
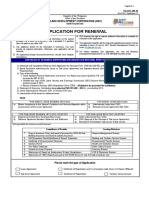
10 - DM SATK Form - Change of Pharmacist or Other Qualified Personnel
10 - DM SATK Form - Change of Pharmacist or Other Qualified Personnel
You might also like
- Informatica Forence 10 2013Document62 pagesInformatica Forence 10 2013Carlos Bernal100% (1)
- 2 - DS SATK Form - Renewal Application of LTO 1.2Document2 pages2 - DS SATK Form - Renewal Application of LTO 1.2Maybielyn David100% (2)
- FDA Circular 2019-001Document4 pagesFDA Circular 2019-001Apple Mae Princess RacpanNo ratings yet
- Revised Application For Renewal FM-CDC-MD-02 As of 2017 Sept 15Document4 pagesRevised Application For Renewal FM-CDC-MD-02 As of 2017 Sept 15Christy SanguyuNo ratings yet
- Invoice: P.T.Evergreen Shipping Agency IndonesiaDocument1 pageInvoice: P.T.Evergreen Shipping Agency IndonesiaDody DermawanNo ratings yet
- J. Carpio-Morales: Surveillance If Such Importations Are Delivered Immediately and For Use Solely Within The SubicDocument3 pagesJ. Carpio-Morales: Surveillance If Such Importations Are Delivered Immediately and For Use Solely Within The SubicTippy Dos SantosNo ratings yet
- Parcor CompuDocument14 pagesParcor CompuErika delos Santos100% (3)
- Change of RPH FormDocument2 pagesChange of RPH FormHapi MedsNo ratings yet
- 9 - DD SATK Form - Change of Pharmacist or Other Qualified Personnel - 10june15Document2 pages9 - DD SATK Form - Change of Pharmacist or Other Qualified Personnel - 10june15BSSNo ratings yet
- 2 - DS SATK Form - Renewal Application of LTO 1.2Document2 pages2 - DS SATK Form - Renewal Application of LTO 1.2Lexi MontanteNo ratings yet
- Renewal Application of LTO 1.2Document2 pagesRenewal Application of LTO 1.2Hazel BisaNo ratings yet
- Center For Drug Regulation and ResearchDocument2 pagesCenter For Drug Regulation and ResearchnetmiNo ratings yet
- RONPD SATK Form Expansion of Establishment 1.3Document2 pagesRONPD SATK Form Expansion of Establishment 1.3ArdenNo ratings yet
- 1 DM SATK Form Initial Application of LTODocument5 pages1 DM SATK Form Initial Application of LTOkhara teanoNo ratings yet
- 7 - DS SATK - Zonal Change in Address 1.2Document2 pages7 - DS SATK - Zonal Change in Address 1.2MCBI AuditorNo ratings yet
- DD SATK Form Change of OwnershipDocument3 pagesDD SATK Form Change of OwnershipMich SantosNo ratings yet
- FDA Lto ChecklistDocument4 pagesFDA Lto ChecklistWillard Lucio100% (1)
- 5 - RONPD SATK Form - Change of Business Name 1.3Document3 pages5 - RONPD SATK Form - Change of Business Name 1.3Kyle Janvier VillaluzNo ratings yet
- 1 DD SATK Form Initial Application of LTODocument4 pages1 DD SATK Form Initial Application of LTOAnonymous i0YU1qCtmNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2Sophia TokieNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2Maan SantiagoNo ratings yet
- Center For Drug Regulation and ResearchDocument3 pagesCenter For Drug Regulation and ResearchStephanie BesanaNo ratings yet
- RONPD SATK Form Initial Application of LTO 1.3Document5 pagesRONPD SATK Form Initial Application of LTO 1.3ArdenNo ratings yet
- 1 - Sponsor CRO SATK Form - Initial Application of LTODocument3 pages1 - Sponsor CRO SATK Form - Initial Application of LTOCzarPaguioNo ratings yet
- Annex C Notification Form MiV NDocument5 pagesAnnex C Notification Form MiV NVincent JosephNo ratings yet
