Download as pdf or txt
You might also like
- Cochrane J. H. Asset Pricing Solution 2010Document34 pagesCochrane J. H. Asset Pricing Solution 2010ire04100% (3)
- ESR Verification FormDocument2 pagesESR Verification Formlance tabinas83% (6)
- Theory of Architecture 1Document4 pagesTheory of Architecture 1ramses0% (2)
- Gone With The Wind ScriptDocument71 pagesGone With The Wind ScriptRafael Aleman0% (1)
- This Is A System Generated Letter and Does Not Require Any SignaturesDocument1 pageThis Is A System Generated Letter and Does Not Require Any SignaturesBISHNU BORAL100% (1)
- VBA 21 0960M 10 ARE Muscle InjuriesDocument6 pagesVBA 21 0960M 10 ARE Muscle InjuriesCombat CraigNo ratings yet
- Wrist Conditions Disability Benefits QuestionnaireDocument8 pagesWrist Conditions Disability Benefits QuestionnaireCombat CraigNo ratings yet
- VBA-21-0960M-2-ARE Ankle PDFDocument9 pagesVBA-21-0960M-2-ARE Ankle PDFCombat CraigNo ratings yet
- Vba-21-0960c-9-Are MS PDFDocument9 pagesVba-21-0960c-9-Are MS PDFCombat CraigNo ratings yet
- VBA 21 0960M 9 ARE Knee and Lower LegDocument10 pagesVBA 21 0960M 9 ARE Knee and Lower LegCombat CraigNo ratings yet
- VBA 21 0960M 12 ARE Shoulder and ArmDocument9 pagesVBA 21 0960M 12 ARE Shoulder and ArmCombat CraigNo ratings yet
- VBA-21-0960K-2-ARE Gynecology PDFDocument6 pagesVBA-21-0960K-2-ARE Gynecology PDFCombat CraigNo ratings yet
- VBA-21-0960C-8-ARE Headaches Migraines PDFDocument3 pagesVBA-21-0960C-8-ARE Headaches Migraines PDFCombat CraigNo ratings yet
- VBA-21-0960A-2-ARE Artery and Vein PDFDocument5 pagesVBA-21-0960A-2-ARE Artery and Vein PDFCombat CraigNo ratings yet
- VBA-21-0960J-2-ARE Male Reproductive PDFDocument6 pagesVBA-21-0960J-2-ARE Male Reproductive PDFCombat CraigNo ratings yet
- Vba 21 0960p 3 Are PTSD ReviewDocument6 pagesVba 21 0960p 3 Are PTSD ReviewCombat CraigNo ratings yet
- VBA-21-0960J-4-ARE Urinary PDFDocument4 pagesVBA-21-0960J-4-ARE Urinary PDFCombat CraigNo ratings yet
- VBA 21 0960M 14 ARE ThoracolumbarDocument11 pagesVBA 21 0960M 14 ARE ThoracolumbarCombat CraigNo ratings yet
- Back (Thoracolumbar Spine) Conditions Disability Benefits QuestionnaireDocument11 pagesBack (Thoracolumbar Spine) Conditions Disability Benefits QuestionnaireAnonymous EDHoRBCep3No ratings yet
- Loss of Sense of Smell And/Or Taste Disability Benefits QuestionnaireDocument2 pagesLoss of Sense of Smell And/Or Taste Disability Benefits QuestionnaireSetiawan Prayudha Wilyadana EndhangNo ratings yet
- VBA-21-0960J-3-ARE Prostate Cancer PDFDocument3 pagesVBA-21-0960J-3-ARE Prostate Cancer PDFCombat CraigNo ratings yet
- Vba 21 0960m 13 Are CervicalDocument11 pagesVba 21 0960m 13 Are CervicalCombat CraigNo ratings yet
- VBA-21-0960P-2-ARE Mental Other Than PTSD and EatingDocument5 pagesVBA-21-0960P-2-ARE Mental Other Than PTSD and EatingCombat CraigNo ratings yet
