Download as pdf or txt
You might also like
- Perevod Natalya VasilevnaDocument186 pagesPerevod Natalya Vasilevnamohammad farooque razaa71% (7)
- Vitreous MicrosurgeryDocument271 pagesVitreous Microsurgerybajo0550% (2)
- HydralazineDocument1 pageHydralazineIvanne Hisoler75% (8)
- Anti HTNDocument59 pagesAnti HTNzaha shamseerNo ratings yet
- HYPERTENSION Priya FINAL PPT 2Document14 pagesHYPERTENSION Priya FINAL PPT 2Priya Tiwari100% (1)
- Pad HPNDocument137 pagesPad HPNpmm21d229No ratings yet
- Anti Hypertensive DrugsDocument40 pagesAnti Hypertensive DrugsjawadNo ratings yet
- Antihypertensive Drugs RTDocument41 pagesAntihypertensive Drugs RTMaherNo ratings yet
- Hyper and Hypoaldosteronism - G1Document39 pagesHyper and Hypoaldosteronism - G1Jazh AyochokNo ratings yet
- Anti Hypertensive DrugsDocument113 pagesAnti Hypertensive DrugsRobert DowneyNo ratings yet
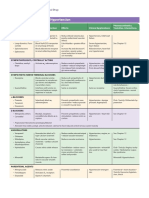
- Chapter 11 Antihypertensive AgentsDocument11 pagesChapter 11 Antihypertensive AgentsChristine Annmarie TapawanNo ratings yet
- Antihypertensive Drugs.Document35 pagesAntihypertensive Drugs.Abdul WahabNo ratings yet
- Hypertension 66Document36 pagesHypertension 66rajeswariNo ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- Penanganan Krisis HipertensiDocument36 pagesPenanganan Krisis Hipertensisuho exoNo ratings yet
- HypertensionDocument5 pagesHypertensiontooba hussainNo ratings yet
- Handout 7 Peripheral Vascular Disorders PDFDocument9 pagesHandout 7 Peripheral Vascular Disorders PDFGrape JuiceNo ratings yet
- HypertensionDocument34 pagesHypertensionThảo MyNo ratings yet
- CCFDocument60 pagesCCFVajja SwatiNo ratings yet
- Antihypertensive Agents 2ndDocument40 pagesAntihypertensive Agents 2ndalikhan52612No ratings yet
- Drugs Used in Hypertension: Dr. R. PilvinieneDocument33 pagesDrugs Used in Hypertension: Dr. R. PilvinieneNewteNo ratings yet
- Y7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, GunturDocument33 pagesY7PH0566, Yedla Pradeep Kumar, 4 B.Pharmacy, Cips, Lam, Gunturప్రదీప్ కుమార్100% (4)
- ACE InhibitorsDocument25 pagesACE InhibitorsShihab AlmoliukiNo ratings yet
- Anti HypertensivesDocument23 pagesAnti HypertensivesLeena AlateeqNo ratings yet
- HTN JmiDocument39 pagesHTN Jmink999999No ratings yet
- Penatalaksanaan Penyulit Gagal JantungDocument17 pagesPenatalaksanaan Penyulit Gagal JantungarumNo ratings yet
- AntihipertensiDocument39 pagesAntihipertensiHarri HardiNo ratings yet
- Review of Advancements in Heart Failure 81220Document65 pagesReview of Advancements in Heart Failure 81220Dr MustafaNo ratings yet
- CVS AgentsDocument25 pagesCVS Agentsanon_925247980No ratings yet
- Pharmacology Semi FinalsDocument269 pagesPharmacology Semi FinalsTrishaNo ratings yet
- Department of Clinical Pharmacology: Pharmacotherapy of Chronic Ischemic Heart DiseaseDocument84 pagesDepartment of Clinical Pharmacology: Pharmacotherapy of Chronic Ischemic Heart DiseasePatty ReyesNo ratings yet
- Antihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DDocument28 pagesAntihypotensive Drugs: Roger Joseph Ii Ramos Jecino, RN, M.DFranz Earl Niño AlbesaNo ratings yet