- Self Assessment Form For Sales Promo PermitDocument2 pagesSelf Assessment Form For Sales Promo PermitdoookaNo ratings yet
- Office of The General Accountant: To Be Filled-Up by Officer of The DayDocument5 pagesOffice of The General Accountant: To Be Filled-Up by Officer of The DayRowena Puno-FilomenoNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2cheska yahniiNo ratings yet
- SATKDocument3 pagesSATKArdenNo ratings yet
- Checklist of Requirements For Lto Importer - WholesalerDocument1 pageChecklist of Requirements For Lto Importer - WholesalerJan Kevin GaliciaNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.1Document4 pages1 - DS SATK Form - Initial Application of LTO 1.1Rudejane TanNo ratings yet
- Notification Form and Assessment Report For Tier 1 ApplicationsDocument5 pagesNotification Form and Assessment Report For Tier 1 ApplicationsJemVivarNo ratings yet
- Office of The General Accountant: To Be Filled-Up by Officer of The DayDocument5 pagesOffice of The General Accountant: To Be Filled-Up by Officer of The DayJUCONS ConstructionNo ratings yet
- Retail / Wholesale Drug LicenseDocument3 pagesRetail / Wholesale Drug LicenseRishi DubeyNo ratings yet
- Module 1: Administrative InformationDocument8 pagesModule 1: Administrative InformationRavinder SutariNo ratings yet
- Conditions of RegistrationDocument13 pagesConditions of RegistrationAnkurNo ratings yet
- Toll Manufacturing Fda Requirements: Checklists and FormsDocument8 pagesToll Manufacturing Fda Requirements: Checklists and FormsMiguel PillasNo ratings yet
- Drug Master Files Version UsDocument7 pagesDrug Master Files Version UsDalmy KashiNo ratings yet
- 2018OGAForm Pre-Evaluation Checklist Individual PDFDocument3 pages2018OGAForm Pre-Evaluation Checklist Individual PDFLeizy-Ann Manabat AdrianoNo ratings yet
- Initial Cosmetics TraderDocument4 pagesInitial Cosmetics TradersalemcarolineNo ratings yet
- Pre-Assessment Form of Requirements For Certificate of Medical Device Registration (CMDR) - Class B Legal Requirements 1. Notarized Application FormDocument4 pagesPre-Assessment Form of Requirements For Certificate of Medical Device Registration (CMDR) - Class B Legal Requirements 1. Notarized Application FormEPHRAIM DISTRIBUTORSNo ratings yet
- Co PPDocument15 pagesCo PPVikas JhawatNo ratings yet
- Importation of Cosmetic Products - ResearchDocument6 pagesImportation of Cosmetic Products - ResearchClaire Anne BernardoNo ratings yet
- Importation of Cosmetic ProductsDocument6 pagesImportation of Cosmetic ProductsClaire Anne BernardoNo ratings yet
- Application ProcedureDocument6 pagesApplication ProcedureShibsankar PayraNo ratings yet
- Benefits Settlement Form (Group Plans)Document1 pageBenefits Settlement Form (Group Plans)OG FAMNo ratings yet
- Initial CMDN Class ADocument6 pagesInitial CMDN Class ABalaji ArumugamNo ratings yet
- Procedure To Obtain Drug Manufacturing License (Fresh)Document2 pagesProcedure To Obtain Drug Manufacturing License (Fresh)Jaiprakash SharmaNo ratings yet
- Integrated ApplicationForm (BLANK)Document42 pagesIntegrated ApplicationForm (BLANK)Reggie Theresa MarquezNo ratings yet
- QWP-CDRRHR/LRD-14 Annex 07 Revision No. 01 Date Effective: 15 March 2021Document3 pagesQWP-CDRRHR/LRD-14 Annex 07 Revision No. 01 Date Effective: 15 March 2021EPHRAIM DISTRIBUTORSNo ratings yet
