Download as pdf or txt
You might also like
- Pesticide Applicator Core ManualDocument206 pagesPesticide Applicator Core Manualdodsm100% (2)
- Pasi CalculatorDocument4 pagesPasi CalculatorBimo Aryo TejoNo ratings yet
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakeBoy MadNo ratings yet
- DictationDocument6 pagesDictationlizNo ratings yet
- Psychiatry Student Guide: MEDD 421 Clinical Skills 2019-2020Document25 pagesPsychiatry Student Guide: MEDD 421 Clinical Skills 2019-2020Rubie Ann TillorNo ratings yet
- 2011 09 PsychiatryDocument40 pages2011 09 PsychiatryGurpreet Chara100% (1)
- CVL Consent PDFDocument5 pagesCVL Consent PDFGolam SarwarNo ratings yet
- Geriatric Psychiatry Group CDocument77 pagesGeriatric Psychiatry Group Cchew weijianNo ratings yet
- Dr. Jagdeo Survival ManualDocument16 pagesDr. Jagdeo Survival ManualAli BabaNo ratings yet
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDocument20 pagesPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470No ratings yet
- "It Is More Important To Know The Person With The Illness Than TheDocument21 pages"It Is More Important To Know The Person With The Illness Than TheMuluken TesfayeNo ratings yet
- Consultation-Liaison Psychiatry: Leslie M. Forman, M.D., Neil Scheurich, M.D., and Kristen Tyszkowski, M.DDocument45 pagesConsultation-Liaison Psychiatry: Leslie M. Forman, M.D., Neil Scheurich, M.D., and Kristen Tyszkowski, M.DRayanNo ratings yet
- Lecture No. 3 Semiology of Psychiatry Part 2Document26 pagesLecture No. 3 Semiology of Psychiatry Part 2ozgur.yonlukNo ratings yet
- Template Clerking PsychiatryDocument2 pagesTemplate Clerking Psychiatrymunii28No ratings yet
- Why Psychiatry? Some Thoughts For Medical Students.Document3 pagesWhy Psychiatry? Some Thoughts For Medical Students.Davin TanNo ratings yet
- Terms in The Field of PsychiatryDocument18 pagesTerms in The Field of PsychiatryOchie YecyecanNo ratings yet
- Assessment of DSH & Suicide RiskDocument2 pagesAssessment of DSH & Suicide RiskStudentNo ratings yet
- General Questions (Mood Disorder)Document5 pagesGeneral Questions (Mood Disorder)Zubair MushtaqNo ratings yet
- Mental Status Examination: Table 1-6Document8 pagesMental Status Examination: Table 1-6Đức Nguyên VũNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Psychiatric Visit1 - AaronVer3Document1 pagePsychiatric Visit1 - AaronVer3api-3764308No ratings yet
- PA 644 - M2 LecturesDocument412 pagesPA 644 - M2 LectureskatNo ratings yet
- Psych 9 (Signs and Symptoms)Document5 pagesPsych 9 (Signs and Symptoms)2013SecB100% (1)
- Acute AgitationDocument83 pagesAcute AgitationSamuel FikaduNo ratings yet
- Aggressive Behaviors - ExtendedDocument7 pagesAggressive Behaviors - ExtendedTeresa Silva100% (1)
- Psychiatry Notes - Defenses MechanismsDocument2 pagesPsychiatry Notes - Defenses MechanismsLiSenNo ratings yet
- Translate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeDocument76 pagesTranslate Kaplan Sadock Sinopsis Psikiatri Komprehensif Halaman 721 730 PDF FreeHadi GunaNo ratings yet
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Phase 3a Psychiatry 2021-22Document88 pagesPhase 3a Psychiatry 2021-22Olivia Genevieve El Jassar100% (1)
- Management of AgitationDocument8 pagesManagement of AgitationMahmoud Ahmed Mahmoud100% (1)
- Treatment Resistant OCD .Document55 pagesTreatment Resistant OCD .Dr viren SolankiNo ratings yet
- Se 04 Abpsych PDFDocument27 pagesSe 04 Abpsych PDFBea SengcoNo ratings yet
- Psychiatry ExamDocument4 pagesPsychiatry Examapi-3703352No ratings yet
- Mneumonics PsychDxDocument7 pagesMneumonics PsychDxSuraj MukatiraNo ratings yet
- Psychosomatic SGDocument1 pagePsychosomatic SGkatNo ratings yet
- Generic Normal Psychiatric Established-Patient Med CheckDocument2 pagesGeneric Normal Psychiatric Established-Patient Med CheckkeishaNo ratings yet
- Varun Kumar, 2017 - Getting Started in PsychiatryDocument148 pagesVarun Kumar, 2017 - Getting Started in PsychiatryBernard FZ100% (1)
- Gillman's AD Algorithm - PsychotropicalDocument50 pagesGillman's AD Algorithm - Psychotropicaldo leeNo ratings yet
- Medicines in PregnancyDocument18 pagesMedicines in Pregnancymominur11No ratings yet
- Mental Disorders Due To A General Medical ConditionDocument145 pagesMental Disorders Due To A General Medical ConditionKaye NepomucenoNo ratings yet
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- Psych Ch. 7 Notes (Tutor)Document5 pagesPsych Ch. 7 Notes (Tutor)Haylle ThomasNo ratings yet
- HPI GuidelinesDocument5 pagesHPI GuidelinesHani NadiahNo ratings yet
- Clinical Features of Common Psychiatric DisordersDocument21 pagesClinical Features of Common Psychiatric DisordersShivan A.C.No ratings yet
- Rubric - NRNP 6675Document4 pagesRubric - NRNP 6675Logan ZaraNo ratings yet
- BTB Template Er-IntakeDocument3 pagesBTB Template Er-IntakehectorNo ratings yet
