
RituximabInfusions 1
RituximabInfusions 1
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ArticleDocument9 pagesArticleAna Lazar IvanNo ratings yet
- Assault and Facial Soft Tissue InjuriesDocument6 pagesAssault and Facial Soft Tissue InjuriesAna Lazar IvanNo ratings yet
- Elusive Diabetes Control Real World Diabetes Care 2017Document8 pagesElusive Diabetes Control Real World Diabetes Care 2017Ana Lazar IvanNo ratings yet
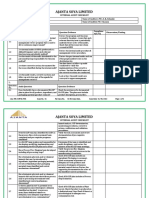
- Diagnosis and Prognosis of Stable Coronary Artery DiseaseDocument55 pagesDiagnosis and Prognosis of Stable Coronary Artery DiseaseAna Lazar IvanNo ratings yet
- Intravenous Fluid Therapy in Adults and ChildrenDocument16 pagesIntravenous Fluid Therapy in Adults and Childrenannisa hayati100% (1)
- Garmin 530W QuickReferenceGuideDocument24 pagesGarmin 530W QuickReferenceGuideLuchohueyNo ratings yet
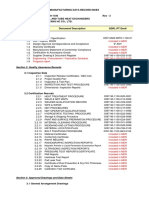
- Internal Audit Checklist Food Safety-MRDocument5 pagesInternal Audit Checklist Food Safety-MRRavi BaghelNo ratings yet
- Application of UV Spectrophotometric Method For Estimation of Iron in Tablet Dosage FormDocument2 pagesApplication of UV Spectrophotometric Method For Estimation of Iron in Tablet Dosage Formahmed ismailNo ratings yet
- Mass Lynx SoftwareDocument94 pagesMass Lynx SoftwareKansy HaikalNo ratings yet
- Rigtools ClampDocument2 pagesRigtools Clampthiban130991No ratings yet
- 1.4 Fourier Transform Technique: 1 1 X 1 1 X X XDocument11 pages1.4 Fourier Transform Technique: 1 1 X 1 1 X X XanaNo ratings yet
- Table of Specification: 2 Grading Period First Summative Test Science 4Document1 pageTable of Specification: 2 Grading Period First Summative Test Science 4Manelyn TagaNo ratings yet
- Lasers in Oral MedicineDocument35 pagesLasers in Oral MedicineShreya singh0% (1)
- Practice 2Document2 pagesPractice 2beebrwNo ratings yet
- Skin Cancer: Mikias Woldetensay Dermatology & Venereology October 2021Document76 pagesSkin Cancer: Mikias Woldetensay Dermatology & Venereology October 2021CHALIE MEQU100% (1)
- Chapter 12Document58 pagesChapter 12reymark ramiterreNo ratings yet
- ON Diesel D2 Russian Gasoil L-0.2-62 Gost 305-82 Contract SpotDocument10 pagesON Diesel D2 Russian Gasoil L-0.2-62 Gost 305-82 Contract Spotdendy alfasaNo ratings yet
- MDRDocument3 pagesMDRjeffreymacasero100% (1)
- Design Process in ElectrochemistryDocument92 pagesDesign Process in ElectrochemistryWulan SariNo ratings yet
- Occlusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsDocument16 pagesOcclusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsHector Flores Soto100% (4)
- What Is A MTE DegreeDocument8 pagesWhat Is A MTE DegreeBonnieNo ratings yet
- CHAPTER 6-10 Level 1Document10 pagesCHAPTER 6-10 Level 1Liana SimionNo ratings yet
- G6 Earth Science Revision Guide - 8Document16 pagesG6 Earth Science Revision Guide - 8Maria JiaNo ratings yet
- CulturalDocument11 pagesCulturalasddsaNo ratings yet
- Beginner Guide - Checklist & Procedures For Ms Flight Simulator by Jaydee 1.23.2Document4 pagesBeginner Guide - Checklist & Procedures For Ms Flight Simulator by Jaydee 1.23.2XBox Aviation100% (1)
- Warning: No Smoking! No Open Flame! While Installing Your Jet KitDocument2 pagesWarning: No Smoking! No Open Flame! While Installing Your Jet KitBrad MonkNo ratings yet
- ARDF DF2020 (D684-17) Parts CatalogDocument32 pagesARDF DF2020 (D684-17) Parts CatalogDumix CataxNo ratings yet
- Programmes For School, Strengthening Environmental Education in School SystemDocument10 pagesProgrammes For School, Strengthening Environmental Education in School SystemRuhi waliaNo ratings yet
- Yaesu Fc757at Instruction ManualDocument28 pagesYaesu Fc757at Instruction ManualAudio TecnologiaNo ratings yet
- Skp-New Price ListDocument26 pagesSkp-New Price ListnuwanwimalNo ratings yet
- Basketball-2 0Document46 pagesBasketball-2 0Catherine EscartinNo ratings yet
- All Rights Reserved. Kim Seng Technical School, 1979Document164 pagesAll Rights Reserved. Kim Seng Technical School, 1979lengyianchua206No ratings yet
- 4.1 Basic Physics and Band Diagrams For MOS CapacitorsDocument5 pages4.1 Basic Physics and Band Diagrams For MOS CapacitorsvinodNo ratings yet
