Download as docx, pdf, or txt
You might also like
- Medical Malpractice and NegligenceDocument10 pagesMedical Malpractice and NegligenceT Cel Mrmg100% (3)
- Trucking Company List 2021Document16 pagesTrucking Company List 2021Deep RennovatorsNo ratings yet
- PPM Informed Consent in Anesthesia WITH FORMSDocument10 pagesPPM Informed Consent in Anesthesia WITH FORMSbalab2311No ratings yet
- Medical NegligenceDocument11 pagesMedical NegligenceNimisha100% (1)
- HRM - Thomas CookDocument52 pagesHRM - Thomas CookSabrish Nair50% (2)
- Cheat Sheet FinalDocument4 pagesCheat Sheet FinalSteve BlubaughNo ratings yet
- Medical Law Informed Consent EssayDocument7 pagesMedical Law Informed Consent EssaySaraswathy KrishnanNo ratings yet
- 1 - Rubi Li CaseDocument60 pages1 - Rubi Li Casemartina lopezNo ratings yet
- CHAPTER FOUR Okisor Jo ProjectDocument14 pagesCHAPTER FOUR Okisor Jo ProjectJoseph OkisorNo ratings yet
- 10 Common Medical Malpractice Defense ArgumentsDocument5 pages10 Common Medical Malpractice Defense ArgumentsDanson NdundaNo ratings yet
- 7 Li v. SolimanDocument91 pages7 Li v. SolimanMlaNo ratings yet
- Healthcare Ethics IIDocument202 pagesHealthcare Ethics IIApril ShowersNo ratings yet
- Medical Negligence SampleDocument7 pagesMedical Negligence SampleRajesh ToolseeNo ratings yet
- Professional NegligenceDocument24 pagesProfessional NegligenceCPA OduolNo ratings yet
- Reviewer in Legal Medicine.Document8 pagesReviewer in Legal Medicine.Emil A. MolinaNo ratings yet
- PracticeDocument4 pagesPracticejinny1_0No ratings yet
- Consent Guidance Revised Jan2018Document12 pagesConsent Guidance Revised Jan2018mazin kenziNo ratings yet
- Fwy 026Document27 pagesFwy 026Heronna WilliamsNo ratings yet
- The Ill-InformedDocument29 pagesThe Ill-InformedAspireBooks WorkNo ratings yet
- DR Khoo Lee Seng MD - Legal Medicine (Informed Consent & Failure To Disclose in Plastic Surgery)Document4 pagesDR Khoo Lee Seng MD - Legal Medicine (Informed Consent & Failure To Disclose in Plastic Surgery)Anonymous 8hVpaQdCtrNo ratings yet
- Informed Consent and Contributory Negligence: Litigation, Legislation, and EthicsDocument3 pagesInformed Consent and Contributory Negligence: Litigation, Legislation, and Ethicsgriffone1No ratings yet
- Medical Negligence 2 123Document8 pagesMedical Negligence 2 123Rio vijayNo ratings yet
- Medico Legal - E-Bulletin Vol. 4Document48 pagesMedico Legal - E-Bulletin Vol. 4AmmalNo ratings yet
- HW No. 1 - Canterbury Vs SpenceDocument4 pagesHW No. 1 - Canterbury Vs SpenceAilyn AñanoNo ratings yet
- The Ethics of Medical ReferralDocument3 pagesThe Ethics of Medical Referralkajal907No ratings yet
- 764 - Pdfsam - Anesthesiology 20for 20obstetric 20chesnuts 20 - 20 20translate+pDocument22 pages764 - Pdfsam - Anesthesiology 20for 20obstetric 20chesnuts 20 - 20 20translate+pAnis Eka SukmadadariNo ratings yet
- Major Bioethical PrinciplesDocument44 pagesMajor Bioethical PrinciplesDr. Liza Manalo50% (2)
- Torts - Li Vs SolimanDocument3 pagesTorts - Li Vs SolimanRhea Mae A. SibalaNo ratings yet
- Casumpang vs. Cortejo: - Second DivisionDocument58 pagesCasumpang vs. Cortejo: - Second DivisionsNo ratings yet
- Medical Negligence HandoutDocument3 pagesMedical Negligence Handoutcriskot21No ratings yet
- Ethics ProfessionalDocument47 pagesEthics ProfessionalShael ZoletaNo ratings yet
- Medical Malpractice Philippine JurisprudenceDocument15 pagesMedical Malpractice Philippine JurisprudencellnpdlstNo ratings yet
- 736 - 6. SksDocument10 pages736 - 6. SksIswenti NoveraNo ratings yet
