Download as docx, pdf, or txt
You might also like
- Grandpas Farm (Possible Worlds Games) - UV6yOlDocument28 pagesGrandpas Farm (Possible Worlds Games) - UV6yOlhjorhrafnNo ratings yet
- Module 3 Prestressed Concrete DesignDocument17 pagesModule 3 Prestressed Concrete DesignJoy lauria100% (1)
- TMJ Article - FullDocument11 pagesTMJ Article - FullBivian Alexandro CastilloNo ratings yet
- Conf 06 Ron Phelan TMJDocument14 pagesConf 06 Ron Phelan TMJtugurlanNo ratings yet
- Obstetrics Nursing Questions Answer KeyDocument13 pagesObstetrics Nursing Questions Answer Keyicy431100% (2)
- Year Book2008Document790 pagesYear Book2008Patricia GomesNo ratings yet
- Talking Fashion: Pierre Cardin Interviewed by Jan KedvesDocument5 pagesTalking Fashion: Pierre Cardin Interviewed by Jan KedvesJanKedves100% (1)
- Come Once Again and Love PDFDocument338 pagesCome Once Again and Love PDFdemsNo ratings yet
- Temporomandibular Joint Syndrome: Statpearls (Internet)Document16 pagesTemporomandibular Joint Syndrome: Statpearls (Internet)Ana YUNo ratings yet
- Lecture 7Document24 pagesLecture 7dr.sarahmajed23No ratings yet
- TMJ DisorderDocument10 pagesTMJ DisordersmritinarayanNo ratings yet
- Temporomandibular Joint Dysfunction Diane L. Viola Union County College June 14, 2011Document10 pagesTemporomandibular Joint Dysfunction Diane L. Viola Union County College June 14, 2011Diane Bellantoni ViolaNo ratings yet
- Diagnosisand Treatmentof Temporomandibular Disorders: Harry Dym,, Howard IsraelDocument13 pagesDiagnosisand Treatmentof Temporomandibular Disorders: Harry Dym,, Howard IsraelKranti PrajapatiNo ratings yet
- Atm y Dolor Oro FacialDocument20 pagesAtm y Dolor Oro FacialJuan Carlos MeloNo ratings yet
- Copeand Cope TMJDent Nurs 2011Document5 pagesCopeand Cope TMJDent Nurs 2011GINAROSE DEGUZMANNo ratings yet
- New Concepts and Treatment Modalities in Temperomandibular JointDocument5 pagesNew Concepts and Treatment Modalities in Temperomandibular JointAniket PotnisNo ratings yet
- Diagnosis, Treatment and Management of TMJ DisordersDocument5 pagesDiagnosis, Treatment and Management of TMJ DisorderscempapiNo ratings yet
- Ankylosing Apondylitis of Temporomandibular Joint (TMJ) : February 2012Document13 pagesAnkylosing Apondylitis of Temporomandibular Joint (TMJ) : February 2012Billy PeterNo ratings yet
- Temporomandibular Joint Disorders: Presented by D.Ramya Priya CRIDocument55 pagesTemporomandibular Joint Disorders: Presented by D.Ramya Priya CRIRamya PriyaNo ratings yet
- Deep Neck Infections - Treatment and PrognosisDocument9 pagesDeep Neck Infections - Treatment and PrognosisDenis KimNo ratings yet
- Structural and FunctionalDocument26 pagesStructural and FunctionalJoselyn M Sandoval ANo ratings yet
- Updates Clinical: International Association For The Study of PainDocument6 pagesUpdates Clinical: International Association For The Study of PainSuaeni Kurnia WirdaNo ratings yet
- Temporomandibular Disorders: An Overview and Its Association With Parafunctional ActivityDocument72 pagesTemporomandibular Disorders: An Overview and Its Association With Parafunctional ActivityNaveen MohanNo ratings yet
- Pharmacological Therapy in The Management ofDocument11 pagesPharmacological Therapy in The Management ofpedrofar-1No ratings yet
- Concepts of TMD Etiology: Effects On Diagnosis and TreatmentDocument18 pagesConcepts of TMD Etiology: Effects On Diagnosis and TreatmentMAHARANINo ratings yet
- Osteo Art RitisDocument15 pagesOsteo Art RitisMaria Beatriz Solis ValenciaNo ratings yet
- Dentist ContentDocument2 pagesDentist ContentKamal ShantoNo ratings yet
- TMJ DislocationDocument56 pagesTMJ DislocationAlok BhardwajNo ratings yet
- Epidemiology, Diagnosis, and Treatment of Temporomandibular DisordersDocument16 pagesEpidemiology, Diagnosis, and Treatment of Temporomandibular DisordersMarwaAmerNo ratings yet
- Dislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementFrom EverandDislocation of the Temporomandibular Joint: A Guide to Diagnosis and ManagementNigel Shaun MatthewsNo ratings yet
- Etiological Factors of Temporomandibular Joint Disorders: Wolters Kluwer - Medknow PublicationsDocument6 pagesEtiological Factors of Temporomandibular Joint Disorders: Wolters Kluwer - Medknow PublicationsPutri AmaliaNo ratings yet
- Temporomandibular Joint Pain and DysfunctionDocument7 pagesTemporomandibular Joint Pain and DysfunctionAfroyCrusherNo ratings yet
- Articular Disc Displacement Disorders and Its Prosthodontic Management: A Literature ReviewDocument9 pagesArticular Disc Displacement Disorders and Its Prosthodontic Management: A Literature ReviewTopan MuhamadNo ratings yet
- Temporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyDocument60 pagesTemporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyJoseph Eduardo Villar CordovaNo ratings yet
- Temporomandibular Disorders. Part 1 PDFDocument11 pagesTemporomandibular Disorders. Part 1 PDFgunawanmulyana12No ratings yet
- Herb 2006Document7 pagesHerb 2006tatiana_gil_4No ratings yet
- TMJ DisordersDocument30 pagesTMJ DisordersDua'a Ma'an100% (3)
- Presented By:: Dr. MadaanDocument65 pagesPresented By:: Dr. MadaanAngela Williams90% (10)
- Growth and Development of Temporomandibular JointDocument40 pagesGrowth and Development of Temporomandibular JointSadhu AbhijeetNo ratings yet
- Dislocacion ATMDocument12 pagesDislocacion ATMAlbert OliveraNo ratings yet
- Li LBM 4 Blok 18 AnggunDocument8 pagesLi LBM 4 Blok 18 AnggunAnggun Amanda SaveriiaNo ratings yet
- Temporomandibular Disorders and ManagementDocument79 pagesTemporomandibular Disorders and ManagementVijay ChinthaNo ratings yet
- Risk Factors in The Initiation of Condylar Resorption 2013 Seminars in OrthodonticsDocument8 pagesRisk Factors in The Initiation of Condylar Resorption 2013 Seminars in OrthodonticsGisselaMaldonadoNo ratings yet
- 3 3 29 934 PDFDocument7 pages3 3 29 934 PDFrikasaleh10112013No ratings yet
- 5th Stage: - NazhatDocument11 pages5th Stage: - Nazhatعلي صادق جعفرNo ratings yet
- Australian Dental Journal (2020) Temporomandibular Disorder A Practical Guide For Dental Practitioners inDocument9 pagesAustralian Dental Journal (2020) Temporomandibular Disorder A Practical Guide For Dental Practitioners innabila puspitaNo ratings yet
- General Principles of Fractures: Department of Orthopaedic Surgery Liu Xueyong (刘学勇)Document82 pagesGeneral Principles of Fractures: Department of Orthopaedic Surgery Liu Xueyong (刘学勇)Banna Kiran KumarNo ratings yet
- Management of Mandibular FractureDocument13 pagesManagement of Mandibular FractureAnonymous WtgTCQJdNNo ratings yet
- TMJ DisordersDocument20 pagesTMJ DisordersDr. Hesham Zaatar100% (2)
- Clinical Anatomy and Physiology of The Temporomandibular JointDocument8 pagesClinical Anatomy and Physiology of The Temporomandibular JointAmaliNo ratings yet
- TMJ DisordersDocument20 pagesTMJ DisordersREZVANI FARHADNo ratings yet
- TMDDocument170 pagesTMDVinaya Srinivasan100% (2)
- Desordenes Musculo Esqueleticos PDFDocument12 pagesDesordenes Musculo Esqueleticos PDFJuan Carlos MeloNo ratings yet
- Artículo 1Document7 pagesArtículo 1José Manuel Varela SánchezNo ratings yet
- Cranio®: The Journal of Craniomandibular & Sleep PracticeDocument11 pagesCranio®: The Journal of Craniomandibular & Sleep PracticeAnthony VillafañeNo ratings yet
- TMD & Its Role in Orthodontics "TMD An Entity Affecting Every Aspect of Life" A ReviewDocument6 pagesTMD & Its Role in Orthodontics "TMD An Entity Affecting Every Aspect of Life" A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drg. Reza Fajarsyah Putra, SP - BM Prodi Ikg FK Univ YarsiDocument38 pagesDrg. Reza Fajarsyah Putra, SP - BM Prodi Ikg FK Univ YarsiAnggun DwitwinstersNo ratings yet
