Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- COSHH Risk Assessment For RoundUPDocument2 pagesCOSHH Risk Assessment For RoundUPRonnie Murphy Knotweed Surveyor50% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Safety Culture and Leadership FundamentalsDocument15 pagesSafety Culture and Leadership FundamentalsAurelio DutariNo ratings yet
- Mental Health For StudentsDocument44 pagesMental Health For StudentsRaphahNo ratings yet
- Occupational Safety and Health in Egypt: A National ProfileDocument55 pagesOccupational Safety and Health in Egypt: A National ProfileKatia KallassyNo ratings yet
- Psycho - Synthesis by Roberto AssagioliDocument17 pagesPsycho - Synthesis by Roberto Assagiolimirrej100% (2)
- Garces PsychDocument2 pagesGarces PsychSherlyn Miranda GarcesNo ratings yet
- Change'your'water.' ' ' ' ''Change'your'life'222': Some Beneficial Uses of Kangen WaterDocument1 pageChange'your'water.' ' ' ' ''Change'your'life'222': Some Beneficial Uses of Kangen WaterGyaan WallahNo ratings yet
- A2 Journal Front PageDocument1 pageA2 Journal Front PageMichelle RogersNo ratings yet
- Rituximab Protocol PDFDocument13 pagesRituximab Protocol PDFSenarathKuleeshaKodisinghe100% (1)
- Daftar Pustaka Makalah Tahap IDocument2 pagesDaftar Pustaka Makalah Tahap IAulina Refri RahmiNo ratings yet
- Contoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanDocument12 pagesContoh Soal PG Bahasa Inggris Kelas XI Semester 1 K13 Beserta JawabanIntan Wahyu DhamayantiNo ratings yet
- Origins of InequalitiesDocument1 pageOrigins of InequalitiesDuvNo ratings yet
- MSDS NaOH PDFDocument9 pagesMSDS NaOH PDFSon Luffy JoestarNo ratings yet
- Study of Radiographic Features of Renal Osteodystrophy in Chronic Kidney Disease (CKD) and Their Correlation With Clinical and Biochemical ParametersDocument10 pagesStudy of Radiographic Features of Renal Osteodystrophy in Chronic Kidney Disease (CKD) and Their Correlation With Clinical and Biochemical ParametersIJAR JOURNALNo ratings yet
- Nutrition of Blueberry 10-7-11 MO StrikDocument60 pagesNutrition of Blueberry 10-7-11 MO StrikJesús Miguel Maguiña EspinozaNo ratings yet
- Chrome Galvanize - AerosolDocument1 pageChrome Galvanize - AerosolJodyNo ratings yet
- 2020-02 Report On Blu Room Heart PatientsDocument16 pages2020-02 Report On Blu Room Heart PatientsBlu RoomNo ratings yet
- CHO-KLAT Version2.0 - Young2013Document5 pagesCHO-KLAT Version2.0 - Young2013Nay AungNo ratings yet
- Polysomnograpy: Charmain Beatriz A. AtosDocument62 pagesPolysomnograpy: Charmain Beatriz A. AtosCharmain Beatriz Ayson Atos100% (2)
- Pashupalan Nirdeshika EnglishDocument122 pagesPashupalan Nirdeshika EnglishdpanickerNo ratings yet
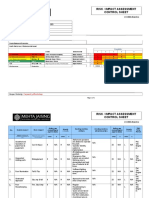
- Risk / Impact Assessment Control Sheet: CC/EHS/RA/014 ContractDocument4 pagesRisk / Impact Assessment Control Sheet: CC/EHS/RA/014 Contractsaurabh juwatkarNo ratings yet
- GDPDocument13 pagesGDPQF Felipe González100% (1)
- (Oxford Handbooks of Political Science) R. A. W. Rhodes, Sarah A. Binder, Bert A. Rockman-Handbook Political Institutions-Oxford University Press, USA (2006)Document456 pages(Oxford Handbooks of Political Science) R. A. W. Rhodes, Sarah A. Binder, Bert A. Rockman-Handbook Political Institutions-Oxford University Press, USA (2006)Perico de los Palotes100% (2)
- Presentation 1Document15 pagesPresentation 1Hala YousefNo ratings yet
- 2015-06-10 - (McCrossin, James) Final REDACTED - CondensedDocument112 pages2015-06-10 - (McCrossin, James) Final REDACTED - CondensedAnonymous dHerywYZ8pNo ratings yet
- Hypernatremia: Kidney Case Conference: How I TreatDocument3 pagesHypernatremia: Kidney Case Conference: How I TreatJulian ViggianoNo ratings yet
- Novilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Diabetes Final Research EssayDocument13 pagesDiabetes Final Research Essayapi-549030089No ratings yet
- Chinese Acupuncture and Moxibustion VideoDocument5 pagesChinese Acupuncture and Moxibustion VideoVirgil Anma100% (1)
- 2021 LFSC Prac 2 GR 12Document8 pages2021 LFSC Prac 2 GR 12Olerato NtsimaneNo ratings yet