
Scabies and Pediculosis
Scabies and Pediculosis
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Oxford Handbooks Download LinkDocument5 pagesOxford Handbooks Download LinkAdithya Vishwanath43% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Buku Manpro Versi IndonesiaDocument375 pagesBuku Manpro Versi IndonesiaTaufan Widiarko100% (3)
- Acquired C1 Inhibitor Deficiencymanagement and PrognosisDocument14 pagesAcquired C1 Inhibitor Deficiencymanagement and PrognosisjalalfaizNo ratings yet
- ACE Inhibitor-Induced AngioedemaDocument14 pagesACE Inhibitor-Induced AngioedemajalalfaizNo ratings yet
- Lichen Planus and Its Management An Update and Observation Ijced 18 001Document5 pagesLichen Planus and Its Management An Update and Observation Ijced 18 001jalalfaizNo ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- Pityriasis RoseaDocument2 pagesPityriasis RoseajalalfaizNo ratings yet
- Lichen Planus: Santa Clara Medical Center, Department of Dermatology #472Document2 pagesLichen Planus: Santa Clara Medical Center, Department of Dermatology #472jalalfaizNo ratings yet
- Acne Keloidalis NuchaeDocument16 pagesAcne Keloidalis NuchaejalalfaizNo ratings yet
- Levamisole in L.PDocument5 pagesLevamisole in L.PjalalfaizNo ratings yet
- Pemphigus: Clinical FeaturesDocument7 pagesPemphigus: Clinical FeaturesjalalfaizNo ratings yet
- WartsDocument5 pagesWartsjalalfaizNo ratings yet
- PemphigoidDocument4 pagesPemphigoidjalalfaizNo ratings yet
- Candidiasis: Clinical FeaturesDocument4 pagesCandidiasis: Clinical FeaturesjalalfaizNo ratings yet
- UrticariaDocument5 pagesUrticariajalalfaizNo ratings yet
- Molluscum ContagiosumDocument2 pagesMolluscum ContagiosumjalalfaizNo ratings yet
- Herpes SimplexDocument5 pagesHerpes SimplexjalalfaizNo ratings yet
- 21 Molluscum Contagiosum PDFDocument2 pages21 Molluscum Contagiosum PDFjalalfaizNo ratings yet
- Tinea (Dermatomycosis)Document9 pagesTinea (Dermatomycosis)jalalfaizNo ratings yet
- Tinea VersicolorDocument2 pagesTinea VersicolorjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- Lichen Simplex ChronicusDocument3 pagesLichen Simplex ChronicusjalalfaizNo ratings yet
- Lupus Vulgaris of External NoseDocument3 pagesLupus Vulgaris of External NosejalalfaizNo ratings yet
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Drug ReactionsDocument11 pagesDrug ReactionsjalalfaizNo ratings yet
- Acne and Acneiform DermatosesDocument5 pagesAcne and Acneiform DermatosesjalalfaizNo ratings yet
- Meralgia Paresthetica: Case PresentationDocument2 pagesMeralgia Paresthetica: Case PresentationjalalfaizNo ratings yet
- I S D, TC, I S: Mechanisms of DiseaseDocument12 pagesI S D, TC, I S: Mechanisms of DiseasejalalfaizNo ratings yet
- Top 30 Skin DiseasesDocument32 pagesTop 30 Skin DiseasesjalalfaizNo ratings yet
- People vs. Umali, 193 SCRA 493, G.R. No. 84450 February 4, 1991Document12 pagesPeople vs. Umali, 193 SCRA 493, G.R. No. 84450 February 4, 1991Trea CheryNo ratings yet
- De Thi Giua Ki 1 Tieng Anh Lop 5 Co Dap An 2021Document28 pagesDe Thi Giua Ki 1 Tieng Anh Lop 5 Co Dap An 2021Đỗ Thanh XuânNo ratings yet
- Portraits of Courage PDF Full Book Online FreeDocument4 pagesPortraits of Courage PDF Full Book Online FreeDark UnicornNo ratings yet
- FM302 Financial Management in The Pacific Region: Week 4: Lecture 7 - Major Assignment Some Discussions and DirectionsDocument15 pagesFM302 Financial Management in The Pacific Region: Week 4: Lecture 7 - Major Assignment Some Discussions and DirectionsHitesh MaharajNo ratings yet
- TMS 3701Document2 pagesTMS 3701nnshabalala290No ratings yet
- Simon The Sportsman: Activity TypeDocument3 pagesSimon The Sportsman: Activity TypeEkaterina DatsenkoNo ratings yet
- In The Supreme Court of Texas: T S T, PDocument14 pagesIn The Supreme Court of Texas: T S T, PLaw&CrimeNo ratings yet
- UE18EE325 - Unit1 - Class4 - Performance Characteristics-StaticDocument16 pagesUE18EE325 - Unit1 - Class4 - Performance Characteristics-StaticGAYATHRI DEVI BNo ratings yet