- Office of The General Accountant: Pre-Evaluation Notice Accreditation As An Asset ValuerDocument4 pagesOffice of The General Accountant: Pre-Evaluation Notice Accreditation As An Asset Valuerdenniel DelacruzNo ratings yet
- HFSRB Citizens-Charter-2020Document54 pagesHFSRB Citizens-Charter-2020Jane Therese RoveloNo ratings yet
- Infographic Registration of Pharmaceutical Product For General Sale 637828524496205508Document1 pageInfographic Registration of Pharmaceutical Product For General Sale 637828524496205508Kdp03No ratings yet
- Documents Needed For Gem Portal BidDocument4 pagesDocuments Needed For Gem Portal BidAayush SharmaNo ratings yet
- dc2022 0584Document4 pagesdc2022 0584RMNo ratings yet
- New Dispensing Licence Application FormDocument7 pagesNew Dispensing Licence Application FormkavithaNo ratings yet
- Application To Change RPHDocument2 pagesApplication To Change RPHHapi MedsNo ratings yet
- The FDA PhilippinesDocument5 pagesThe FDA PhilippinesJose Mari Angelo DionioNo ratings yet
- Technical AspectDocument32 pagesTechnical AspectRod Cor FelNo ratings yet
- Checklist of Requirements For Cosmetic LTO Application PDFDocument2 pagesChecklist of Requirements For Cosmetic LTO Application PDFBianca Camille YlingNo ratings yet
- Bizzpaa - Generic MedicineDocument8 pagesBizzpaa - Generic MedicineFITI TechNo ratings yet
- Medical Plan Forensics: Examining the EvidenceFrom EverandMedical Plan Forensics: Examining the EvidenceNo ratings yet
- DELMO, MARK - FINAL EXAMINATION - CIVIL LAW REVIEW I February 12, 2021Document3 pagesDELMO, MARK - FINAL EXAMINATION - CIVIL LAW REVIEW I February 12, 2021Mark Anthony Ruiz DelmoNo ratings yet
- Remedial Law To Be Passed On MondayDocument3 pagesRemedial Law To Be Passed On MondayMark Anthony Ruiz DelmoNo ratings yet
- MTC Vs RTCDocument2 pagesMTC Vs RTCMark Anthony Ruiz DelmoNo ratings yet
- Quiz Corporation Law May 11 2020Document2 pagesQuiz Corporation Law May 11 2020Mark Anthony Ruiz DelmoNo ratings yet
- Parens Patriae Is Inherent in The Supreme Power of The State, Whether ThatDocument3 pagesParens Patriae Is Inherent in The Supreme Power of The State, Whether ThatMark Anthony Ruiz DelmoNo ratings yet
- QUIZZ 5 (May 8, 2020) : Delmo, Mark Anthony R. Law On EvidenceDocument1 pageQUIZZ 5 (May 8, 2020) : Delmo, Mark Anthony R. Law On EvidenceMark Anthony Ruiz DelmoNo ratings yet
- Quiz Corporation Law May 11 2020Document2 pagesQuiz Corporation Law May 11 2020Mark Anthony Ruiz DelmoNo ratings yet
- Legal Forms Quiz May 21 2020 PAUL VINCENT VILLEGASDocument7 pagesLegal Forms Quiz May 21 2020 PAUL VINCENT VILLEGASMark Anthony Ruiz DelmoNo ratings yet
- Delmo, Mark Anthony R. Quiz - Corporation Law May 27, 2020 1Document2 pagesDelmo, Mark Anthony R. Quiz - Corporation Law May 27, 2020 1Mark Anthony Ruiz DelmoNo ratings yet
- Delmo, Mark Anthony R. Quiz - Corporation Law May 4, 2020Document2 pagesDelmo, Mark Anthony R. Quiz - Corporation Law May 4, 2020Mark Anthony Ruiz DelmoNo ratings yet
- CORPORATION-LAW - ExamDocument7 pagesCORPORATION-LAW - ExamMark Anthony Ruiz DelmoNo ratings yet
- People of The PhilippinesDocument3 pagesPeople of The PhilippinesMark Anthony Ruiz DelmoNo ratings yet
- Angular Histograms - Zhao Geng - 2011Document9 pagesAngular Histograms - Zhao Geng - 2011guimanolNo ratings yet
