Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ge Hong and Zhou Hou Jiu Zu Fang (A Handbook of Formulas For Emergencies)Document2 pagesGe Hong and Zhou Hou Jiu Zu Fang (A Handbook of Formulas For Emergencies)GobiNo ratings yet
- Stages of LaborDocument5 pagesStages of LaborGeraldine Marie Salvo100% (4)
- Science 10 Quarter 3 Week 5 1Document5 pagesScience 10 Quarter 3 Week 5 1Celeste PalogmeNo ratings yet
- Nclex Questions FinalsDocument301 pagesNclex Questions Finalsticoystephanie100% (2)
- Rainer M. Holm-Hadulla, Alina Bertolino: Use of Drugs by Jazz MusiciansDocument3 pagesRainer M. Holm-Hadulla, Alina Bertolino: Use of Drugs by Jazz MusiciansTitikshaNo ratings yet
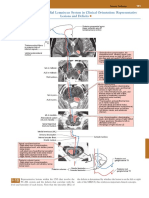
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 pagePosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezNo ratings yet
- CDC - Stool Specimen CollectionDocument3 pagesCDC - Stool Specimen CollectionC. HidalgoNo ratings yet
- NGT Insertion 2022Document41 pagesNGT Insertion 2022Krishna Faith P. DelaraNo ratings yet
- Sickle Cell Anemia Thesis StatementDocument4 pagesSickle Cell Anemia Thesis StatementStacy Vasquez100% (2)
- 0306-4941878 (DR - Sadaqat Baloch) Bio MDCAT ReproductionDocument2 pages0306-4941878 (DR - Sadaqat Baloch) Bio MDCAT ReproductionSADAQAT ALI KHANNo ratings yet
- McCoy 2006 - Essay On YogaDocument102 pagesMcCoy 2006 - Essay On YogaRulosNo ratings yet
- Varilrix Detail Aid DraftDocument5 pagesVarilrix Detail Aid DraftpheverishNo ratings yet
- DiphenhydramineDocument6 pagesDiphenhydramineAndrea BroccoliNo ratings yet
- Excessive Genu Valgum FINALDocument13 pagesExcessive Genu Valgum FINALMeeraNo ratings yet
- Khalifeh 2016Document16 pagesKhalifeh 2016Felipe LazoNo ratings yet
- DetainedyouthDocument3 pagesDetainedyouthlosangelesNo ratings yet
- Risk AssessmentDocument101 pagesRisk Assessmentrevu dasNo ratings yet
- Assignment QIMP PDF 1Document20 pagesAssignment QIMP PDF 1Amrin AdibaNo ratings yet
- Repeat Case Breech 1Document73 pagesRepeat Case Breech 1Francis MendozaNo ratings yet
- Scientific ProgramDocument40 pagesScientific ProgramDrAhmad HammadyNo ratings yet
- HallDocument804 pagesHallMichael100% (1)
- 2023 - George Felfoldi (eBook-Herbs) Health Benefits of Leaf of Life, 126 PagesDocument126 pages2023 - George Felfoldi (eBook-Herbs) Health Benefits of Leaf of Life, 126 PagesGeorge FelfoldiNo ratings yet
- GPAT Microbiology SyllabusDocument2 pagesGPAT Microbiology Syllabuskumar HarshNo ratings yet
- Literature Review Cross ReferencingDocument4 pagesLiterature Review Cross Referencingafdtxmwjs100% (1)
- Acupuncture and Cold Laser Therapy For Pudendal Nerve PainDocument8 pagesAcupuncture and Cold Laser Therapy For Pudendal Nerve PainJøsh HessNo ratings yet
- Test 1-5Document34 pagesTest 1-5Phương Anh NguyễnNo ratings yet
- Patient M. G Drug 1 - Ob MaxDocument5 pagesPatient M. G Drug 1 - Ob MaxGrace MellaineNo ratings yet
- RIISPOA (En)Document13 pagesRIISPOA (En)Caio F Gonçalves NNo ratings yet
- Dysfunctional LaborDocument29 pagesDysfunctional LaborKolimlim, Marienne SD.No ratings yet
- Quiz 2Document5 pagesQuiz 2Ani MepharishviliNo ratings yet