Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- NICU - Policies, Procedures and ProtocolsDocument190 pagesNICU - Policies, Procedures and Protocolskrishnasree100% (3)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Тести, розділені за темамиDocument361 pagesТести, розділені за темамиАнна Олексіївна ГайченкоNo ratings yet
- Management of Epistaxis in Patients On Anti-Platelet And/ or Anticoagulant MedicationDocument6 pagesManagement of Epistaxis in Patients On Anti-Platelet And/ or Anticoagulant MedicationDrGurkirpal Singh MarwahNo ratings yet
- Organic Vapour List PDFDocument1 pageOrganic Vapour List PDFDrGurkirpal Singh MarwahNo ratings yet
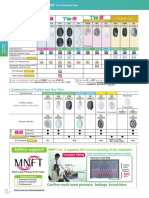
- Reusable & Disposable Respirator For Particle: Japanese Government StandardsDocument1 pageReusable & Disposable Respirator For Particle: Japanese Government StandardsDrGurkirpal Singh MarwahNo ratings yet
- Coulthard 2006Document1 pageCoulthard 2006DrGurkirpal Singh MarwahNo ratings yet
- Reusable Respirator: Particle FilterDocument1 pageReusable Respirator: Particle FilterDrGurkirpal Singh MarwahNo ratings yet
- 1 s2.0 S0901502709009941 MainDocument6 pages1 s2.0 S0901502709009941 MainDrGurkirpal Singh MarwahNo ratings yet
- Code For Identification of Gas-Mask Canisters: United States Department of LaborDocument9 pagesCode For Identification of Gas-Mask Canisters: United States Department of LaborDrGurkirpal Singh MarwahNo ratings yet
- Flexible Contribution Tenure With 25 Years of Protection: HSBC Takaful Future SmartDocument6 pagesFlexible Contribution Tenure With 25 Years of Protection: HSBC Takaful Future SmartmiazainuddinNo ratings yet
- Cerebral Palsy Research PaperDocument6 pagesCerebral Palsy Research Paperapi-354964737No ratings yet
- Best Gallbladder Removal Surgery in Pune - Kaizen Gastro CareDocument3 pagesBest Gallbladder Removal Surgery in Pune - Kaizen Gastro CareKaizen Gastro CareNo ratings yet
- A Study On Molecular Diagnosis of Theileria Species Infection by PCR Amplification in Sheep and Goats in Multan, PakistanDocument10 pagesA Study On Molecular Diagnosis of Theileria Species Infection by PCR Amplification in Sheep and Goats in Multan, PakistanAhmad RazaNo ratings yet
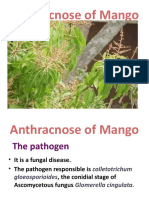
- Anthracnose of MangnoDocument22 pagesAnthracnose of MangnoLINTA JOSEPHNo ratings yet
- TheileriosisDocument10 pagesTheileriosisSomesh SharmaNo ratings yet
- Hypertension CaseDocument3 pagesHypertension CaseArnold Christian QuilonNo ratings yet
- Prevalence of Hypoalbuminemia in Outpatients With HIV/AIDS: ArticleDocument5 pagesPrevalence of Hypoalbuminemia in Outpatients With HIV/AIDS: ArticleMUHAMMAD BAGIR ALJUFRINo ratings yet
- Effectiveness of Proprioceptive Neuromuscular FacilitationDocument4 pagesEffectiveness of Proprioceptive Neuromuscular FacilitationMuhajir AjiNo ratings yet
- Bombay Hospital: Medical CertificateDocument1 pageBombay Hospital: Medical CertificateSandeep ShahNo ratings yet
- اختصارات المندوه ObstetricsDocument11 pagesاختصارات المندوه ObstetricssamyNo ratings yet
- Libro Ciencia y TecnologiaDocument173 pagesLibro Ciencia y TecnologiaLorenzo FuentesNo ratings yet
- MICP211 LEC - CombinedDocument40 pagesMICP211 LEC - CombinedJULIANA NICOLE TUIBUENNo ratings yet
- Clinical Reasoning Assessment For Thinking Effectively CRAFTeDocument4 pagesClinical Reasoning Assessment For Thinking Effectively CRAFTejohn smithNo ratings yet
- Biochemistry Papers MSUDocument20 pagesBiochemistry Papers MSUShiv BhattNo ratings yet
- CAS-GEC04 Module5 Mortality-and-Fertility RPZubietoDocument4 pagesCAS-GEC04 Module5 Mortality-and-Fertility RPZubietoArvie TVNo ratings yet
- AnemiaDocument2 pagesAnemiaLazeh MeNo ratings yet
- Chapter 25 The Child With Cardiovascular DysfunctionDocument20 pagesChapter 25 The Child With Cardiovascular DysfunctionJill Hill100% (3)
- Peripheral Nerve Repair and Reconstruction PDFDocument9 pagesPeripheral Nerve Repair and Reconstruction PDFDea Alberta SNo ratings yet
- Avian InfluenzaDocument9 pagesAvian Influenzajazz100% (1)
- Plagiarism Checker X Originality Report: Similarity Found: 12%Document10 pagesPlagiarism Checker X Originality Report: Similarity Found: 12%Project DevelopmentNo ratings yet
- Vsim Nursing Assignment #1: Toua Xiong 501 Pathophysiology and Pharmacology Gelsey Jian University of Maryland School of Nursing 9/14/18Document7 pagesVsim Nursing Assignment #1: Toua Xiong 501 Pathophysiology and Pharmacology Gelsey Jian University of Maryland School of Nursing 9/14/18Gelsey Gelsinator JianNo ratings yet
- Nhls Handbook 2019Document337 pagesNhls Handbook 2019xhdrv7nvdrNo ratings yet
- Understanding The Circulatory SystemDocument7 pagesUnderstanding The Circulatory SystempiknameripNo ratings yet
- Antibiotics IN Maxillofacial Surgery: Presenter: Dr. Venu G.RDocument92 pagesAntibiotics IN Maxillofacial Surgery: Presenter: Dr. Venu G.RkatnevNo ratings yet
- Max Lab ReportDocument8 pagesMax Lab ReportKallu PrasadNo ratings yet
- Qdoc - Tips Urology Mcqs For Posgraduate ExamDocument62 pagesQdoc - Tips Urology Mcqs For Posgraduate ExamDALIANo ratings yet
- Nausea, Vomiting in Pregnancy & Hyperemesis Gravidarum, UPDATE 2024Document30 pagesNausea, Vomiting in Pregnancy & Hyperemesis Gravidarum, UPDATE 2024patsilwalNo ratings yet