- Japan's Jishu-Bosai-Soshiki Community Activities: Analysis of Its Role in Participatory Community Disaster Risk ManagementDocument12 pagesJapan's Jishu-Bosai-Soshiki Community Activities: Analysis of Its Role in Participatory Community Disaster Risk Managementannette_henderson123No ratings yet
- ZTE UMTS UR15 NodeB Uplink Interference Cancellation Feature GuideDocument34 pagesZTE UMTS UR15 NodeB Uplink Interference Cancellation Feature GuideNiraj Ram ShresthaNo ratings yet
- Presence of Boron in Drinking Water: International Desalination Association BAH03-185Document7 pagesPresence of Boron in Drinking Water: International Desalination Association BAH03-185Jayanath Nuwan SameeraNo ratings yet
- Module 4Document3 pagesModule 4Queenie ValleNo ratings yet
- Mechanics L5 PDFDocument52 pagesMechanics L5 PDFCharlie LaiNo ratings yet
- Shashi - Latest - Sep 2021Document1 pageShashi - Latest - Sep 2021asha peirisNo ratings yet
- Sikafloor®-169: Product Data SheetDocument4 pagesSikafloor®-169: Product Data SheetMohammed AwfNo ratings yet
- 2014-01-15 US (Szymoniak) V American Doc 241-1 Memo MTD JPMCDocument23 pages2014-01-15 US (Szymoniak) V American Doc 241-1 Memo MTD JPMClarry-612445No ratings yet
- Capital Expenditure Control: DR Palash BairagiDocument38 pagesCapital Expenditure Control: DR Palash Bairagisundaram MishraNo ratings yet
- Kenya Supreme Court Justice Njoki Ndung'u's Dissenting VerdictDocument4 pagesKenya Supreme Court Justice Njoki Ndung'u's Dissenting VerdictThe Independent MagazineNo ratings yet
- Rutgers University, Department of Electrical and Computer Engineering Abet Course Syllabus COURSE: 14:332:366Document3 pagesRutgers University, Department of Electrical and Computer Engineering Abet Course Syllabus COURSE: 14:332:366HUANG YINo ratings yet
- Agency Competition AnalysisDocument15 pagesAgency Competition Analysischauhan1983anupamNo ratings yet
- Anexa 2. Eon 25Document11 pagesAnexa 2. Eon 25Alexandra AntonNo ratings yet
- Casing Collar LocatorDocument4 pagesCasing Collar LocatorHammad ShouketNo ratings yet
- Pakistan's Corruption Tsunami: Curse, Contours, Causes, Cost, Challenge and CuresDocument173 pagesPakistan's Corruption Tsunami: Curse, Contours, Causes, Cost, Challenge and CuresPakistan's Corruption100% (3)
- Rent Agreement FormatDocument3 pagesRent Agreement FormatyasinNo ratings yet
- Technical Specification Wooden HousesDocument8 pagesTechnical Specification Wooden HousesNoor MohdNo ratings yet
- Gripping, Prying and TwistingDocument8 pagesGripping, Prying and TwistingLeslie Joy Anastacio VizcarraNo ratings yet
- Governance Modes in Supply Chains and Financial Performance at Buyer, Supplier and Dyadic Levels: The Positive Impact of Power BalanceDocument30 pagesGovernance Modes in Supply Chains and Financial Performance at Buyer, Supplier and Dyadic Levels: The Positive Impact of Power BalancegiovanniNo ratings yet
- Personal MKTG PKG - Part 2 V2Document3 pagesPersonal MKTG PKG - Part 2 V2Lakshya TripathiNo ratings yet
- Geocentric MoonDocument7 pagesGeocentric MoonBob McDonaldNo ratings yet
- M5 Questions and AnswersDocument14 pagesM5 Questions and AnswersAвнιѕнєк SVNo ratings yet
- Chapter 3 Decision TreesDocument12 pagesChapter 3 Decision TreesMark MagumbaNo ratings yet
- Diass-Week 3Document8 pagesDiass-Week 3Gia MarieNo ratings yet
