: Designation: Office: Incident Information Date: October 6, 2020 Location of Incident: Incident DescriptionLeonardo Jr SultanNo ratings yet
- Sant Kabeer - DohasDocument23 pagesSant Kabeer - DohasAniket100% (2)
- Economic Mineral Deposits of PakistanDocument12 pagesEconomic Mineral Deposits of PakistanOolasyar Khattak67% (12)
- 71 75 PBDocument63 pages71 75 PBJoey FalaNo ratings yet
- Brainstorming 2Document14 pagesBrainstorming 2AmierahIzzatiAisyahNo ratings yet
- PM 150 CSD 120Document7 pagesPM 150 CSD 120elecompinnNo ratings yet
- SM Project Report - P&GDocument22 pagesSM Project Report - P&GNikhil AjwaniNo ratings yet
- 30+ Types of Project RiskDocument1 page30+ Types of Project RiskSulemanNo ratings yet
- 11 Physical Education Chapter 3Document12 pages11 Physical Education Chapter 3shreyNo ratings yet
- Tickler Final PDFDocument29 pagesTickler Final PDFSerious LeoNo ratings yet
- (S) Topic 1 - IntroductionDocument11 pages(S) Topic 1 - IntroductionKelvin YapNo ratings yet
- RealVNC Enterprise Edition 4Document2 pagesRealVNC Enterprise Edition 4fannybrawijayaNo ratings yet
- Parents ConsentDocument2 pagesParents ConsentkarlylNo ratings yet
- Fluid 04Document104 pagesFluid 04Edgar HuancaNo ratings yet
- OS Forecast Kwartal Mei - Agst 2024Document22 pagesOS Forecast Kwartal Mei - Agst 2024Iqbal MontgomeryNo ratings yet
- Ice Hockey GoaliesDocument4 pagesIce Hockey GoaliesDylan HochreiterNo ratings yet
- Zhao - An Intertextual Approach To Translation at The Macro-LevelDocument9 pagesZhao - An Intertextual Approach To Translation at The Macro-LevelangielskiajNo ratings yet
- Desert Explorer1Document44 pagesDesert Explorer1Wes ChambersNo ratings yet
- The Story of Adam and EveDocument3 pagesThe Story of Adam and EveJensen ManaloNo ratings yet
- Lesson 1Document36 pagesLesson 1Phước NguyễnNo ratings yet
- Jawaban Pma 1-100Document4 pagesJawaban Pma 1-100Agung KurniawanNo ratings yet