- VBA 21 0960N 3 ARE Sense of SmellDocument2 pagesVBA 21 0960N 3 ARE Sense of SmellCombat CraigNo ratings yet
- VBA-21-0960L-2-ARE Sleep Apnea PDFDocument2 pagesVBA-21-0960L-2-ARE Sleep Apnea PDFCombat CraigNo ratings yet
- Vba-21-0960c-2-Are Als PDFDocument7 pagesVba-21-0960c-2-Are Als PDFCombat CraigNo ratings yet
- VBA-21-0960G-4-ARE Intestinal Surgery PDFDocument3 pagesVBA-21-0960G-4-ARE Intestinal Surgery PDFCombat CraigNo ratings yet
- VBA-21-0960J-1-ARE Kidney PDFDocument5 pagesVBA-21-0960J-1-ARE Kidney PDFCombat CraigNo ratings yet
- VBA-21-0960C-11-ARE Seizure Disorders Epilepsy PDFDocument4 pagesVBA-21-0960C-11-ARE Seizure Disorders Epilepsy PDFCombat CraigNo ratings yet
- CI-08-Other Critical IllnessDocument2 pagesCI-08-Other Critical IllnessAna AzNo ratings yet
- VBA-21-0960C-4-ARE Diabetic Neuropathy PDFDocument5 pagesVBA-21-0960C-4-ARE Diabetic Neuropathy PDFCombat CraigNo ratings yet
- VBA 21 0960Q 1 ARE Chronic Fatigue SyndromeDocument3 pagesVBA 21 0960Q 1 ARE Chronic Fatigue SyndromeCombat CraigNo ratings yet
- VBA-21-0960C-3-ARE Cranial Nerves PDFDocument5 pagesVBA-21-0960C-3-ARE Cranial Nerves PDFCombat CraigNo ratings yet
- CI-08 - Others Critical Illness (Lain-Lain Jenis Penyakit Kritikal)Document2 pagesCI-08 - Others Critical Illness (Lain-Lain Jenis Penyakit Kritikal)nur'afeefa binti hamdanNo ratings yet
- VBA-21-0960G-1-ARE Esophageal GERD PDFDocument4 pagesVBA-21-0960G-1-ARE Esophageal GERD PDFCombat CraigNo ratings yet
- Health Examination Report SECTION 1 (To Be Completed by Candidate) (PART A)Document5 pagesHealth Examination Report SECTION 1 (To Be Completed by Candidate) (PART A)Fifi AinNo ratings yet
- Test Case 3 OASIS - RedactedDocument39 pagesTest Case 3 OASIS - RedactedFernando Galera Jr.No ratings yet
- MDS 3.0 - DzalkjDocument3 pagesMDS 3.0 - DzalkjWiwiNo ratings yet
- VBA-21-0960E-1-ARE Diabetes PDFDocument3 pagesVBA-21-0960E-1-ARE Diabetes PDFCombat CraigNo ratings yet
- Mcu Form International StudentDocument12 pagesMcu Form International StudentJason WongNo ratings yet
- Medical Claim - Doctor StatementDocument3 pagesMedical Claim - Doctor Statement2cqxjrz4gnNo ratings yet
- HMIS 105 Health Unit Outpatient Monthly ReportDocument32 pagesHMIS 105 Health Unit Outpatient Monthly ReportOdette100% (1)
- Joint & Tendon Injection: Coding CornerDocument4 pagesJoint & Tendon Injection: Coding CornerkarkodanNo ratings yet
- ESR Verification Form ReviseDocument4 pagesESR Verification Form ReviseRouella DoverteNo ratings yet
- US Army Medical Course MD0753-101 Book2 - Medical Records Administration BranchDocument101 pagesUS Army Medical Course MD0753-101 Book2 - Medical Records Administration BranchGeorgesNo ratings yet
- VBA-21-0960G-2-ARE Gallbladder Pancreas PDFDocument4 pagesVBA-21-0960G-2-ARE Gallbladder Pancreas PDFCombat CraigNo ratings yet