- IIS Interview Questions and AnswersDocument14 pagesIIS Interview Questions and AnswerspallaravisankarNo ratings yet
































































































Download as docx, pdf, or txt
You might also like
- Informatica Forence 10 2013Document62 pagesInformatica Forence 10 2013Carlos Bernal100% (1)
- 2 - DS SATK Form - Renewal Application of LTO 1.2Document2 pages2 - DS SATK Form - Renewal Application of LTO 1.2Maybielyn David100% (2)
- FDA Circular 2019-001Document4 pagesFDA Circular 2019-001Apple Mae Princess RacpanNo ratings yet
- Revised Application For Renewal FM-CDC-MD-02 As of 2017 Sept 15Document4 pagesRevised Application For Renewal FM-CDC-MD-02 As of 2017 Sept 15Christy SanguyuNo ratings yet
- Invoice: P.T.Evergreen Shipping Agency IndonesiaDocument1 pageInvoice: P.T.Evergreen Shipping Agency IndonesiaDody DermawanNo ratings yet
- J. Carpio-Morales: Surveillance If Such Importations Are Delivered Immediately and For Use Solely Within The SubicDocument3 pagesJ. Carpio-Morales: Surveillance If Such Importations Are Delivered Immediately and For Use Solely Within The SubicTippy Dos SantosNo ratings yet
- Parcor CompuDocument14 pagesParcor CompuErika delos Santos100% (3)
- Change of RPH FormDocument2 pagesChange of RPH FormHapi MedsNo ratings yet
- 9 - DD SATK Form - Change of Pharmacist or Other Qualified Personnel - 10june15Document2 pages9 - DD SATK Form - Change of Pharmacist or Other Qualified Personnel - 10june15BSSNo ratings yet
- 2 - DS SATK Form - Renewal Application of LTO 1.2Document2 pages2 - DS SATK Form - Renewal Application of LTO 1.2Lexi MontanteNo ratings yet
- Renewal Application of LTO 1.2Document2 pagesRenewal Application of LTO 1.2Hazel BisaNo ratings yet
- Center For Drug Regulation and ResearchDocument2 pagesCenter For Drug Regulation and ResearchnetmiNo ratings yet
- RONPD SATK Form Expansion of Establishment 1.3Document2 pagesRONPD SATK Form Expansion of Establishment 1.3ArdenNo ratings yet
- 1 DM SATK Form Initial Application of LTODocument5 pages1 DM SATK Form Initial Application of LTOkhara teanoNo ratings yet
- 7 - DS SATK - Zonal Change in Address 1.2Document2 pages7 - DS SATK - Zonal Change in Address 1.2MCBI AuditorNo ratings yet
- DD SATK Form Change of OwnershipDocument3 pagesDD SATK Form Change of OwnershipMich SantosNo ratings yet
- FDA Lto ChecklistDocument4 pagesFDA Lto ChecklistWillard Lucio100% (1)
- 5 - RONPD SATK Form - Change of Business Name 1.3Document3 pages5 - RONPD SATK Form - Change of Business Name 1.3Kyle Janvier VillaluzNo ratings yet
- 1 DD SATK Form Initial Application of LTODocument4 pages1 DD SATK Form Initial Application of LTOAnonymous i0YU1qCtmNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2Sophia TokieNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2Maan SantiagoNo ratings yet
- Center For Drug Regulation and ResearchDocument3 pagesCenter For Drug Regulation and ResearchStephanie BesanaNo ratings yet
- RONPD SATK Form Initial Application of LTO 1.3Document5 pagesRONPD SATK Form Initial Application of LTO 1.3ArdenNo ratings yet
- 1 - Sponsor CRO SATK Form - Initial Application of LTODocument3 pages1 - Sponsor CRO SATK Form - Initial Application of LTOCzarPaguioNo ratings yet
- Annex C Notification Form MiV NDocument5 pagesAnnex C Notification Form MiV NVincent JosephNo ratings yet