- Private Files Module 3 Practical Research 2 Conceptual Framework and Hypothesis PDFDocument20 pagesPrivate Files Module 3 Practical Research 2 Conceptual Framework and Hypothesis PDFLovely IñigoNo ratings yet
- Words That HurtDocument5 pagesWords That Hurtsir_leoNo ratings yet
- Aquios LIS Interface SpecificationDocument56 pagesAquios LIS Interface SpecificationLuis AriasNo ratings yet
- The Travels of Macarius, Patriarch of Antioch: Written by his Attendant Archdeacon, Paul of Aleppo, In Arabic. Volume I and II. Translated By F. C. Belfour London: Printed for the Oriental Translation Fund, 1837Document8 pagesThe Travels of Macarius, Patriarch of Antioch: Written by his Attendant Archdeacon, Paul of Aleppo, In Arabic. Volume I and II. Translated By F. C. Belfour London: Printed for the Oriental Translation Fund, 1837Nicholas PappasNo ratings yet
- Preposition, Conjunction and ParticiplesDocument22 pagesPreposition, Conjunction and ParticiplesAudrey MonicaNo ratings yet
- Kneehigh TheaterDocument2 pagesKneehigh Theaterapi-706488422No ratings yet
- The Illustrated Philosophy of FreedomDocument168 pagesThe Illustrated Philosophy of FreedomrudolfsteinerbooksNo ratings yet
- Grouped Data Mean, Median, ModeDocument15 pagesGrouped Data Mean, Median, ModeTricia EspañolNo ratings yet
- Module 7 Week 7 Dyadic Relationshp Followershp Delegation L SHIP 7 PDFDocument67 pagesModule 7 Week 7 Dyadic Relationshp Followershp Delegation L SHIP 7 PDFHarshithaNo ratings yet
- Hirschsprung DiseaseDocument14 pagesHirschsprung DiseaseFlordelyn Anuales100% (2)
- Educ - MidtermDocument8 pagesEduc - MidtermAn Jannette AlmodielNo ratings yet
- 5.1 RadioactivityDocument4 pages5.1 RadioactivitypanitiafiziksmkbNo ratings yet
- Mapeh 10 Exam 4th QuarterDocument2 pagesMapeh 10 Exam 4th QuarterMaybelyn de los ReyesNo ratings yet
- Ubd Unit Plan TemplateDocument6 pagesUbd Unit Plan Templateapi-309680087No ratings yet
- Removing Baseline Wander in ECG WaveformsDocument3 pagesRemoving Baseline Wander in ECG WaveformsSohaib AkhterNo ratings yet
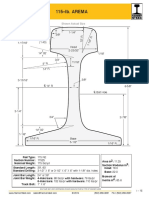
- Arema 115REDocument1 pageArema 115REAntonioNo ratings yet
- Emcee Script - ExpertMCDocument14 pagesEmcee Script - ExpertMCHARUN BONCHELNo ratings yet
- Social PhilosophyDocument20 pagesSocial PhilosophyPrincess Diane Gravides100% (1)
- Problem and Solution Electric FieldDocument10 pagesProblem and Solution Electric FieldSansen Diamante Colipano Jr.No ratings yet
- Numerical Grid Generation Techniques - NASADocument563 pagesNumerical Grid Generation Techniques - NASAMárioSilva100% (1)
- Quiz 2Document5 pagesQuiz 2Apples Ermida BanuelosNo ratings yet

































































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Oxford Handbooks Download LinkDocument5 pagesOxford Handbooks Download LinkAdithya Vishwanath43% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Buku Manpro Versi IndonesiaDocument375 pagesBuku Manpro Versi IndonesiaTaufan Widiarko100% (3)
- Acquired C1 Inhibitor Deficiencymanagement and PrognosisDocument14 pagesAcquired C1 Inhibitor Deficiencymanagement and PrognosisjalalfaizNo ratings yet
- ACE Inhibitor-Induced AngioedemaDocument14 pagesACE Inhibitor-Induced AngioedemajalalfaizNo ratings yet
- Lichen Planus and Its Management An Update and Observation Ijced 18 001Document5 pagesLichen Planus and Its Management An Update and Observation Ijced 18 001jalalfaizNo ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- Pityriasis RoseaDocument2 pagesPityriasis RoseajalalfaizNo ratings yet
- Lichen Planus: Santa Clara Medical Center, Department of Dermatology #472Document2 pagesLichen Planus: Santa Clara Medical Center, Department of Dermatology #472jalalfaizNo ratings yet
- Acne Keloidalis NuchaeDocument16 pagesAcne Keloidalis NuchaejalalfaizNo ratings yet
