Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Curriculum Vitae: Personal InformationDocument2 pagesCurriculum Vitae: Personal InformationChun TironeeNo ratings yet
- Motivation Leter and CompaniesDocument2 pagesMotivation Leter and CompaniesChun TironeeNo ratings yet
- Pass CrackerDocument1 pagePass CrackerChun TironeeNo ratings yet
- Terminal Velocity1Document11 pagesTerminal Velocity1Chun TironeeNo ratings yet
- HTR India - Products - Wire Wound Resistors - Silicone Coated Resistors - HTA (English)Document3 pagesHTR India - Products - Wire Wound Resistors - Silicone Coated Resistors - HTA (English)crplzNo ratings yet
- WPS Format For Asme Ix - Wps - Gtaw Fcaw GmawDocument1 pageWPS Format For Asme Ix - Wps - Gtaw Fcaw GmawThe Welding Inspections CommunityNo ratings yet
- APRS Tracker X1C3 ManualDocument20 pagesAPRS Tracker X1C3 ManualVisal KelNo ratings yet
- Design Standards Manual: Chapter 3 - Civil Design: Facilities Management and Operations CenterDocument31 pagesDesign Standards Manual: Chapter 3 - Civil Design: Facilities Management and Operations CenterTumulak IanNo ratings yet
- Format For Research Paper (Immersion)Document4 pagesFormat For Research Paper (Immersion)Dayanara LabardaNo ratings yet
- ARMY TM 5-822-7 Air Force Afm 88-6, Chap. 8Document55 pagesARMY TM 5-822-7 Air Force Afm 88-6, Chap. 8PDHLibraryNo ratings yet
- Complexity1 Quick SummaryDocument5 pagesComplexity1 Quick SummaryagNo ratings yet
- DG型高压锅炉给水泵说明书 tài liệu kỹ thuật bơm cấpDocument26 pagesDG型高压锅炉给水泵说明书 tài liệu kỹ thuật bơm cấpMạnh CườngNo ratings yet
- OMRON - E5CZ DatasheetDocument17 pagesOMRON - E5CZ DatasheetLove BoyNo ratings yet
- Nibiru Research Gerald Clark 04.28.15 PDFDocument49 pagesNibiru Research Gerald Clark 04.28.15 PDFsunsangra100% (1)
- Cashew Nut Biosorbent For Heavy Metal Ions RemovalNi PDFDocument12 pagesCashew Nut Biosorbent For Heavy Metal Ions RemovalNi PDFAnonymous YagZQlNo ratings yet
- Tensorflow Deep Learning With KerasDocument90 pagesTensorflow Deep Learning With Keraswick91274No ratings yet
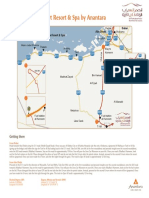
- Qasr Al Sarab Desert Resort Location Map June2012Document1 pageQasr Al Sarab Desert Resort Location Map June2012Anant GârgNo ratings yet
- Lab ProgramsDocument13 pagesLab ProgramsAkhila RNo ratings yet
- 2024 Bss Chemistry P IIDocument8 pages2024 Bss Chemistry P IIbarotathomas1234No ratings yet
- Bassman 400Document17 pagesBassman 400Hasanudin UdinNo ratings yet
- Tip Izvještaja: Instalirani Softver Na Računaru SERVKUPACA-RS03Document2 pagesTip Izvještaja: Instalirani Softver Na Računaru SERVKUPACA-RS03milenkovic_sasaNo ratings yet
- 2018 May June IGCSE Chemistry Past Paper 3Document16 pages2018 May June IGCSE Chemistry Past Paper 3saowanee toonchueNo ratings yet
- Gas Train Equipment 2016Document91 pagesGas Train Equipment 2016Ivan BeljinNo ratings yet
- Studies On Biosorption of Titan Yellow Dye With Hyptis Suaveolens Powder and Optimization Through Central Composite DesignDocument16 pagesStudies On Biosorption of Titan Yellow Dye With Hyptis Suaveolens Powder and Optimization Through Central Composite DesignInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Operasi&Deteksi KerusakanDocument27 pagesOperasi&Deteksi KerusakandennybtgNo ratings yet
- Laboratory Bias Detection Using Single Test Result From Standard MaterialDocument5 pagesLaboratory Bias Detection Using Single Test Result From Standard Materialmohammed karasnehNo ratings yet
- Eaton 281198 Dilm65 XMV en GBDocument2 pagesEaton 281198 Dilm65 XMV en GBwajdyzNo ratings yet
- Mixed Liquor Volatile Suspended SolidsDocument4 pagesMixed Liquor Volatile Suspended Solidscva50% (2)
- Calcaneal FracturesDocument39 pagesCalcaneal FracturesNavin ChandarNo ratings yet
- 46 Useful PHP Code SnippetsDocument39 pages46 Useful PHP Code SnippetsMassimo GeovanniiNo ratings yet
- Convolutional Codes706760093Document27 pagesConvolutional Codes706760093Feroza MirajkarNo ratings yet
- Node-Based VS Layer-Based: Compositing SoftwareDocument4 pagesNode-Based VS Layer-Based: Compositing Softwaredak280No ratings yet
- Chapter 5 Stresses in Beams With Solved ProblemsDocument65 pagesChapter 5 Stresses in Beams With Solved ProblemsWnikyla Manggad BalanguiNo ratings yet
- A Big Five Scoring System MBTIDocument10 pagesA Big Five Scoring System MBTIcapuletoNo ratings yet