- Self Assessment Form For Sales Promo PermitDocument2 pagesSelf Assessment Form For Sales Promo PermitdoookaNo ratings yet
- Office of The General Accountant: To Be Filled-Up by Officer of The DayDocument5 pagesOffice of The General Accountant: To Be Filled-Up by Officer of The DayRowena Puno-FilomenoNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2cheska yahniiNo ratings yet
- SATKDocument3 pagesSATKArdenNo ratings yet
- Checklist of Requirements For Lto Importer - WholesalerDocument1 pageChecklist of Requirements For Lto Importer - WholesalerJan Kevin GaliciaNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.1Document4 pages1 - DS SATK Form - Initial Application of LTO 1.1Rudejane TanNo ratings yet
- Notification Form and Assessment Report For Tier 1 ApplicationsDocument5 pagesNotification Form and Assessment Report For Tier 1 ApplicationsJemVivarNo ratings yet
- Office of The General Accountant: To Be Filled-Up by Officer of The DayDocument5 pagesOffice of The General Accountant: To Be Filled-Up by Officer of The DayJUCONS ConstructionNo ratings yet
- Retail / Wholesale Drug LicenseDocument3 pagesRetail / Wholesale Drug LicenseRishi DubeyNo ratings yet
- Module 1: Administrative InformationDocument8 pagesModule 1: Administrative InformationRavinder SutariNo ratings yet
- Conditions of RegistrationDocument13 pagesConditions of RegistrationAnkurNo ratings yet
- Toll Manufacturing Fda Requirements: Checklists and FormsDocument8 pagesToll Manufacturing Fda Requirements: Checklists and FormsMiguel PillasNo ratings yet
- Drug Master Files Version UsDocument7 pagesDrug Master Files Version UsDalmy KashiNo ratings yet
- 2018OGAForm Pre-Evaluation Checklist Individual PDFDocument3 pages2018OGAForm Pre-Evaluation Checklist Individual PDFLeizy-Ann Manabat AdrianoNo ratings yet
- Initial Cosmetics TraderDocument4 pagesInitial Cosmetics TradersalemcarolineNo ratings yet
- Pre-Assessment Form of Requirements For Certificate of Medical Device Registration (CMDR) - Class B Legal Requirements 1. Notarized Application FormDocument4 pagesPre-Assessment Form of Requirements For Certificate of Medical Device Registration (CMDR) - Class B Legal Requirements 1. Notarized Application FormEPHRAIM DISTRIBUTORSNo ratings yet
- Co PPDocument15 pagesCo PPVikas JhawatNo ratings yet
- Importation of Cosmetic Products - ResearchDocument6 pagesImportation of Cosmetic Products - ResearchClaire Anne BernardoNo ratings yet
- Importation of Cosmetic ProductsDocument6 pagesImportation of Cosmetic ProductsClaire Anne BernardoNo ratings yet
- Application ProcedureDocument6 pagesApplication ProcedureShibsankar PayraNo ratings yet
- Benefits Settlement Form (Group Plans)Document1 pageBenefits Settlement Form (Group Plans)OG FAMNo ratings yet
- Initial CMDN Class ADocument6 pagesInitial CMDN Class ABalaji ArumugamNo ratings yet
- Procedure To Obtain Drug Manufacturing License (Fresh)Document2 pagesProcedure To Obtain Drug Manufacturing License (Fresh)Jaiprakash SharmaNo ratings yet
- Integrated ApplicationForm (BLANK)Document42 pagesIntegrated ApplicationForm (BLANK)Reggie Theresa MarquezNo ratings yet
- QWP-CDRRHR/LRD-14 Annex 07 Revision No. 01 Date Effective: 15 March 2021Document3 pagesQWP-CDRRHR/LRD-14 Annex 07 Revision No. 01 Date Effective: 15 March 2021EPHRAIM DISTRIBUTORSNo ratings yet