- Medical Malpractice SuitDocument7 pagesMedical Malpractice SuitKevin G. PerezNo ratings yet
- 07 Li V SolimanDocument103 pages07 Li V SolimanJanlo FevidalNo ratings yet
- Legal MedicineDocument14 pagesLegal MedicineSuzanne Pagaduan CruzNo ratings yet
- Medical NegligenceDocument9 pagesMedical NegligencenorashmurmooNo ratings yet
- Torts CIA 1Document5 pagesTorts CIA 1Amayra DixitNo ratings yet
- Eol 5 - Arihan Gupta 1Document5 pagesEol 5 - Arihan Gupta 1api-529369011No ratings yet
- Cobbs v. Grant On Informed ConsentDocument2 pagesCobbs v. Grant On Informed ConsentAldan Subion AvilaNo ratings yet
- Admission Procedure For The Critically Ill PatientDocument3 pagesAdmission Procedure For The Critically Ill Patientgeorgeloto12100% (1)
- Law and MedicineDocument4 pagesLaw and MedicineCP Ispat Unit IINo ratings yet
- It IsDocument4 pagesIt IsANIKET MISHRA 103No ratings yet
- The Principle of Non MaleficenceDocument1 pageThe Principle of Non MaleficenceClaire Esic PontanarNo ratings yet
- Committee (1957) 2 All ER 118 Where He StatedDocument3 pagesCommittee (1957) 2 All ER 118 Where He StatedPutri NabilaNo ratings yet
- Good Medical Practice: September 2018Document49 pagesGood Medical Practice: September 2018gabrielNo ratings yet
- Patient EducationDocument3 pagesPatient EducationNicelle SantiagoNo ratings yet
- Guidelines For ConsentDocument4 pagesGuidelines For ConsentYwagar YwagarNo ratings yet
- JORAMDocument15 pagesJORAMAllan Ssebuyira KiweesiNo ratings yet
- Medical Negligence: 1) Existence of Legal Duty: Whenever A Person Approaches Another Trusting Him To Possess CertainDocument7 pagesMedical Negligence: 1) Existence of Legal Duty: Whenever A Person Approaches Another Trusting Him To Possess Certainshruti singhNo ratings yet
- Ethical Issues in Palliative CareDocument16 pagesEthical Issues in Palliative CarevassalliNo ratings yet
- California Informed Consent For Urine Drug Testing of OB Patients PDFDocument3 pagesCalifornia Informed Consent For Urine Drug Testing of OB Patients PDFThee Lesserof TwoevilsNo ratings yet
- Bioethics Final ReviewerDocument7 pagesBioethics Final ReviewerJeizel IgnacioNo ratings yet
- Lesson 13Document108 pagesLesson 13Rizalyn Padua ReyNo ratings yet
- Article - Medical NegligenceDocument4 pagesArticle - Medical NegligenceSimon RajNo ratings yet
- 08 PDFDocument16 pages08 PDFMădălina RădulescuNo ratings yet
- WWW - Eastzonemedic WWW - Eastzonemedico .In: Helpline No 7549489999Document15 pagesWWW - Eastzonemedic WWW - Eastzonemedico .In: Helpline No 7549489999Anonymous YPAsyOtNo ratings yet
- Clinical Negligence Made Clear: A Guide for Patients and ProfessionalsFrom EverandClinical Negligence Made Clear: A Guide for Patients and ProfessionalsRating: 5 out of 5 stars5/5 (1)
- Correctional Nurse Legal Briefs: Important Information to Keep You Out of Court!From EverandCorrectional Nurse Legal Briefs: Important Information to Keep You Out of Court!No ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- Profil Company 2017Document10 pagesProfil Company 2017Eno Ronaldfrank OguriNo ratings yet
- 170989-Article Text-439183-1-10-20180515Document6 pages170989-Article Text-439183-1-10-20180515mehwish maqboolNo ratings yet
- Catalog IDSI 3Document186 pagesCatalog IDSI 3Adrian OprisanNo ratings yet
- Reason Report: President's LetterDocument8 pagesReason Report: President's LetterreasonorgNo ratings yet
- Does Corporate Social Responsibility Disclosure Improve Firm Investment Efficiency? Evidence From ChinaDocument32 pagesDoes Corporate Social Responsibility Disclosure Improve Firm Investment Efficiency? Evidence From ChinaNi Luh Lemi Sushmita DeviNo ratings yet