- MC IIIA Topics: Midterm Material. Won't Be in The Final Exam, Only Antiparkinsonian IncludedDocument138 pagesMC IIIA Topics: Midterm Material. Won't Be in The Final Exam, Only Antiparkinsonian IncludedToqa ElmansouryNo ratings yet
- Pharmacotherapy in PschiatryDocument8 pagesPharmacotherapy in PschiatryygfhdgNo ratings yet
- Psychiatry Made EasyDocument14 pagesPsychiatry Made EasyD. W. S JayarathnaNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- Descriptive Psychopathology (Synopsis of Symptoms of The Mind)Document35 pagesDescriptive Psychopathology (Synopsis of Symptoms of The Mind)hungryscribeNo ratings yet
- High Yield Topics For The Shelf - 2022 PsychDocument3 pagesHigh Yield Topics For The Shelf - 2022 PsychTonNo ratings yet
- Pharmacological Management of DepressionDocument66 pagesPharmacological Management of DepressionPriyash JainNo ratings yet
- Study Guide Test 1Document11 pagesStudy Guide Test 1jwasylow13No ratings yet
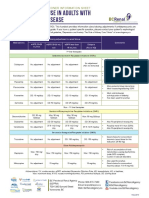
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Clozapine Care GuideDocument16 pagesClozapine Care GuideERWIN SUMARDINo ratings yet
- Emergency Psychiatry: Care in Special SettingsDocument15 pagesEmergency Psychiatry: Care in Special SettingsCassandra BoduchNo ratings yet
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocument8 pagesCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniNo ratings yet
- Psychiatrypoisoning E.ODocument24 pagesPsychiatrypoisoning E.OZeenat JunaidNo ratings yet
- Psych IeDocument10 pagesPsych IeRicah Mae AbingNo ratings yet
- Psych Ch. 5 NotesDocument7 pagesPsych Ch. 5 NotesHaylle ThomasNo ratings yet
- Ebp HandoutDocument2 pagesEbp Handoutapi-543558169No ratings yet
- Oxygen Therapy AdviceDocument38 pagesOxygen Therapy Advicenick_clayton_9No ratings yet
- Approved InstDocument108 pagesApproved Instrajarao001No ratings yet
- Hyperworks Technology Conference (HTC) 2011: Optimization of PMH StructuresDocument25 pagesHyperworks Technology Conference (HTC) 2011: Optimization of PMH StructuresgiakovidNo ratings yet
- Rabbit KeepingDocument12 pagesRabbit KeepingMoses NdwaruNo ratings yet
- Chemical and Nutritional Changes in Food During ExtrusionDocument30 pagesChemical and Nutritional Changes in Food During ExtrusionZubi BaigNo ratings yet
- 3 - Chemical Reactions of Fat and OilsDocument16 pages3 - Chemical Reactions of Fat and Oilssha_bee100% (1)
- GIT InfectionDocument43 pagesGIT InfectionRaja RuzannaNo ratings yet
- Factor Affecting The Development of FetusDocument8 pagesFactor Affecting The Development of FetusWhye Jun CheongNo ratings yet
- Practice 9-10-11Document12 pagesPractice 9-10-11cheplit123No ratings yet
- Green Light Surgical GuideDocument88 pagesGreen Light Surgical GuidekbrinaldiNo ratings yet
- New Lipid PowerpointDocument113 pagesNew Lipid PowerpointMadane Jamila Amerol SaminNo ratings yet
- ComplaintDocument52 pagesComplaintmarwaNo ratings yet
- Impact of Covid19 On The Indian Stock MarketDocument6 pagesImpact of Covid19 On The Indian Stock MarketB31 Viraj PatilNo ratings yet
- 1574-Article Text-2641-1-10-20181107Document5 pages1574-Article Text-2641-1-10-20181107Faraz HaiderNo ratings yet
- The Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateDocument5 pagesThe Effects of Emotion On Short-Term Power Spectrum Analysis of Heart RateManuel Guerrero GómezNo ratings yet
- HPLC Article - 1Document8 pagesHPLC Article - 1akkimipadmaNo ratings yet
- Celebrating Worthing College 2012 SpeadsDocument9 pagesCelebrating Worthing College 2012 SpeadsWorthing College-SportNo ratings yet
- ACTIVITY Psychological First Aid PFADocument25 pagesACTIVITY Psychological First Aid PFAChristine DianeNo ratings yet
- Readings On Human Development of NepalDocument310 pagesReadings On Human Development of NepalBirkha B PunNo ratings yet
- Monthly Report Bundle 2021Document55 pagesMonthly Report Bundle 2021Don alewoh7No ratings yet
- For DissertationDocument13 pagesFor DissertationRegi viniciyaNo ratings yet
- Chapter 21 Muscle Blood FlowDocument17 pagesChapter 21 Muscle Blood Flowelmedina omeragicNo ratings yet
- Jsa For Radiography WorkDocument2 pagesJsa For Radiography WorkVipul ShankarNo ratings yet
- Post Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MDocument3 pagesPost Partum Psychosis Nursing Diagnosis: Aurelio, Lyca Mae MLyca Mae AurelioNo ratings yet
- Illuminating The Aura of Nostalgia: Perceptions of Time, Place, and Identity (ANASTASIA PLATOFF)Document33 pagesIlluminating The Aura of Nostalgia: Perceptions of Time, Place, and Identity (ANASTASIA PLATOFF)Anastasia PlatoffNo ratings yet
- Anthropometry For ElderlyDocument20 pagesAnthropometry For ElderlyjarvantaraNo ratings yet
- Mindfulness: The Big IdeasDocument6 pagesMindfulness: The Big IdeasLuis AndradeNo ratings yet