- Carli2021 Article DeepVeinThrombosisDVTOccurringDocument2 pagesCarli2021 Article DeepVeinThrombosisDVTOccurringAdhe MirnawatiNo ratings yet
- Thoracic Out Let NeurogenicDocument14 pagesThoracic Out Let NeurogenicMisa AjversonNo ratings yet
- ECmed Eval SheetDocument1 pageECmed Eval SheetSalie GuarinoNo ratings yet
- Emt Physical FormDocument1 pageEmt Physical FormLeeann LopezNo ratings yet
- Worksheet in WEHUDocument22 pagesWorksheet in WEHUKeirel EdrinNo ratings yet
- A.I.M.S: Anaesthetic Incident ReportDocument6 pagesA.I.M.S: Anaesthetic Incident ReportvelangniNo ratings yet
- Medical Record Dept.Document32 pagesMedical Record Dept.Kool KingNo ratings yet
- Part Two: ICD-9-CM Official Guidelines (X General RulesDocument24 pagesPart Two: ICD-9-CM Official Guidelines (X General Rulessanpaku2003No ratings yet
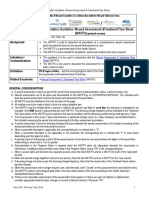
- Documentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)Document4 pagesDocumentation Guideline: Wound Assessment &treatment Flow Sheet (Watfs)eva arna abrarNo ratings yet
- Veterans Hearing Loss Physician EvaluationDocument5 pagesVeterans Hearing Loss Physician Evaluationjim912No ratings yet
- Aefi CifDocument4 pagesAefi CifVic KwanNo ratings yet
- ESR Follow-Up FormDocument2 pagesESR Follow-Up FormAflkjael JamaelNo ratings yet
- Form G Health Examination Report International StudentDocument6 pagesForm G Health Examination Report International StudentVictor OjukwuNo ratings yet
- Ar AllenDocument1 pageAr Allenjocelyn dNo ratings yet
- General Instructions For Canine Trauma Combat Casualty Care Card (CTCCC)Document3 pagesGeneral Instructions For Canine Trauma Combat Casualty Care Card (CTCCC)Felix WinklerNo ratings yet
- Septic ArtritisDocument40 pagesSeptic ArtritisAbiyyuda Naufal PriambodoNo ratings yet
- Medical Coding ICD-10-CM: a QuickStudy Laminated Reference GuideFrom EverandMedical Coding ICD-10-CM: a QuickStudy Laminated Reference GuideNo ratings yet
- Neuroimaging of Covid-19. First Insights based on Clinical CasesFrom EverandNeuroimaging of Covid-19. First Insights based on Clinical CasesSimonetta Gerevini M.D.No ratings yet
- VBA 21 0960Q 1 ARE Chronic Fatigue SyndromeDocument3 pagesVBA 21 0960Q 1 ARE Chronic Fatigue SyndromeCombat CraigNo ratings yet
- Vba 21 0960p 3 Are PTSD ReviewDocument6 pagesVba 21 0960p 3 Are PTSD ReviewCombat CraigNo ratings yet
- VBA-21-0960P-2-ARE Mental Other Than PTSD and EatingDocument5 pagesVBA-21-0960P-2-ARE Mental Other Than PTSD and EatingCombat CraigNo ratings yet
- VBA 21 0960P 1 ARE Eating DisorderDocument2 pagesVBA 21 0960P 1 ARE Eating DisorderCombat CraigNo ratings yet
- VBA-21-0960N-2-ARE EyesDocument10 pagesVBA-21-0960N-2-ARE EyesCombat CraigNo ratings yet
- VBA 21 0960M 12 ARE Shoulder and ArmDocument9 pagesVBA 21 0960M 12 ARE Shoulder and ArmCombat CraigNo ratings yet
- VBA 21 0960N 3 ARE Sense of SmellDocument2 pagesVBA 21 0960N 3 ARE Sense of SmellCombat CraigNo ratings yet
