Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pediatric Nursing Knowledge & Skills ChecklistDocument4 pagesPediatric Nursing Knowledge & Skills Checklistnorthweststaffing67% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Jadwal Jaga Bulan Oktober 2021Document4 pagesJadwal Jaga Bulan Oktober 2021Devi SetiawanNo ratings yet
- Rancangan Jadwal Oktober 2021Document16 pagesRancangan Jadwal Oktober 2021Devi SetiawanNo ratings yet
- Vocabulary (In and Around The Hospital)Document3 pagesVocabulary (In and Around The Hospital)Devi SetiawanNo ratings yet
- Resume Dan Askep Peritonitis (HDocument10 pagesResume Dan Askep Peritonitis (HDevi SetiawanNo ratings yet
- Class C - 1Document2 pagesClass C - 1Devi SetiawanNo ratings yet
- DeviDocument4 pagesDeviDevi SetiawanNo ratings yet
- English in Nursing Science Assignment Name: Devi SetiawanDocument12 pagesEnglish in Nursing Science Assignment Name: Devi SetiawanDevi SetiawanNo ratings yet
- Curiculum VitaeDocument1 pageCuriculum VitaeDevi SetiawanNo ratings yet
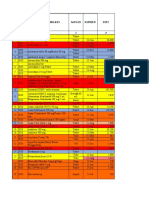
- No Tahun Nama Obat / Perbelkes Satuan Expired UnitDocument5 pagesNo Tahun Nama Obat / Perbelkes Satuan Expired UnitBayu Firmansyah AlitNo ratings yet
- A Multidisciplinary Approach To Management of TinnitusDocument8 pagesA Multidisciplinary Approach To Management of TinnitusAsti YuliadhaNo ratings yet
- ESAMCC7Document206 pagesESAMCC7jeremy_raineyNo ratings yet
- Surgical Neurology International: Fibromyalgia and Arachnoiditis Presented As An Acute Spinal DisorderDocument6 pagesSurgical Neurology International: Fibromyalgia and Arachnoiditis Presented As An Acute Spinal DisorderMartha OktaviaNo ratings yet
- How To Use This MedicineDocument2 pagesHow To Use This MedicinelelaniaNo ratings yet
- SonotronDocument10 pagesSonotronSyafiq YusryNo ratings yet
- A Week in The Life of A Hospital Physician by Isaac DayanDocument3 pagesA Week in The Life of A Hospital Physician by Isaac DayanYOFHSNo ratings yet
- Physical TherapyDocument11 pagesPhysical TherapyEvelyn MedinaNo ratings yet
- A Study On Impact of Acne Vulgaris On Quality of LifeDocument7 pagesA Study On Impact of Acne Vulgaris On Quality of LifeIJAR JOURNALNo ratings yet
- Defining The Practice of Medical TechnologyDocument47 pagesDefining The Practice of Medical TechnologyCharles Ian OliquinoNo ratings yet
- ProPath Selected As Medical Director For Baylor Scott & White Medical Center - SunnyvaleDocument3 pagesProPath Selected As Medical Director For Baylor Scott & White Medical Center - SunnyvalePR.comNo ratings yet
- Complex Regional Pain SyndromeDocument10 pagesComplex Regional Pain SyndromegeejeiNo ratings yet
- Immunization PDFDocument23 pagesImmunization PDFعبدالرحمن علىNo ratings yet
- Maria Case Study 2Document2 pagesMaria Case Study 2api-316574434No ratings yet
- The Bigger The Bulge The Better - Rayner & Smale PDFDocument4 pagesThe Bigger The Bulge The Better - Rayner & Smale PDFItai IzhakNo ratings yet
- Otology Fellowships 2019Document5 pagesOtology Fellowships 2019Sandra SandrinaNo ratings yet
- Hypertension & Diabetis MellitusDocument51 pagesHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- Stok Opname: Tablet No Nama Obat SisaDocument7 pagesStok Opname: Tablet No Nama Obat SisajuleNo ratings yet
- Trauma-Sensitive Yoga - Principles, Practice and ResearchDocument6 pagesTrauma-Sensitive Yoga - Principles, Practice and ResearchRichard Guerra100% (1)
- Clinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessDocument4 pagesClinical Manifestations and Management of Hospitalized Women With Bartholin Versus Non Bartholin Vulvar AbscessPaul HartingNo ratings yet
- Uti ProphylaxisDocument9 pagesUti ProphylaxisaNo ratings yet
- Odd Adhd Case StudyDocument8 pagesOdd Adhd Case StudyRich AmbroseNo ratings yet
- Manuver Head Tilt-Chin Lift-Jaw ThrustDocument6 pagesManuver Head Tilt-Chin Lift-Jaw ThrustKevin CindarjoNo ratings yet
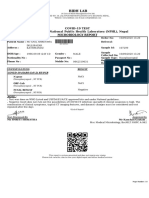
- Covid-19 Test Authorized by National Public Health Laboratory (NPHL), Nepal Microbiology ReportDocument1 pageCovid-19 Test Authorized by National Public Health Laboratory (NPHL), Nepal Microbiology ReportAnil ShresthaNo ratings yet
- Stem Cells Treatment Potential Therapy DiseasesDocument11 pagesStem Cells Treatment Potential Therapy DiseasesNOVO Cellular Medicine InstituteNo ratings yet
- App en 4Document5 pagesApp en 4Reena RamosNo ratings yet
- Skin Assessment ActivityDocument6 pagesSkin Assessment ActivityRenee Dwi Permata MessakaraengNo ratings yet
- Instructions: Certification of Health Care Provider: Family and Medical Leave ActDocument5 pagesInstructions: Certification of Health Care Provider: Family and Medical Leave ActMichelleNo ratings yet
- Wilson's DiseaseDocument52 pagesWilson's DiseaseAmit KumarNo ratings yet