- Office of The General Accountant: Pre-Evaluation Notice Accreditation As An Asset ValuerDocument4 pagesOffice of The General Accountant: Pre-Evaluation Notice Accreditation As An Asset Valuerdenniel DelacruzNo ratings yet
- HFSRB Citizens-Charter-2020Document54 pagesHFSRB Citizens-Charter-2020Jane Therese RoveloNo ratings yet
- Infographic Registration of Pharmaceutical Product For General Sale 637828524496205508Document1 pageInfographic Registration of Pharmaceutical Product For General Sale 637828524496205508Kdp03No ratings yet
- Documents Needed For Gem Portal BidDocument4 pagesDocuments Needed For Gem Portal BidAayush SharmaNo ratings yet
- dc2022 0584Document4 pagesdc2022 0584RMNo ratings yet
- New Dispensing Licence Application FormDocument7 pagesNew Dispensing Licence Application FormkavithaNo ratings yet
- Application To Change RPHDocument2 pagesApplication To Change RPHHapi MedsNo ratings yet
- The FDA PhilippinesDocument5 pagesThe FDA PhilippinesJose Mari Angelo DionioNo ratings yet
- Technical AspectDocument32 pagesTechnical AspectRod Cor FelNo ratings yet
- Checklist of Requirements For Cosmetic LTO Application PDFDocument2 pagesChecklist of Requirements For Cosmetic LTO Application PDFBianca Camille YlingNo ratings yet
- Bizzpaa - Generic MedicineDocument8 pagesBizzpaa - Generic MedicineFITI TechNo ratings yet
- Medical Plan Forensics: Examining the EvidenceFrom EverandMedical Plan Forensics: Examining the EvidenceNo ratings yet
- DELMO, MARK - FINAL EXAMINATION - CIVIL LAW REVIEW I February 12, 2021Document3 pagesDELMO, MARK - FINAL EXAMINATION - CIVIL LAW REVIEW I February 12, 2021Mark Anthony Ruiz DelmoNo ratings yet
- Remedial Law To Be Passed On MondayDocument3 pagesRemedial Law To Be Passed On MondayMark Anthony Ruiz DelmoNo ratings yet
- MTC Vs RTCDocument2 pagesMTC Vs RTCMark Anthony Ruiz DelmoNo ratings yet
- Quiz Corporation Law May 11 2020Document2 pagesQuiz Corporation Law May 11 2020Mark Anthony Ruiz DelmoNo ratings yet
- Parens Patriae Is Inherent in The Supreme Power of The State, Whether ThatDocument3 pagesParens Patriae Is Inherent in The Supreme Power of The State, Whether ThatMark Anthony Ruiz DelmoNo ratings yet
- QUIZZ 5 (May 8, 2020) : Delmo, Mark Anthony R. Law On EvidenceDocument1 pageQUIZZ 5 (May 8, 2020) : Delmo, Mark Anthony R. Law On EvidenceMark Anthony Ruiz DelmoNo ratings yet
- Quiz Corporation Law May 11 2020Document2 pagesQuiz Corporation Law May 11 2020Mark Anthony Ruiz DelmoNo ratings yet
- Legal Forms Quiz May 21 2020 PAUL VINCENT VILLEGASDocument7 pagesLegal Forms Quiz May 21 2020 PAUL VINCENT VILLEGASMark Anthony Ruiz DelmoNo ratings yet
- Delmo, Mark Anthony R. Quiz - Corporation Law May 27, 2020 1Document2 pagesDelmo, Mark Anthony R. Quiz - Corporation Law May 27, 2020 1Mark Anthony Ruiz DelmoNo ratings yet
- Delmo, Mark Anthony R. Quiz - Corporation Law May 4, 2020Document2 pagesDelmo, Mark Anthony R. Quiz - Corporation Law May 4, 2020Mark Anthony Ruiz DelmoNo ratings yet
- CORPORATION-LAW - ExamDocument7 pagesCORPORATION-LAW - ExamMark Anthony Ruiz DelmoNo ratings yet
- People of The PhilippinesDocument3 pagesPeople of The PhilippinesMark Anthony Ruiz DelmoNo ratings yet
- Angular Histograms - Zhao Geng - 2011Document9 pagesAngular Histograms - Zhao Geng - 2011guimanolNo ratings yet