- Pharmacology of Disopyramide: Yosephine A. H. 020100058Document20 pagesPharmacology of Disopyramide: Yosephine A. H. 020100058zulfantri1983No ratings yet
- HypertensionDocument58 pagesHypertensionSHAHALOMGIR AHMEDNo ratings yet
- Anaphylaxis Suman Mam 2015Document47 pagesAnaphylaxis Suman Mam 2015Parvathy R NairNo ratings yet
- Dr. Bambang Tridjaja - Hyponatremia Endocrin ApproachDocument42 pagesDr. Bambang Tridjaja - Hyponatremia Endocrin ApproachayushintamahaputriNo ratings yet
- Pharmacology of Anti Hypertensive Agents (For BPT Students)Document17 pagesPharmacology of Anti Hypertensive Agents (For BPT Students)Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Dr.M.Kannan MD DA Professor and HOD of Anaesthesiology Tirunelveli Medical CollegeDocument26 pagesDr.M.Kannan MD DA Professor and HOD of Anaesthesiology Tirunelveli Medical CollegeAlina CiubotariuNo ratings yet
- Oral Anti-Htn MedicationsDocument84 pagesOral Anti-Htn Medicationsأبوأحمد الحكيمNo ratings yet
- High AlertDocument61 pagesHigh Alertdrsidra.mustafaNo ratings yet
- Diagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaDocument51 pagesDiagnosis and Management of Shock: Dr. Nurkhalis, SPJP, FihaHilmaNo ratings yet
- Hypertension FinalDocument54 pagesHypertension FinalPatrick CommettantNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- 15 - CCLS - PharmacologyDocument32 pages15 - CCLS - PharmacologyVENKATESH RAMSALINo ratings yet
- Antihypertensive DrugsDocument37 pagesAntihypertensive Drugsleiann_jessicaNo ratings yet
- Drugs Acting On Cardiovascular SystemDocument81 pagesDrugs Acting On Cardiovascular SystemevaNo ratings yet
- Toxicology Cases: Tom Heaps Consultant Acute PhysicianDocument34 pagesToxicology Cases: Tom Heaps Consultant Acute PhysiciandrusmansaleemNo ratings yet
- CVD and HTNDocument60 pagesCVD and HTNZsazsa100% (1)
- Antihypertensive AgentsDocument97 pagesAntihypertensive AgentsL2 - MAKILALA, Zion joy B.No ratings yet
- Anaesthesia Diabetes NotesDocument103 pagesAnaesthesia Diabetes Notesnandhumydad123No ratings yet
- Young Hypertension FinalDocument27 pagesYoung Hypertension FinalMiyuru HasarangaNo ratings yet
- Cardio DrugsDocument68 pagesCardio DrugsIconMaicoNo ratings yet
- Diagnosis and Management of HypertensionDocument55 pagesDiagnosis and Management of HypertensionDanaTyastriNo ratings yet
- Hipertensi KrisisDocument30 pagesHipertensi KrisisLuthfan HakimNo ratings yet
- DiureticsDocument33 pagesDiureticskamalotus135No ratings yet
- Pharmacotherapy IN Cadiovascular Disease: Dept - Pharmacology & Toxicology Faculty of Medicine G M UDocument46 pagesPharmacotherapy IN Cadiovascular Disease: Dept - Pharmacology & Toxicology Faculty of Medicine G M UKHoiry As ShoBirinNo ratings yet
- 19BCPDocument64 pages19BCPNinna Isabel VictorioNo ratings yet
- General Measure in The Management of PoisoningDocument43 pagesGeneral Measure in The Management of PoisoningCharlotte Anne Villero TiuNo ratings yet
- SUMMARY Drugs Used in HypertensionDocument11 pagesSUMMARY Drugs Used in HypertensionPAULINE ANGELI DIEGONo ratings yet
- Antihypertensive DrugsDocument56 pagesAntihypertensive Drugssultan khabeebNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Critical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Anti-Arrhythmics Study Guide: Critical Care EssentialsNo ratings yet
