Download as pdf or txt
You might also like
- Williams Obstetrics Study Guide, 24th EditionDocument1,013 pagesWilliams Obstetrics Study Guide, 24th EditionKadenceFreya-Charisse G PosadasBulintao90% (20)
- Site Specific Health Safety Environment Plan HvacDocument74 pagesSite Specific Health Safety Environment Plan Hvacsyed khaja misbhuddin100% (1)
- Manual - Facoemulsificador Los DosDocument36 pagesManual - Facoemulsificador Los DosSoporte Técnico ElectronitechNo ratings yet
- Aussie Emergency CareDocument9 pagesAussie Emergency CarePuspita Sari FiazNo ratings yet
- Pod Uveitis Book RevDocument252 pagesPod Uveitis Book Revelika dwi100% (1)
- Standard 2-Family ScenariosDocument13 pagesStandard 2-Family Scenariosapi-249216975No ratings yet
- S.Sharma, Et Al - 2Document4 pagesS.Sharma, Et Al - 2Anonymous QPXAgjBwNo ratings yet
- Caso de EncefalitisDocument4 pagesCaso de EncefalitisJonathan CuevaNo ratings yet
- J Infect Dis. 2012 Ponsford 663 71Document9 pagesJ Infect Dis. 2012 Ponsford 663 71Galant Lefebvre 戈蓝No ratings yet
- A 5 Year Old Boy With Super Refractory Status Epilepticus and RANBP2 Variant WarrantingDocument8 pagesA 5 Year Old Boy With Super Refractory Status Epilepticus and RANBP2 Variant WarrantingAlice MaulisovaNo ratings yet
- Artigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanDocument4 pagesArtigo Neuromeningeal Cryptococcosis in A Patient Not Infected With HumanRENATA SANTOS ASSUNCAONo ratings yet
- Eastern Equine Encephalitis: A Classical Case: Connecticut Medicine October 2014Document4 pagesEastern Equine Encephalitis: A Classical Case: Connecticut Medicine October 2014Chrislyn SanlaoNo ratings yet
- Journal Pre-Proof: IdcasesDocument8 pagesJournal Pre-Proof: IdcasesDaniel GuevaraNo ratings yet
- JurnalDocument4 pagesJurnalGaluh M ArtamtiNo ratings yet
- Cerebral Infarction Pattern in Tuberculous Meningitis: MethodologyDocument10 pagesCerebral Infarction Pattern in Tuberculous Meningitis: MethodologyJanice MuliadiNo ratings yet
- Cerebral Toxoplasmosis: ClinicalpictureDocument2 pagesCerebral Toxoplasmosis: ClinicalpictureRahul RaiNo ratings yet
- HIV Hemicorea CNS Histoplasmosis 2016Document3 pagesHIV Hemicorea CNS Histoplasmosis 2016Juan Salazar PajaresNo ratings yet
- Cerebral Toxoplasmosis - 1Document2 pagesCerebral Toxoplasmosis - 1hasbi.alginaaNo ratings yet
- 72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientDocument7 pages72 - Progressive Multifocal Leukoencephalopathy in An Immunocompetent PatientFaras ArinalNo ratings yet
- The Clinical Syndrome Cerebral MalariaDocument14 pagesThe Clinical Syndrome Cerebral Malaria1130120017 ALI ANTONO TANNo ratings yet
- Cerebral Malaria Immunopathology PDFDocument11 pagesCerebral Malaria Immunopathology PDFAurelia WetondieNo ratings yet
- UKPMC Funders Group: Author ManuscriptDocument20 pagesUKPMC Funders Group: Author ManuscriptHadley AuliaNo ratings yet
- Epilepsy & Behavior Case ReportsDocument4 pagesEpilepsy & Behavior Case ReportsPutu Filla JfNo ratings yet
