
Ken
Ken
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 2017-CE May PDFDocument32 pages2017-CE May PDFKristin Argosino100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HydraulicsDocument8 pagesHydraulicsKristin ArgosinoNo ratings yet
- Algebra 2 Discussion (CLK)Document16 pagesAlgebra 2 Discussion (CLK)Kristin ArgosinoNo ratings yet
- Math MeDocument7 pagesMath MeKristin ArgosinoNo ratings yet
- Simplified Steel DesignDocument473 pagesSimplified Steel DesignKristin ArgosinoNo ratings yet
- Fans and Blowers ReportDocument49 pagesFans and Blowers ReportKristin ArgosinoNo ratings yet
- Engineering MechanicsDocument320 pagesEngineering MechanicsKristin Argosino67% (3)
- Set 1 Problems PDFDocument2 pagesSet 1 Problems PDFKristin Argosino0% (1)
- Name Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisDocument3 pagesName Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisKristin ArgosinoNo ratings yet
- Compute The Stadia Interval FactorDocument7 pagesCompute The Stadia Interval FactorKristin ArgosinoNo ratings yet
- Stresses in Soil Mass Problem 1: Foundation Engineering 1Document3 pagesStresses in Soil Mass Problem 1: Foundation Engineering 1Kristin ArgosinoNo ratings yet
- CALENDARDocument1 pageCALENDARKristin ArgosinoNo ratings yet
- Basis of Bisection MethodDocument31 pagesBasis of Bisection MethodKristin ArgosinoNo ratings yet
- Newton-Raphson: Prepared By: Cielito V. Maligagli, RCEDocument6 pagesNewton-Raphson: Prepared By: Cielito V. Maligagli, RCEKristin ArgosinoNo ratings yet
- Modification Design of Stone Mastic Asphalt Using Polypropylene Film As Additives To BitumenDocument5 pagesModification Design of Stone Mastic Asphalt Using Polypropylene Film As Additives To BitumenKristin ArgosinoNo ratings yet
- Prestressed Concrete Design ObjectivesDocument15 pagesPrestressed Concrete Design ObjectivesKristin ArgosinoNo ratings yet
- Name Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisDocument3 pagesName Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisKristin ArgosinoNo ratings yet
- Book 1Document2 pagesBook 1Kristin ArgosinoNo ratings yet
- Part 3 4 SPECS CONTRACTSDocument45 pagesPart 3 4 SPECS CONTRACTSKristin ArgosinoNo ratings yet
- Argosino Martee Socio Eco IssuesDocument4 pagesArgosino Martee Socio Eco IssuesKristin ArgosinoNo ratings yet
- No.1 PrestressedDocument10 pagesNo.1 PrestressedKristin ArgosinoNo ratings yet
- SteelDocument61 pagesSteelSonNguyenNo ratings yet
- HD Hammock InstDocument4 pagesHD Hammock InstLarry WagarNo ratings yet
- Case Study TPM Jet AirwaysDocument15 pagesCase Study TPM Jet AirwaysSanjay Domdiya100% (1)
- Calibration Curve Between Pressure Drop and Mass Flow RateDocument2 pagesCalibration Curve Between Pressure Drop and Mass Flow RateMikail IsmailNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- Light and ShadowDocument5 pagesLight and ShadowLisa Lipsett50% (2)
- HP 245 G6 Notebook PC: Maintenance and Service GuideDocument106 pagesHP 245 G6 Notebook PC: Maintenance and Service GuideStevenson QuinteroNo ratings yet
- Substation Construction and CommissioningDocument83 pagesSubstation Construction and CommissioningShung Tak ChanNo ratings yet
- Generalbio2 StecDocument105 pagesGeneralbio2 StecJohn V. LabradorNo ratings yet
- Definitive Guide Robot Welding Torches v1.0Document50 pagesDefinitive Guide Robot Welding Torches v1.0AlexgriNo ratings yet
- 11 VESDA Pipes and Fittings TDS AQ IE LoresDocument4 pages11 VESDA Pipes and Fittings TDS AQ IE Loresarmand isakhNo ratings yet
- Drug Induced OsteoporosisDocument8 pagesDrug Induced OsteoporosislueglemeNo ratings yet
- To Study Well Design Aspects in HPHT EnvironmentDocument40 pagesTo Study Well Design Aspects in HPHT Environmentnikhil_barshettiwat100% (1)
- Turbo Charger - ProjectDocument36 pagesTurbo Charger - ProjectSam Sams100% (2)
