Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- MSDS Amerzine SDSDocument11 pagesMSDS Amerzine SDSZKCL Zedkay Corporation LtdNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
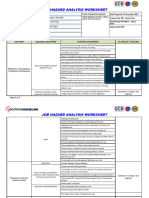
- JHA - Unloading of Sheet PileDocument3 pagesJHA - Unloading of Sheet PileJensen Sunga100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CEMENTUM & CementogenesisDocument41 pagesCEMENTUM & CementogenesisMohammed hisham khan100% (3)
- Competency-Based Learning Materials: Visares National High SchoolDocument43 pagesCompetency-Based Learning Materials: Visares National High SchoolLudivino Toto Ledesma Condalor86% (7)
- Pseudoradicular and Radicular Low-Back Pain: How To Diagnose Clinically?Document3 pagesPseudoradicular and Radicular Low-Back Pain: How To Diagnose Clinically?adeNo ratings yet
- Clinical Communications: Adults: Acute Lumbar Radiculopathy With Weak LegsDocument3 pagesClinical Communications: Adults: Acute Lumbar Radiculopathy With Weak LegsadeNo ratings yet
- Spinal Epidural Abscess A Review With Special Emph PDFDocument7 pagesSpinal Epidural Abscess A Review With Special Emph PDFadeNo ratings yet
- Osteoid Osteoma: A Diagnosis For Radicular Pain of ExtremitiesDocument7 pagesOsteoid Osteoma: A Diagnosis For Radicular Pain of ExtremitiesadeNo ratings yet
- Diseases of The Spine: 2.1 Back PainDocument13 pagesDiseases of The Spine: 2.1 Back PainadeNo ratings yet
- PT1A - Salvadora, N. Assignment 1Document2 pagesPT1A - Salvadora, N. Assignment 1N.No ratings yet
- MSDS Fleetguard ES Complete EG Premix LT16587 ENDocument14 pagesMSDS Fleetguard ES Complete EG Premix LT16587 ENVusal HasanovNo ratings yet
- NICOLAS, SHERENA Q. BSN IV-1 Ass. in NCM119 (LEC)Document7 pagesNICOLAS, SHERENA Q. BSN IV-1 Ass. in NCM119 (LEC)Sherena NicolasNo ratings yet
- Income FlexCareDocument22 pagesIncome FlexCareDarren ChenNo ratings yet
- Instant Download Ebook PDF Adobe Indesign CC Classroom in A Book 2017 Release PDF ScribdDocument41 pagesInstant Download Ebook PDF Adobe Indesign CC Classroom in A Book 2017 Release PDF Scribdwilliam.smith656100% (46)
- Document Required at The Time of Joining: Sr. No. Description RemarksDocument9 pagesDocument Required at The Time of Joining: Sr. No. Description RemarksPrabhati KumuraNo ratings yet
- ICSA Labs ONC HIT Certification Program Certification Manual PDFDocument25 pagesICSA Labs ONC HIT Certification Program Certification Manual PDFSpit FireNo ratings yet
- Impact of Lockdown Due To Coronavirus Pandemic On The Performance of Reliance Industries LTDDocument6 pagesImpact of Lockdown Due To Coronavirus Pandemic On The Performance of Reliance Industries LTDAishNo ratings yet
- Silva, Marlon ArDocument1 pageSilva, Marlon ArTeacher Ronel SDO NavotasNo ratings yet
- PreviewpdfDocument82 pagesPreviewpdfDR. RockyNo ratings yet
- Ati RN Community Health Proctored Exam 7 Versions Latest 2020 21 All Correct AnswersDocument35 pagesAti RN Community Health Proctored Exam 7 Versions Latest 2020 21 All Correct Answersolgahuntr827o100% (17)
- Ipcr Final Mon July To December 2023Document2 pagesIpcr Final Mon July To December 2023Jhosie Melchor de GuzmanNo ratings yet
- CHAPTER 5. Terminology in Clinical SettingDocument10 pagesCHAPTER 5. Terminology in Clinical Settingputra bhagasNo ratings yet
- Chakrapani Dasa's Abhinava Chintamani - Early Modern or Post Classical Ayurveda - Jan E.M. HoubenDocument26 pagesChakrapani Dasa's Abhinava Chintamani - Early Modern or Post Classical Ayurveda - Jan E.M. HoubensadabrjNo ratings yet
- Beige and Purple Illustrated Physical Education Physical Fitness Educational PresentationDocument25 pagesBeige and Purple Illustrated Physical Education Physical Fitness Educational PresentationMarco ZoletaNo ratings yet
- PTW - Level 1 Training New Proposal SimonDocument39 pagesPTW - Level 1 Training New Proposal SimonKORAMA KIEN100% (1)
- Model Code of Practice How To Safely Remove AsbestosDocument94 pagesModel Code of Practice How To Safely Remove AsbestosfwvcNo ratings yet
- Test Bank For Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Wilburta Billie Q Lindh Carol D Tamparo Barbara M Dahl Julie Morris Cindy CorreaDocument4 pagesTest Bank For Comprehensive Medical Assisting Administrative and Clinical Competencies 6th Edition Wilburta Billie Q Lindh Carol D Tamparo Barbara M Dahl Julie Morris Cindy Correatrangdatif0No ratings yet
- Emergence Delirium in Pediatric PatientsDocument6 pagesEmergence Delirium in Pediatric PatientsJZ100% (1)
- Emotional Intelligence by GolemanDocument27 pagesEmotional Intelligence by GolemanAli HassanNo ratings yet
- Skripsi Tanpa Bab PembahasanDocument55 pagesSkripsi Tanpa Bab PembahasanUliyatun AwaliyahNo ratings yet
- Hepatitis B: Related ArticlesDocument1 pageHepatitis B: Related ArticlesMicheleFontanaNo ratings yet
- Community Action PlanDocument16 pagesCommunity Action PlanChloegelo MendozaNo ratings yet
- Module in Physical Education 9 (First Quarter, WEEK 1) MelcDocument11 pagesModule in Physical Education 9 (First Quarter, WEEK 1) MelcElton Martin de LeonNo ratings yet
- Malaysia Elderly Care Market Report - Industry Trends and Forecast To 2027 - Data Bridge Market ResearchDocument5 pagesMalaysia Elderly Care Market Report - Industry Trends and Forecast To 2027 - Data Bridge Market ResearchTNNo ratings yet
- Transcript 137 Hashimotos The Root Cause With Dr. Izabella Wentz PDFDocument26 pagesTranscript 137 Hashimotos The Root Cause With Dr. Izabella Wentz PDFPopescu AndreeaNo ratings yet