- Temporomandibular Joint Disordres 2023 FIFTH YEARSDocument30 pagesTemporomandibular Joint Disordres 2023 FIFTH YEARSيسر مكي وهاب المظفرNo ratings yet
- TMJDocument66 pagesTMJmounika50% (2)
- TMD ,,,,,7Document15 pagesTMD ,,,,,7انور الحاجNo ratings yet
- 1200 Walker MelissaDocument55 pages1200 Walker Melissazano_adamNo ratings yet
- Ginglymoarthrodial JointDocument5 pagesGinglymoarthrodial JointŽäíñäb ÄljaÑabìNo ratings yet
- TMJ LiuDocument16 pagesTMJ LiuCLAUDIA ALEJANDRA CORNEJO FLORESNo ratings yet
- Maxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Document24 pagesMaxillofacial Trauma and Management - Dental Ebook & Lecture Notes PDF Download (Studynama - Com - India's Biggest Website For BDS Study Material Downloads)Vinnie SinghNo ratings yet
- Treatment of Long Term Anterior Dislocation of TMJDocument22 pagesTreatment of Long Term Anterior Dislocation of TMJXavir KhanNo ratings yet
- Internal Derangement GoodDocument29 pagesInternal Derangement GoodMohamed ShokryNo ratings yet
- Api 577 Q 114Document31 pagesApi 577 Q 114Mohammed YoussefNo ratings yet
- IDC POS Lab Project Plan 2 2Document471 pagesIDC POS Lab Project Plan 2 2shiramkkNo ratings yet
- Angles and Directions SurveyingDocument23 pagesAngles and Directions SurveyingAbel AmmoNo ratings yet
- A Review Paper On Effect of Input Welding Process Parameters On Structures and Properties of Weld in Submerged Arc Welding ProcessDocument5 pagesA Review Paper On Effect of Input Welding Process Parameters On Structures and Properties of Weld in Submerged Arc Welding ProcessZarif YusufNo ratings yet
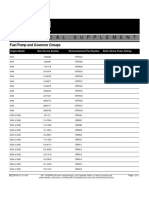
- FuelPump&GovernorGroups SELD0135 11Document11 pagesFuelPump&GovernorGroups SELD0135 11narit00007No ratings yet
- A Concept Paper About LoveDocument5 pagesA Concept Paper About LoveStephen Rivera100% (1)
- Sep. Gravimetrica - CromitaDocument13 pagesSep. Gravimetrica - Cromitaemerson sennaNo ratings yet
- Spare Parts CatalogueDocument45 pagesSpare Parts CatalogueАлексей ДомнинNo ratings yet
- Solutions OSI ExercisesDocument50 pagesSolutions OSI ExercisesHussam AlwareethNo ratings yet
- Mirantis CKA ExamDocument10 pagesMirantis CKA ExamvNo ratings yet
- Floyd Edwrads Memorial Scholarship Terms of Reference 2017Document3 pagesFloyd Edwrads Memorial Scholarship Terms of Reference 2017Aswin HarishNo ratings yet
- McDonald's Vision Statement & Mission Statement Analysis - Panmore InstituteDocument3 pagesMcDonald's Vision Statement & Mission Statement Analysis - Panmore InstituteBorislav FRITZ FrancuskiNo ratings yet
- 2170908Document19 pages2170908bhavikNo ratings yet
- A Project Report On TaxationDocument68 pagesA Project Report On TaxationDinesh ChahalNo ratings yet
- (A3) The Genuine Marks of The Disciples of ChristDocument7 pages(A3) The Genuine Marks of The Disciples of ChristDenmark SaviduriaNo ratings yet
- A Project Report ON A Study On Consumer Satisfaction of PlywoodDocument7 pagesA Project Report ON A Study On Consumer Satisfaction of Plywoodjassi nishadNo ratings yet
- Hoshizaki Technical Support - Warranty Labor Claim InstructionsDocument12 pagesHoshizaki Technical Support - Warranty Labor Claim InstructionsJohn DuttingerNo ratings yet
- Adonis SaturnoDocument6 pagesAdonis SaturnoRaymond G. PanhonNo ratings yet
- Handling Housekeeping RequestsDocument10 pagesHandling Housekeeping RequestsDarlene De PazNo ratings yet
- MCQ-Environmental StudiesDocument45 pagesMCQ-Environmental StudiesShabana Yasmin67% (6)
- 哈佛商业评论 (Harvard Business Review)Document7 pages哈佛商业评论 (Harvard Business Review)h68f9trq100% (1)
- Form MOUDocument4 pagesForm MOUDouglas SugimotoNo ratings yet
- Mole Concept DPP-2 - 501352Document1 pageMole Concept DPP-2 - 501352Vatsal BhargavaNo ratings yet
- A User-Friendly Classification: The Irregular Verbs in EnglishDocument10 pagesA User-Friendly Classification: The Irregular Verbs in EnglishPabloNo ratings yet