- Retrospective Analysis of 49 Cases of Brain Abscess and Review of The LiteratureDocument11 pagesRetrospective Analysis of 49 Cases of Brain Abscess and Review of The LiteraturenisaNo ratings yet
- Malaria and StrokeDocument3 pagesMalaria and StrokeRia Septi HarmiaNo ratings yet
- 2011 Virulence 0059 RDocument9 pages2011 Virulence 0059 RHervi LaksariNo ratings yet
- Lee 2007Document6 pagesLee 2007Luis PerezNo ratings yet
- Nej MR A 1216008Document11 pagesNej MR A 1216008guillosarahNo ratings yet
- Combined Treatment of Progressive Encephalitis in An X-Linked Agammaglobulinemia PatientDocument6 pagesCombined Treatment of Progressive Encephalitis in An X-Linked Agammaglobulinemia PatientMaría De Lourdes MartínezNo ratings yet
- 0309 Case 2Document4 pages0309 Case 2willygopeNo ratings yet
- J Neurol Neurosurg Psychiatry-2000-Newton-433-41Document10 pagesJ Neurol Neurosurg Psychiatry-2000-Newton-433-41Joy SanjayaNo ratings yet
- Granulomatous Amebic EncephalitisDocument2 pagesGranulomatous Amebic EncephalitisKristian CadienteNo ratings yet
- Zoo 1Document3 pagesZoo 1nurul rezki fitrianiazisNo ratings yet
- Brain AbcesDocument6 pagesBrain AbcesGintar Isnu WardoyoNo ratings yet
- Infective Endocarditis and Brain Abscess Secondary To Aggregatibacter AphrophilusDocument5 pagesInfective Endocarditis and Brain Abscess Secondary To Aggregatibacter AphrophiluslathifatulNo ratings yet
- Art Acta - Neurol.belgicaDocument6 pagesArt Acta - Neurol.belgicaAna GabrielaNo ratings yet
- Progressive Multifocal Leukoencephalopathy - A Case: Ovidiu Rosca, Elena-Cecilia Rosca, Lucian NegrutiuDocument5 pagesProgressive Multifocal Leukoencephalopathy - A Case: Ovidiu Rosca, Elena-Cecilia Rosca, Lucian Negrutiunoorhadi.n10No ratings yet
- Brain Abscess Potentially Secondary To Odontogenic Infection: CaseDocument4 pagesBrain Abscess Potentially Secondary To Odontogenic Infection: Caseلقمان حنفيNo ratings yet
- Cerebral ToxoplasmaDocument4 pagesCerebral ToxoplasmaTheodoreNo ratings yet
- Tuberculous Meningitis With Initial Manifestation of Isolated Oculomotor Nerve PalsyDocument3 pagesTuberculous Meningitis With Initial Manifestation of Isolated Oculomotor Nerve PalsyRakasiwi GalihNo ratings yet
- Review Article: Cerebral Malaria: A ReviewDocument6 pagesReview Article: Cerebral Malaria: A ReviewAndi Trisnawaty InhaNo ratings yet
- Research ArticleDocument13 pagesResearch ArticlenetifarhatiiNo ratings yet
- Infectious Dan Autoantibody Associated EncephalitisDocument13 pagesInfectious Dan Autoantibody Associated EncephalitisAyudiah ParamitaNo ratings yet
- Immune Reconstitution Inflammatory Syndrome and Cerebral ToxoplasmosisDocument2 pagesImmune Reconstitution Inflammatory Syndrome and Cerebral ToxoplasmosisFirda PotterNo ratings yet
- Encefalitis EquinaDocument8 pagesEncefalitis EquinaAndrésNo ratings yet
- Case Study: A Case of An AIDS Patient With Cryptococcus Neoformans InfectionDocument5 pagesCase Study: A Case of An AIDS Patient With Cryptococcus Neoformans InfectionAdib HaikalNo ratings yet
