Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
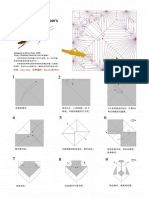
- Brian Chan-Locust PDFDocument10 pagesBrian Chan-Locust PDFdrrahulsshindeNo ratings yet
- Quarterly Oru Folding Diagrams Vol 1Document199 pagesQuarterly Oru Folding Diagrams Vol 1drrahulsshinde95% (20)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 2018 CSB520 ANSWERS Skeletal System PathologyDocument4 pages2018 CSB520 ANSWERS Skeletal System PathologyNathanNo ratings yet
- Quarterly Oru Folding Diagrams - Vol.2Document186 pagesQuarterly Oru Folding Diagrams - Vol.2drrahulsshinde89% (19)
- Tubeless Hypotonic DuodenographyDocument12 pagesTubeless Hypotonic DuodenographydrrahulsshindeNo ratings yet
- Ultrasound Spectrum in Intraductal Papillary Neoplasms of BreastDocument7 pagesUltrasound Spectrum in Intraductal Papillary Neoplasms of BreastdrrahulsshindeNo ratings yet
- Surgical Anatomy PF PNSDocument11 pagesSurgical Anatomy PF PNSdrrahulsshindeNo ratings yet
- 2020 - Management of Recurrent Sebaceous Gland CarcinomaDocument9 pages2020 - Management of Recurrent Sebaceous Gland CarcinomaMikiNo ratings yet
- Nls Diagnostic of Nasopharynx CancerDocument5 pagesNls Diagnostic of Nasopharynx Cancerapi-186101394No ratings yet
- A New Genetic Form of Autism: Antitumor Duality of ApoeDocument1 pageA New Genetic Form of Autism: Antitumor Duality of ApoeMariana CotaNo ratings yet
- Uterine Smooth Muscle Tumors of Unknown Malignant Potential - A Challenging QuestionDocument7 pagesUterine Smooth Muscle Tumors of Unknown Malignant Potential - A Challenging QuestionArt AdibahNo ratings yet
- Motion of A Tumour Cell Under The Blood Flow at Low Reynolds Number in A Curved MicrovesselDocument10 pagesMotion of A Tumour Cell Under The Blood Flow at Low Reynolds Number in A Curved MicrovesselJuana Valentina CamachoNo ratings yet
- It Is Not Always A Cholangiocarcinoma: Unusual Peritoneal Carcinomatosis Revealing Gastric AdenocarcinomaDocument5 pagesIt Is Not Always A Cholangiocarcinoma: Unusual Peritoneal Carcinomatosis Revealing Gastric AdenocarcinomaIJAR JOURNALNo ratings yet
- Eighth Edition of The UICC Classification of Malignant TumoursDocument14 pagesEighth Edition of The UICC Classification of Malignant TumoursСергей СадовниковNo ratings yet
- Phytochemical Analysis in Capsicum SPP.: March 2016Document154 pagesPhytochemical Analysis in Capsicum SPP.: March 2016AbdurrohimnNo ratings yet
- SEER MRCC - ASCO GU 2016 Poster - RaoDocument1 pageSEER MRCC - ASCO GU 2016 Poster - Raoarpit_aiimsNo ratings yet
- Grading and Staging of NeoplasiaDocument13 pagesGrading and Staging of NeoplasiaElvis DuotNo ratings yet
- Skin TumorsDocument357 pagesSkin Tumorscreminelli100% (6)
- PublicationDocument398 pagesPublicationsuci nurjanahNo ratings yet
- Grading and Staging of TumorsDocument11 pagesGrading and Staging of TumorsJahanzaib Bashir100% (1)
- Peri Ampullary TumorDocument69 pagesPeri Ampullary TumorMuhammed Muzzammil SanganiNo ratings yet
- Mucinous Tumors of The Ovary: Current Thoughts On Diagnosis and ManagementDocument9 pagesMucinous Tumors of The Ovary: Current Thoughts On Diagnosis and ManagementKenneth DomasianNo ratings yet
- Con Favre Ux 2018Document29 pagesCon Favre Ux 2018dianpayanganNo ratings yet
- Breast Cancer 1-Prof. Dr. Tarek Abdel Halim El-FayoumiDocument12 pagesBreast Cancer 1-Prof. Dr. Tarek Abdel Halim El-FayoumiYomna HossamNo ratings yet
- Numb Chin Syndrome: A Subtle Clue To Possible Serious IllnessDocument3 pagesNumb Chin Syndrome: A Subtle Clue To Possible Serious IllnessBush HsiehNo ratings yet
- New Gen Dr. Vita OPC Double Layer Tablet 20220727Document26 pagesNew Gen Dr. Vita OPC Double Layer Tablet 20220727Vicky AquinoNo ratings yet
- CA Penis PT1G2Document26 pagesCA Penis PT1G2Anil Kumar GowdaNo ratings yet
- How To Cure Cancer 1Document74 pagesHow To Cure Cancer 1Andres RiveraNo ratings yet
- Us de Tiroides y Ganglios LinfDocument17 pagesUs de Tiroides y Ganglios Linfpruebaprueba321765No ratings yet
- PNLE III For Community Health Nursing and Care of The Mother and Child (Set 1)Document21 pagesPNLE III For Community Health Nursing and Care of The Mother and Child (Set 1)jerarddaria.elakNo ratings yet
- Medicine: Clinical Trial/Experimental StudyDocument10 pagesMedicine: Clinical Trial/Experimental StudyIchaNo ratings yet
- NCM 41118L Final Quiz 3Document13 pagesNCM 41118L Final Quiz 3Matelyn OargaNo ratings yet
- Refrat CA OvariumDocument21 pagesRefrat CA OvariumKurnia SariNo ratings yet
- Q4 - Module 3 Consumer ChemistryDocument23 pagesQ4 - Module 3 Consumer Chemistryjessie100% (2)
- AAO - External Disease and CorneaDocument19 pagesAAO - External Disease and CorneaJohn Paul VillaflorNo ratings yet
- GastroDocument9 pagesGastroAnonymous plYGwXNo ratings yet