- Pathophysiology of Hyponatremia in Children: Frontiers in Pediatrics October 2017Document9 pagesPathophysiology of Hyponatremia in Children: Frontiers in Pediatrics October 2017nuhigiartoNo ratings yet
- Circulatory MatchDocument2 pagesCirculatory MatchJinky AydallaNo ratings yet
- Spesifikasi Lung Ventilator - Uvent-T (Turbine)Document4 pagesSpesifikasi Lung Ventilator - Uvent-T (Turbine)Fahri FurqanNo ratings yet
- ChesttubesDocument30 pagesChesttubesapi-2692977900% (1)
- BacteriophagesDocument25 pagesBacteriophagesHamza KhanNo ratings yet
- Oral & Maxillofacial SurgeryDocument3 pagesOral & Maxillofacial SurgeryAamir Bugti0% (1)
- Disaster P1examDocument9 pagesDisaster P1examJushua Opsima RuizNo ratings yet
- Pathophysiological Mechanisms of Root Resorption After Dental TraumaDocument15 pagesPathophysiological Mechanisms of Root Resorption After Dental TraumadianaNo ratings yet
- 24.18.00 - Chikungunya2 DR RAGADocument48 pages24.18.00 - Chikungunya2 DR RAGAjcvh24No ratings yet
- Disorders of Acid Base BalanceDocument1 pageDisorders of Acid Base BalanceLyn Domingo EllaquezNo ratings yet
- Performance Comparison of Two Sysmex Hematology Analyzers: The XN-550 and The XS-1000iDocument12 pagesPerformance Comparison of Two Sysmex Hematology Analyzers: The XN-550 and The XS-1000iEjiwumi A. SNo ratings yet
- Parasitology Question and AnswersDocument22 pagesParasitology Question and Answersofficialmwalusamba100% (1)
- Aquanet LG100 MSDS 21.5.2012Document5 pagesAquanet LG100 MSDS 21.5.2012Alejandra Paz San MartínNo ratings yet
- Clinical Case Quizzes - American Association of Clinical EndocrinologyDocument20 pagesClinical Case Quizzes - American Association of Clinical EndocrinologyNesreden Jemal KedirNo ratings yet
- Blood Groups, Abo and RHDocument6 pagesBlood Groups, Abo and RHromeoenny4154No ratings yet
- SJMC - xi-nCP&HTP - Impaired Skin IntegrityDocument10 pagesSJMC - xi-nCP&HTP - Impaired Skin IntegrityJoy CompetenteNo ratings yet
- Rapid Plasma Reagin (RPR) TestDocument5 pagesRapid Plasma Reagin (RPR) Testkiedd_04100% (3)
- References: Doi Pmid Isbn 978-0-83-858529-0Document6 pagesReferences: Doi Pmid Isbn 978-0-83-858529-0JONATHAN BASTIANNo ratings yet
- Complications of PregnancyDocument33 pagesComplications of PregnancyMilagros Maglasang100% (1)
- Diagnostic TestsDocument3 pagesDiagnostic TestspiggypattyNo ratings yet
- CHN Day 2Document12 pagesCHN Day 2Enrico LavariasNo ratings yet
- Maternal and Child Care Nursing Sample ExamDocument7 pagesMaternal and Child Care Nursing Sample ExamteabagmanNo ratings yet
- Guideline Rabies Prophylaxis PPT PDFDocument49 pagesGuideline Rabies Prophylaxis PPT PDFdarkknightlokNo ratings yet
- Surviving Sepsis After BurnsDocument38 pagesSurviving Sepsis After BurnsjustincruzabelleraNo ratings yet
- Basic Maternity ConceptsDocument14 pagesBasic Maternity ConceptsDivine Grace Arreglo AbingNo ratings yet
- Norman CousinsDocument3 pagesNorman CousinsXochilt Medina100% (1)
- Gap Report Astha HospitalDocument29 pagesGap Report Astha Hospitalronit234No ratings yet