- Subhyaloid Hemorrhage in Cerebral Malaria: Case ReportDocument4 pagesSubhyaloid Hemorrhage in Cerebral Malaria: Case ReportFaza KahfiNo ratings yet
- Wjarr 2024 1077Document3 pagesWjarr 2024 1077mcvallespinNo ratings yet
- Case Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of ViewDocument4 pagesCase Report: A Case of Herpes Simplex Virus-1 Encephalitis From A Medicolegal Point of Viewzefri suhendarNo ratings yet
- Asymptomatic Mycoplasma Infection Causing Acute Demyelinating Encephalomyelitis: Case Report and Review of LiteratureDocument4 pagesAsymptomatic Mycoplasma Infection Causing Acute Demyelinating Encephalomyelitis: Case Report and Review of Literatureluisalfredo_montesNo ratings yet
- JOURNAL REVIEW Periumbilical Rash in An Immunosupressed IndividualDocument4 pagesJOURNAL REVIEW Periumbilical Rash in An Immunosupressed IndividualVincent ReyesNo ratings yet
- Meningitis Por Angiostrongilus Cantonensis 12974 - 2018 - Article - 1071Document13 pagesMeningitis Por Angiostrongilus Cantonensis 12974 - 2018 - Article - 1071Cristhian RuizNo ratings yet
- JurnalDocument9 pagesJurnalMelita Amalia AyubaNo ratings yet
- Bacterial Brain Abscess: Kevin Patel, MD, and David B. Clifford, MDDocument9 pagesBacterial Brain Abscess: Kevin Patel, MD, and David B. Clifford, MDDayuKurnia DewantiNo ratings yet
- In Deep: Cerebral Toxoplasmosis: Diagnostic DilemmaDocument3 pagesIn Deep: Cerebral Toxoplasmosis: Diagnostic DilemmaYukii Triby-a AnniimesztNo ratings yet
- 2016 Article 174Document8 pages2016 Article 174Alfeus GradyNo ratings yet
- Langerhans Cell Histiocytosis Followed by Folliculotropic Mycosis FungoidesDocument4 pagesLangerhans Cell Histiocytosis Followed by Folliculotropic Mycosis FungoidesYuniita VerayantiiNo ratings yet
- HPV Vaccine Gardasil Crosses Blood-Brain Barrier and Causes Cerebral VasculitisDocument11 pagesHPV Vaccine Gardasil Crosses Blood-Brain Barrier and Causes Cerebral VasculitisMoralVolcano100% (8)
- 278 977 1 SMDocument2 pages278 977 1 SMMohamed MukhrizNo ratings yet
- Case Report... ChamindiDocument5 pagesCase Report... Chamindisajanagamage95No ratings yet
- Annals of Neurology - 2022 - Gollion - Unilateral Leukoencephalopathy Revealing Cerebral Autosomal Dominant ArteriopathyDocument2 pagesAnnals of Neurology - 2022 - Gollion - Unilateral Leukoencephalopathy Revealing Cerebral Autosomal Dominant Arteriopathyalex mondomobeNo ratings yet
- Next Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostDocument4 pagesNext Generation Sequencing of Microbial Cell Free DNA To Rapidly Detect Fluoribacter Bozemanae Pneumonia in An Immunocompromised HostAthenaeum Scientific PublishersNo ratings yet
- Rodgers 2015Document5 pagesRodgers 2015No LimitNo ratings yet
- Importancia de Las Imágenes y El Diagnóstico Etiológico en El Paciente Inmunocomprometido Con Afección Del SNCDocument9 pagesImportancia de Las Imágenes y El Diagnóstico Etiológico en El Paciente Inmunocomprometido Con Afección Del SNCFranciely GarridoNo ratings yet
- Newborn With Meningoencephalitis Proteus MirabilisDocument5 pagesNewborn With Meningoencephalitis Proteus MirabilisRestu TriwulandaniNo ratings yet