- Japan's Jishu-Bosai-Soshiki Community Activities: Analysis of Its Role in Participatory Community Disaster Risk ManagementDocument12 pagesJapan's Jishu-Bosai-Soshiki Community Activities: Analysis of Its Role in Participatory Community Disaster Risk Managementannette_henderson123No ratings yet
- ZTE UMTS UR15 NodeB Uplink Interference Cancellation Feature GuideDocument34 pagesZTE UMTS UR15 NodeB Uplink Interference Cancellation Feature GuideNiraj Ram ShresthaNo ratings yet
- Presence of Boron in Drinking Water: International Desalination Association BAH03-185Document7 pagesPresence of Boron in Drinking Water: International Desalination Association BAH03-185Jayanath Nuwan SameeraNo ratings yet
- Module 4Document3 pagesModule 4Queenie ValleNo ratings yet
- Mechanics L5 PDFDocument52 pagesMechanics L5 PDFCharlie LaiNo ratings yet
- Shashi - Latest - Sep 2021Document1 pageShashi - Latest - Sep 2021asha peirisNo ratings yet
- Sikafloor®-169: Product Data SheetDocument4 pagesSikafloor®-169: Product Data SheetMohammed AwfNo ratings yet
- 2014-01-15 US (Szymoniak) V American Doc 241-1 Memo MTD JPMCDocument23 pages2014-01-15 US (Szymoniak) V American Doc 241-1 Memo MTD JPMClarry-612445No ratings yet
- Capital Expenditure Control: DR Palash BairagiDocument38 pagesCapital Expenditure Control: DR Palash Bairagisundaram MishraNo ratings yet
- Kenya Supreme Court Justice Njoki Ndung'u's Dissenting VerdictDocument4 pagesKenya Supreme Court Justice Njoki Ndung'u's Dissenting VerdictThe Independent MagazineNo ratings yet
- Rutgers University, Department of Electrical and Computer Engineering Abet Course Syllabus COURSE: 14:332:366Document3 pagesRutgers University, Department of Electrical and Computer Engineering Abet Course Syllabus COURSE: 14:332:366HUANG YINo ratings yet
- Agency Competition AnalysisDocument15 pagesAgency Competition Analysischauhan1983anupamNo ratings yet
- Anexa 2. Eon 25Document11 pagesAnexa 2. Eon 25Alexandra AntonNo ratings yet
- Casing Collar LocatorDocument4 pagesCasing Collar LocatorHammad ShouketNo ratings yet
- Pakistan's Corruption Tsunami: Curse, Contours, Causes, Cost, Challenge and CuresDocument173 pagesPakistan's Corruption Tsunami: Curse, Contours, Causes, Cost, Challenge and CuresPakistan's Corruption100% (3)
- Rent Agreement FormatDocument3 pagesRent Agreement FormatyasinNo ratings yet
- Technical Specification Wooden HousesDocument8 pagesTechnical Specification Wooden HousesNoor MohdNo ratings yet
- Gripping, Prying and TwistingDocument8 pagesGripping, Prying and TwistingLeslie Joy Anastacio VizcarraNo ratings yet
- Governance Modes in Supply Chains and Financial Performance at Buyer, Supplier and Dyadic Levels: The Positive Impact of Power BalanceDocument30 pagesGovernance Modes in Supply Chains and Financial Performance at Buyer, Supplier and Dyadic Levels: The Positive Impact of Power BalancegiovanniNo ratings yet
- Personal MKTG PKG - Part 2 V2Document3 pagesPersonal MKTG PKG - Part 2 V2Lakshya TripathiNo ratings yet
- Geocentric MoonDocument7 pagesGeocentric MoonBob McDonaldNo ratings yet
- M5 Questions and AnswersDocument14 pagesM5 Questions and AnswersAвнιѕнєк SVNo ratings yet
- Chapter 3 Decision TreesDocument12 pagesChapter 3 Decision TreesMark MagumbaNo ratings yet
- Diass-Week 3Document8 pagesDiass-Week 3Gia MarieNo ratings yet
- IIS Interview Questions and AnswersDocument14 pagesIIS Interview Questions and AnswerspallaravisankarNo ratings yet