- VBA 21 0960M 14 ARE ThoracolumbarDocument11 pagesVBA 21 0960M 14 ARE ThoracolumbarCombat CraigNo ratings yet
- Wrist Conditions Disability Benefits QuestionnaireDocument8 pagesWrist Conditions Disability Benefits QuestionnaireCombat CraigNo ratings yet
- Vba 21 0960m 13 Are CervicalDocument11 pagesVba 21 0960m 13 Are CervicalCombat CraigNo ratings yet
- VBA-21-0960M-2-ARE Ankle PDFDocument9 pagesVBA-21-0960M-2-ARE Ankle PDFCombat CraigNo ratings yet
- VBA 21 0960M 9 ARE Knee and Lower LegDocument10 pagesVBA 21 0960M 9 ARE Knee and Lower LegCombat CraigNo ratings yet
- VBA 21 0960M 10 ARE Muscle InjuriesDocument6 pagesVBA 21 0960M 10 ARE Muscle InjuriesCombat CraigNo ratings yet
- VBA-21-0960J-4-ARE Urinary PDFDocument4 pagesVBA-21-0960J-4-ARE Urinary PDFCombat CraigNo ratings yet
- VBA-21-0960J-2-ARE Male Reproductive PDFDocument6 pagesVBA-21-0960J-2-ARE Male Reproductive PDFCombat CraigNo ratings yet
- VBA-21-0960L-2-ARE Sleep Apnea PDFDocument2 pagesVBA-21-0960L-2-ARE Sleep Apnea PDFCombat CraigNo ratings yet
- VBA-21-0960M-1-ARE Amputations PDFDocument4 pagesVBA-21-0960M-1-ARE Amputations PDFCombat CraigNo ratings yet
- VBA-21-0960K-2-ARE Gynecology PDFDocument6 pagesVBA-21-0960K-2-ARE Gynecology PDFCombat CraigNo ratings yet
- VBA-21-0960J-3-ARE Prostate Cancer PDFDocument3 pagesVBA-21-0960J-3-ARE Prostate Cancer PDFCombat CraigNo ratings yet
- VBA-21-0960G-4-ARE Intestinal Surgery PDFDocument3 pagesVBA-21-0960G-4-ARE Intestinal Surgery PDFCombat CraigNo ratings yet
- VBA-21-0960F-2-ARE Skin PDFDocument5 pagesVBA-21-0960F-2-ARE Skin PDFCombat CraigNo ratings yet
- VBA-21-0960J-1-ARE Kidney PDFDocument5 pagesVBA-21-0960J-1-ARE Kidney PDFCombat CraigNo ratings yet
- VBA-21-0960G-2-ARE Gallbladder Pancreas PDFDocument4 pagesVBA-21-0960G-2-ARE Gallbladder Pancreas PDFCombat CraigNo ratings yet
- VBA-21-0960G-1-ARE Esophageal GERD PDFDocument4 pagesVBA-21-0960G-1-ARE Esophageal GERD PDFCombat CraigNo ratings yet
- Hagerstown Community College Nursing 229 Clinical Prep CardDocument3 pagesHagerstown Community College Nursing 229 Clinical Prep CardBenNo ratings yet
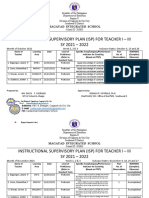
- ISP For Teacher 1Document25 pagesISP For Teacher 1Carlz BrianNo ratings yet
- Creating The Corporate Soul The Rise of Public Relations and Corporate Imagery in American Big Business (Roland Marchand)Document275 pagesCreating The Corporate Soul The Rise of Public Relations and Corporate Imagery in American Big Business (Roland Marchand)Agnes MalkinsonNo ratings yet
- ENG 451 LOTF MCQ Quiz 1 Week 8 PDFDocument6 pagesENG 451 LOTF MCQ Quiz 1 Week 8 PDFSummaira MushtaqNo ratings yet
- Unit 3 - TAKEAWAY Sheets - Activity 1-3: Activity 1: Regional Differences Between The North & South in The Mid-1800sDocument6 pagesUnit 3 - TAKEAWAY Sheets - Activity 1-3: Activity 1: Regional Differences Between The North & South in The Mid-1800sTradconNo ratings yet