- Auto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementFrom EverandAuto-Inflammatory Syndromes: Pathophysiology, Diagnosis, and ManagementPetros EfthimiouNo ratings yet
- Lead and Manage People TTLMDocument41 pagesLead and Manage People TTLMHenok Mehari100% (1)
- Chicago London: Your ItineraryDocument3 pagesChicago London: Your ItineraryZubaidah ZamNo ratings yet
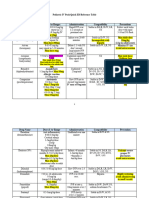
- Pediatric IV Push Quick ED Reference TableDocument4 pagesPediatric IV Push Quick ED Reference TableTayyab RazaNo ratings yet
- The Orgasm Prescription For Women - Andrea Pennington, MD, C.AcDocument54 pagesThe Orgasm Prescription For Women - Andrea Pennington, MD, C.AcNelsonne MampembeNo ratings yet
- Biomedical Waste ManagementDocument22 pagesBiomedical Waste ManagementJayashreeNo ratings yet
- BOM - Chapter 10 - Unilever CaseDocument2 pagesBOM - Chapter 10 - Unilever CaseHuyền HoàngNo ratings yet
- Jurnal Teledentistry 1Document7 pagesJurnal Teledentistry 1Dio Nella ArlinggaNo ratings yet
- Blues CluesDocument24 pagesBlues CluesShy TolentinoNo ratings yet
- 5.2024 Tattoo and PMU Anaesthetic, Repair CreamDocument6 pages5.2024 Tattoo and PMU Anaesthetic, Repair CreamVicente Rogelio Anido RamilNo ratings yet
- CultureandHealth Nupe NigerJMed OleribeDocument2 pagesCultureandHealth Nupe NigerJMed OleribeIdris Aji DaudaNo ratings yet
- Detection of Adulteration of Buffalo and Cow MilkDocument3 pagesDetection of Adulteration of Buffalo and Cow MilkarchanavermaNo ratings yet
- Rural Camp Jan 2016 Report FinalDocument35 pagesRural Camp Jan 2016 Report FinalZEEL PATELNo ratings yet
- Drug Study PreeclampsiaDocument14 pagesDrug Study PreeclampsiaBiway RegalaNo ratings yet
- Vitamin D The Sunshine Vitamin: Dietary SourcesDocument1 pageVitamin D The Sunshine Vitamin: Dietary SourcesjothiNo ratings yet
- France and Saudi ArabiaDocument17 pagesFrance and Saudi ArabiaHajar HossamNo ratings yet
- 2018-089. NASKAH PUBLIKASI Elsi Nursyahdin MayaranaDocument12 pages2018-089. NASKAH PUBLIKASI Elsi Nursyahdin MayaranaElsi NursyahdinNo ratings yet
- Focus3 2E End of Year Test WritingDocument2 pagesFocus3 2E End of Year Test WritingLjhhggNo ratings yet
- Radcliffe EducationDocument4 pagesRadcliffe EducationSherwin Buenavente SulitNo ratings yet
- DisclaimerDocument2 pagesDisclaimergokul gawadeNo ratings yet
- Classification of Proteins and Their Functions PDFDocument1 pageClassification of Proteins and Their Functions PDFConfidentro BlospotNo ratings yet
- Congratulations Gisela Paredes Doctorate of Nurse PractitionerDocument1 pageCongratulations Gisela Paredes Doctorate of Nurse PractitionerAngeloNo ratings yet
- Community Health Nursing Part 1 & 2Document35 pagesCommunity Health Nursing Part 1 & 2mark OrpillaNo ratings yet
- Kuria and MaranyaThe Legal Impunity For Gender Based ViolenceDocument23 pagesKuria and MaranyaThe Legal Impunity For Gender Based ViolenceKelvin NdambiriNo ratings yet
- Loctite Sticker 2Document1 pageLoctite Sticker 2smartitsolution9727No ratings yet