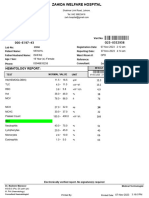
- Hematology Report:: MRN: Visit NoDocument1 pageHematology Report:: MRN: Visit Nojuniadsheikh6No ratings yet
- ColaTeric BE 16Document2 pagesColaTeric BE 16mndmattNo ratings yet
- 6-Büşra BahatDocument4 pages6-Büşra BahatAYŞE NURNo ratings yet
- Kant's Concept of BeautyDocument14 pagesKant's Concept of BeautyVishnuNo ratings yet
- PHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdDocument6 pagesPHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdHarsitNo ratings yet
- UBE-H-103 - Piping and Ducting MaterialDocument587 pagesUBE-H-103 - Piping and Ducting Materialjohn carterNo ratings yet
- Avago HLCP j100, HDSP 48xxDocument7 pagesAvago HLCP j100, HDSP 48xxvelizarkoNo ratings yet
- Hypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHDocument6 pagesHypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHLeyla SaabNo ratings yet
- Einstein HomeworkDocument8 pagesEinstein Homeworkgfdrvlyod100% (1)
- Fortran CF DDocument160 pagesFortran CF DLahcen AkerkouchNo ratings yet
- Edux110 SimDocument307 pagesEdux110 SimElijahNo ratings yet
- Soal OkeDocument12 pagesSoal OkefredyNo ratings yet
- 6 - DNV - Composites Repair JIP - New Approach To Repair of FPSO's Without Hot Work Using Glueing PolymersDocument31 pages6 - DNV - Composites Repair JIP - New Approach To Repair of FPSO's Without Hot Work Using Glueing PolymersAnonymous 19QCaJNo ratings yet
- Renoise User ManualDocument198 pagesRenoise User Manualdrkstr77No ratings yet
- GEA Chapter6 Economy HiresDocument37 pagesGEA Chapter6 Economy HiresMike LassaNo ratings yet
- Mathematics ECAT (Sir Nasim Zulfiqar) - 1Document134 pagesMathematics ECAT (Sir Nasim Zulfiqar) - 1AYESH qureshiNo ratings yet


























































































Download as docx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 2017-CE May PDFDocument32 pages2017-CE May PDFKristin Argosino100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- HydraulicsDocument8 pagesHydraulicsKristin ArgosinoNo ratings yet
- Algebra 2 Discussion (CLK)Document16 pagesAlgebra 2 Discussion (CLK)Kristin ArgosinoNo ratings yet
- Math MeDocument7 pagesMath MeKristin ArgosinoNo ratings yet
- Simplified Steel DesignDocument473 pagesSimplified Steel DesignKristin ArgosinoNo ratings yet
- Fans and Blowers ReportDocument49 pagesFans and Blowers ReportKristin ArgosinoNo ratings yet
- Engineering MechanicsDocument320 pagesEngineering MechanicsKristin Argosino67% (3)
- Set 1 Problems PDFDocument2 pagesSet 1 Problems PDFKristin Argosino0% (1)
- Name Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisDocument3 pagesName Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisKristin ArgosinoNo ratings yet
- Compute The Stadia Interval FactorDocument7 pagesCompute The Stadia Interval FactorKristin ArgosinoNo ratings yet
- Stresses in Soil Mass Problem 1: Foundation Engineering 1Document3 pagesStresses in Soil Mass Problem 1: Foundation Engineering 1Kristin ArgosinoNo ratings yet
- CALENDARDocument1 pageCALENDARKristin ArgosinoNo ratings yet
- Basis of Bisection MethodDocument31 pagesBasis of Bisection MethodKristin ArgosinoNo ratings yet
- Newton-Raphson: Prepared By: Cielito V. Maligagli, RCEDocument6 pagesNewton-Raphson: Prepared By: Cielito V. Maligagli, RCEKristin ArgosinoNo ratings yet
- Modification Design of Stone Mastic Asphalt Using Polypropylene Film As Additives To BitumenDocument5 pagesModification Design of Stone Mastic Asphalt Using Polypropylene Film As Additives To BitumenKristin ArgosinoNo ratings yet
- Prestressed Concrete Design ObjectivesDocument15 pagesPrestressed Concrete Design ObjectivesKristin ArgosinoNo ratings yet