- Astm A184Document3 pagesAstm A184racingspirit800% (1)







































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ArticleDocument9 pagesArticleAna Lazar IvanNo ratings yet
- Assault and Facial Soft Tissue InjuriesDocument6 pagesAssault and Facial Soft Tissue InjuriesAna Lazar IvanNo ratings yet
- Elusive Diabetes Control Real World Diabetes Care 2017Document8 pagesElusive Diabetes Control Real World Diabetes Care 2017Ana Lazar IvanNo ratings yet
- Diagnosis and Prognosis of Stable Coronary Artery DiseaseDocument55 pagesDiagnosis and Prognosis of Stable Coronary Artery DiseaseAna Lazar IvanNo ratings yet
- Intravenous Fluid Therapy in Adults and ChildrenDocument16 pagesIntravenous Fluid Therapy in Adults and Childrenannisa hayati100% (1)
- Garmin 530W QuickReferenceGuideDocument24 pagesGarmin 530W QuickReferenceGuideLuchohueyNo ratings yet
- Internal Audit Checklist Food Safety-MRDocument5 pagesInternal Audit Checklist Food Safety-MRRavi BaghelNo ratings yet
- Application of UV Spectrophotometric Method For Estimation of Iron in Tablet Dosage FormDocument2 pagesApplication of UV Spectrophotometric Method For Estimation of Iron in Tablet Dosage Formahmed ismailNo ratings yet
- Mass Lynx SoftwareDocument94 pagesMass Lynx SoftwareKansy HaikalNo ratings yet
- Rigtools ClampDocument2 pagesRigtools Clampthiban130991No ratings yet
- 1.4 Fourier Transform Technique: 1 1 X 1 1 X X XDocument11 pages1.4 Fourier Transform Technique: 1 1 X 1 1 X X XanaNo ratings yet
- Table of Specification: 2 Grading Period First Summative Test Science 4Document1 pageTable of Specification: 2 Grading Period First Summative Test Science 4Manelyn TagaNo ratings yet
- Lasers in Oral MedicineDocument35 pagesLasers in Oral MedicineShreya singh0% (1)
- Practice 2Document2 pagesPractice 2beebrwNo ratings yet
- Skin Cancer: Mikias Woldetensay Dermatology & Venereology October 2021Document76 pagesSkin Cancer: Mikias Woldetensay Dermatology & Venereology October 2021CHALIE MEQU100% (1)
- Chapter 12Document58 pagesChapter 12reymark ramiterreNo ratings yet
- ON Diesel D2 Russian Gasoil L-0.2-62 Gost 305-82 Contract SpotDocument10 pagesON Diesel D2 Russian Gasoil L-0.2-62 Gost 305-82 Contract Spotdendy alfasaNo ratings yet
- MDRDocument3 pagesMDRjeffreymacasero100% (1)
- Design Process in ElectrochemistryDocument92 pagesDesign Process in ElectrochemistryWulan SariNo ratings yet
- Occlusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsDocument16 pagesOcclusal Vertical Dimension Treatment Planning Decisions and Management ConsiderationsHector Flores Soto100% (4)
- What Is A MTE DegreeDocument8 pagesWhat Is A MTE DegreeBonnieNo ratings yet
- CHAPTER 6-10 Level 1Document10 pagesCHAPTER 6-10 Level 1Liana SimionNo ratings yet
- G6 Earth Science Revision Guide - 8Document16 pagesG6 Earth Science Revision Guide - 8Maria JiaNo ratings yet
- CulturalDocument11 pagesCulturalasddsaNo ratings yet
- Beginner Guide - Checklist & Procedures For Ms Flight Simulator by Jaydee 1.23.2Document4 pagesBeginner Guide - Checklist & Procedures For Ms Flight Simulator by Jaydee 1.23.2XBox Aviation100% (1)
- Warning: No Smoking! No Open Flame! While Installing Your Jet KitDocument2 pagesWarning: No Smoking! No Open Flame! While Installing Your Jet KitBrad MonkNo ratings yet
- ARDF DF2020 (D684-17) Parts CatalogDocument32 pagesARDF DF2020 (D684-17) Parts CatalogDumix CataxNo ratings yet
- Programmes For School, Strengthening Environmental Education in School SystemDocument10 pagesProgrammes For School, Strengthening Environmental Education in School SystemRuhi waliaNo ratings yet
- Yaesu Fc757at Instruction ManualDocument28 pagesYaesu Fc757at Instruction ManualAudio TecnologiaNo ratings yet
- Skp-New Price ListDocument26 pagesSkp-New Price ListnuwanwimalNo ratings yet
- Basketball-2 0Document46 pagesBasketball-2 0Catherine EscartinNo ratings yet
- All Rights Reserved. Kim Seng Technical School, 1979Document164 pagesAll Rights Reserved. Kim Seng Technical School, 1979lengyianchua206No ratings yet
- 4.1 Basic Physics and Band Diagrams For MOS CapacitorsDocument5 pages4.1 Basic Physics and Band Diagrams For MOS CapacitorsvinodNo ratings yet
- Astm A184Document3 pagesAstm A184racingspirit800% (1)