- Cost Accounting IDocument147 pagesCost Accounting IBilisummaa LammiiNo ratings yet
- De 3.2Document6 pagesDe 3.2minh trungNo ratings yet
- The Federal Polytechnic, IdahDocument3 pagesThe Federal Polytechnic, Idahwisdomeneojoufedo0147No ratings yet
- 2nd Q QRA-FORM-3BDocument79 pages2nd Q QRA-FORM-3BApril Catadman QuitonNo ratings yet
- Challenges For Management in A Global EnvironmentDocument2 pagesChallenges For Management in A Global EnvironmentLinh Đặng Thị HuyềnNo ratings yet
- David Grumett and Rachel Muers - Theology On The Menu Asceticism, Meat and Christian DietDocument218 pagesDavid Grumett and Rachel Muers - Theology On The Menu Asceticism, Meat and Christian DietAntônio Oliveira100% (1)
- Key Success Strategy of Inbound Tourism Management in Bangkok ThailandDocument12 pagesKey Success Strategy of Inbound Tourism Management in Bangkok ThailandLee Hock SengNo ratings yet
- Read Online Textbook Mistletoe and MR Right Sarah Morgenthaler 2 Ebook All Chapter PDFDocument22 pagesRead Online Textbook Mistletoe and MR Right Sarah Morgenthaler 2 Ebook All Chapter PDFronald.payne460100% (6)
- Works of Defence Act 1903 1Document21 pagesWorks of Defence Act 1903 1Eighteenth JulyNo ratings yet
- Alpha and OmegaDocument9 pagesAlpha and OmegaMark WatsonNo ratings yet
- Conflict 2Document8 pagesConflict 2api-164711099No ratings yet
- Successful Entrepreneur in BangladeshDocument7 pagesSuccessful Entrepreneur in BangladeshRajib AhmedNo ratings yet
- Manager Training & Quality - Chennai - Aegis Customer Support Services Private Limited. - 8 To 12 Years of ExperienceDocument3 pagesManager Training & Quality - Chennai - Aegis Customer Support Services Private Limited. - 8 To 12 Years of ExperienceSelecticaDeepshikha AroraNo ratings yet
- Fuel Tank Monitoring SystemDocument3 pagesFuel Tank Monitoring SystemCALLCOMM FUEL LEVEL SENSOR AND SOLUTIONNo ratings yet
- ASISC Rules and Regulations For Literary EventsDocument6 pagesASISC Rules and Regulations For Literary EventsSahil PahanNo ratings yet
- Multiple Employees Weekly TimesheetDocument7 pagesMultiple Employees Weekly TimesheetLaura ShintaNo ratings yet
- Allen - The Tears of God - Jimmy AllenDocument8 pagesAllen - The Tears of God - Jimmy AllenkyleNo ratings yet
- Law-Of-Negotiable-Instruments - Abrham YohannesDocument171 pagesLaw-Of-Negotiable-Instruments - Abrham YohannesJøñë ÊphrèmNo ratings yet
- MH0414754ENC - PDF Web PDFDocument4 pagesMH0414754ENC - PDF Web PDFEuropean Institute for Gender EqualityNo ratings yet
- June 2009 QP - Unit 2 Edexcel Economics A-LevelDocument30 pagesJune 2009 QP - Unit 2 Edexcel Economics A-LevelStevenNo ratings yet
- Capital Market Structure in IndiaDocument14 pagesCapital Market Structure in IndiaRahul BhattNo ratings yet