- Name Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisDocument3 pagesName Title Kristine Mae O. Argosino: Procedures For Spectrum AnalysisKristin ArgosinoNo ratings yet
- Book 1Document2 pagesBook 1Kristin ArgosinoNo ratings yet
- Part 3 4 SPECS CONTRACTSDocument45 pagesPart 3 4 SPECS CONTRACTSKristin ArgosinoNo ratings yet
- Argosino Martee Socio Eco IssuesDocument4 pagesArgosino Martee Socio Eco IssuesKristin ArgosinoNo ratings yet
- No.1 PrestressedDocument10 pagesNo.1 PrestressedKristin ArgosinoNo ratings yet
- SteelDocument61 pagesSteelSonNguyenNo ratings yet
- HD Hammock InstDocument4 pagesHD Hammock InstLarry WagarNo ratings yet
- Case Study TPM Jet AirwaysDocument15 pagesCase Study TPM Jet AirwaysSanjay Domdiya100% (1)
- Calibration Curve Between Pressure Drop and Mass Flow RateDocument2 pagesCalibration Curve Between Pressure Drop and Mass Flow RateMikail IsmailNo ratings yet
- The Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFDocument2 pagesThe Secrets of Ancient Rome's Buildings - History - Smithsonian Magazine PDFMarlui Faith MaglambayanNo ratings yet
- Light and ShadowDocument5 pagesLight and ShadowLisa Lipsett50% (2)
- HP 245 G6 Notebook PC: Maintenance and Service GuideDocument106 pagesHP 245 G6 Notebook PC: Maintenance and Service GuideStevenson QuinteroNo ratings yet
- Substation Construction and CommissioningDocument83 pagesSubstation Construction and CommissioningShung Tak ChanNo ratings yet
- Generalbio2 StecDocument105 pagesGeneralbio2 StecJohn V. LabradorNo ratings yet
- Definitive Guide Robot Welding Torches v1.0Document50 pagesDefinitive Guide Robot Welding Torches v1.0AlexgriNo ratings yet
- 11 VESDA Pipes and Fittings TDS AQ IE LoresDocument4 pages11 VESDA Pipes and Fittings TDS AQ IE Loresarmand isakhNo ratings yet
- Drug Induced OsteoporosisDocument8 pagesDrug Induced OsteoporosislueglemeNo ratings yet
- To Study Well Design Aspects in HPHT EnvironmentDocument40 pagesTo Study Well Design Aspects in HPHT Environmentnikhil_barshettiwat100% (1)
- Turbo Charger - ProjectDocument36 pagesTurbo Charger - ProjectSam Sams100% (2)
- Hematology Report:: MRN: Visit NoDocument1 pageHematology Report:: MRN: Visit Nojuniadsheikh6No ratings yet
- ColaTeric BE 16Document2 pagesColaTeric BE 16mndmattNo ratings yet
- 6-Büşra BahatDocument4 pages6-Büşra BahatAYŞE NURNo ratings yet
- Kant's Concept of BeautyDocument14 pagesKant's Concept of BeautyVishnuNo ratings yet
- PHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdDocument6 pagesPHY101A: Home Experiment - 1: Simple Pendulum: PHY101A - Physics Laboratory Ha - 1B Ynm/Ahk/Sub/SdHarsitNo ratings yet
- UBE-H-103 - Piping and Ducting MaterialDocument587 pagesUBE-H-103 - Piping and Ducting Materialjohn carterNo ratings yet
- Avago HLCP j100, HDSP 48xxDocument7 pagesAvago HLCP j100, HDSP 48xxvelizarkoNo ratings yet
- Hypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHDocument6 pagesHypomorphic Mutations in PRF1, MUNC13-4, and STXBP2 Are Associated With Adult-Onset Familial HLHLeyla SaabNo ratings yet
- Einstein HomeworkDocument8 pagesEinstein Homeworkgfdrvlyod100% (1)
- Fortran CF DDocument160 pagesFortran CF DLahcen AkerkouchNo ratings yet
- Edux110 SimDocument307 pagesEdux110 SimElijahNo ratings yet
- Soal OkeDocument12 pagesSoal OkefredyNo ratings yet
- 6 - DNV - Composites Repair JIP - New Approach To Repair of FPSO's Without Hot Work Using Glueing PolymersDocument31 pages6 - DNV - Composites Repair JIP - New Approach To Repair of FPSO's Without Hot Work Using Glueing PolymersAnonymous 19QCaJNo ratings yet
- Renoise User ManualDocument198 pagesRenoise User Manualdrkstr77No ratings yet
- GEA Chapter6 Economy HiresDocument37 pagesGEA Chapter6 Economy HiresMike LassaNo ratings yet
- Mathematics ECAT (Sir Nasim Zulfiqar) - 1Document134 pagesMathematics ECAT (Sir Nasim Zulfiqar) - 1AYESH qureshiNo ratings yet