- Education Research and Development 9sometimes Called ResearchDocument4 pagesEducation Research and Development 9sometimes Called ResearchFirmanNo ratings yet
- Localization and InternationalizationDocument34 pagesLocalization and InternationalizationalexnekitaNo ratings yet
- Demosthenes, Speeches 1-17Document364 pagesDemosthenes, Speeches 1-17silviudx100% (1)
- Quality of Work Life in Selected Public Universities in Dar Es Salaam, TanzaniaDocument6 pagesQuality of Work Life in Selected Public Universities in Dar Es Salaam, TanzaniaInternational Journal of Arts, Humanities and Social Studies (IJAHSS)No ratings yet
- Stokan 7 - 13 SeptemberDocument25 pagesStokan 7 - 13 SeptemberNovianti Sri WahyuniNo ratings yet
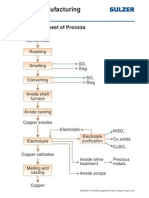
- Copper Manufacturing Process: General Flowsheet of ProcessDocument28 pagesCopper Manufacturing Process: General Flowsheet of ProcessflaviosazevedoNo ratings yet
- Beginners' Guide On How To Become A Successful InvestorDocument51 pagesBeginners' Guide On How To Become A Successful InvestorAoButterflyNo ratings yet
- Newly Hired Teachers Lived Experiences in Classroom Management During The Full Face-to-Face Classes in The New Normal: A PhenomenologyDocument9 pagesNewly Hired Teachers Lived Experiences in Classroom Management During The Full Face-to-Face Classes in The New Normal: A PhenomenologyPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Autopsy Report of Phoenix RiverDocument17 pagesAutopsy Report of Phoenix RiverAnn MirNo ratings yet
- Artikel 13 Hak Dan Kewajiban Anak Terhadap Orang TuaDocument12 pagesArtikel 13 Hak Dan Kewajiban Anak Terhadap Orang TuaMuhammad Irfan SaputraNo ratings yet
- Fortinet Brand Guidelines Partnerv2.3Document13 pagesFortinet Brand Guidelines Partnerv2.3Betiana BoikoNo ratings yet
- SAMPLE LESSON PLAN FOR 5es IN TEACHING SCIENCE PDFDocument4 pagesSAMPLE LESSON PLAN FOR 5es IN TEACHING SCIENCE PDFMia AstilloNo ratings yet
- A Study On Surveillance Mechanism and Surveillance Techniques in The Securities Market at Apollo Sindhoori Capital Investments LTD, ChennaiDocument95 pagesA Study On Surveillance Mechanism and Surveillance Techniques in The Securities Market at Apollo Sindhoori Capital Investments LTD, ChennaiMythili InnconNo ratings yet
- 170706160718tokyo Cement Company (Lanka) PLC Annual Report 2016-17Document140 pages170706160718tokyo Cement Company (Lanka) PLC Annual Report 2016-17Audithya KahawattaNo ratings yet
- Specification of 1500v 5.1mva Solar Ware Station - RevaDocument15 pagesSpecification of 1500v 5.1mva Solar Ware Station - Revalilama45-1No ratings yet
- Product Description (V100R002 03)Document151 pagesProduct Description (V100R002 03)ghallabalsadehNo ratings yet
- Donau CarbonDocument2 pagesDonau CarbonLim Chee SiangNo ratings yet
- Ieee C37.20.3-2013Document70 pagesIeee C37.20.3-2013damaso taracena100% (2)
- Software ListingDocument5 pagesSoftware ListingStefan RadaNo ratings yet
- Es - Chatta Bakhtawar-Shaheen ColonyDocument3 pagesEs - Chatta Bakhtawar-Shaheen ColonyNida NazNo ratings yet
- Top 10 PCB Assembly Companies in Thailand (Updated 2023)Document13 pagesTop 10 PCB Assembly Companies in Thailand (Updated 2023)jackNo ratings yet
- Jestine Seva - PEModuleWeek5&6Document5 pagesJestine Seva - PEModuleWeek5&6Mike AlbaNo ratings yet
- Social Capital, Civil Society and Development: Francis FukuyamaDocument14 pagesSocial Capital, Civil Society and Development: Francis FukuyamaBruno NeneNo ratings yet