- Levamisole in L.PDocument5 pagesLevamisole in L.PjalalfaizNo ratings yet
- Pemphigus: Clinical FeaturesDocument7 pagesPemphigus: Clinical FeaturesjalalfaizNo ratings yet
- WartsDocument5 pagesWartsjalalfaizNo ratings yet
- PemphigoidDocument4 pagesPemphigoidjalalfaizNo ratings yet
- Candidiasis: Clinical FeaturesDocument4 pagesCandidiasis: Clinical FeaturesjalalfaizNo ratings yet
- UrticariaDocument5 pagesUrticariajalalfaizNo ratings yet
- Molluscum ContagiosumDocument2 pagesMolluscum ContagiosumjalalfaizNo ratings yet
- Herpes SimplexDocument5 pagesHerpes SimplexjalalfaizNo ratings yet
- 21 Molluscum Contagiosum PDFDocument2 pages21 Molluscum Contagiosum PDFjalalfaizNo ratings yet
- Tinea (Dermatomycosis)Document9 pagesTinea (Dermatomycosis)jalalfaizNo ratings yet
- Tinea VersicolorDocument2 pagesTinea VersicolorjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- Lichen Simplex ChronicusDocument3 pagesLichen Simplex ChronicusjalalfaizNo ratings yet
- Lupus Vulgaris of External NoseDocument3 pagesLupus Vulgaris of External NosejalalfaizNo ratings yet
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Drug ReactionsDocument11 pagesDrug ReactionsjalalfaizNo ratings yet
- Acne and Acneiform DermatosesDocument5 pagesAcne and Acneiform DermatosesjalalfaizNo ratings yet
- Meralgia Paresthetica: Case PresentationDocument2 pagesMeralgia Paresthetica: Case PresentationjalalfaizNo ratings yet
- I S D, TC, I S: Mechanisms of DiseaseDocument12 pagesI S D, TC, I S: Mechanisms of DiseasejalalfaizNo ratings yet
- Top 30 Skin DiseasesDocument32 pagesTop 30 Skin DiseasesjalalfaizNo ratings yet
- People vs. Umali, 193 SCRA 493, G.R. No. 84450 February 4, 1991Document12 pagesPeople vs. Umali, 193 SCRA 493, G.R. No. 84450 February 4, 1991Trea CheryNo ratings yet
- De Thi Giua Ki 1 Tieng Anh Lop 5 Co Dap An 2021Document28 pagesDe Thi Giua Ki 1 Tieng Anh Lop 5 Co Dap An 2021Đỗ Thanh XuânNo ratings yet
- Portraits of Courage PDF Full Book Online FreeDocument4 pagesPortraits of Courage PDF Full Book Online FreeDark UnicornNo ratings yet
- FM302 Financial Management in The Pacific Region: Week 4: Lecture 7 - Major Assignment Some Discussions and DirectionsDocument15 pagesFM302 Financial Management in The Pacific Region: Week 4: Lecture 7 - Major Assignment Some Discussions and DirectionsHitesh MaharajNo ratings yet
- TMS 3701Document2 pagesTMS 3701nnshabalala290No ratings yet
- Simon The Sportsman: Activity TypeDocument3 pagesSimon The Sportsman: Activity TypeEkaterina DatsenkoNo ratings yet
- In The Supreme Court of Texas: T S T, PDocument14 pagesIn The Supreme Court of Texas: T S T, PLaw&CrimeNo ratings yet
- UE18EE325 - Unit1 - Class4 - Performance Characteristics-StaticDocument16 pagesUE18EE325 - Unit1 - Class4 - Performance Characteristics-StaticGAYATHRI DEVI BNo ratings yet
- Private Files Module 3 Practical Research 2 Conceptual Framework and Hypothesis PDFDocument20 pagesPrivate Files Module 3 Practical Research 2 Conceptual Framework and Hypothesis PDFLovely IñigoNo ratings yet
- Words That HurtDocument5 pagesWords That Hurtsir_leoNo ratings yet
- Aquios LIS Interface SpecificationDocument56 pagesAquios LIS Interface SpecificationLuis AriasNo ratings yet
- The Travels of Macarius, Patriarch of Antioch: Written by his Attendant Archdeacon, Paul of Aleppo, In Arabic. Volume I and II. Translated By F. C. Belfour London: Printed for the Oriental Translation Fund, 1837Document8 pagesThe Travels of Macarius, Patriarch of Antioch: Written by his Attendant Archdeacon, Paul of Aleppo, In Arabic. Volume I and II. Translated By F. C. Belfour London: Printed for the Oriental Translation Fund, 1837Nicholas PappasNo ratings yet
- Preposition, Conjunction and ParticiplesDocument22 pagesPreposition, Conjunction and ParticiplesAudrey MonicaNo ratings yet
- Kneehigh TheaterDocument2 pagesKneehigh Theaterapi-706488422No ratings yet
- The Illustrated Philosophy of FreedomDocument168 pagesThe Illustrated Philosophy of FreedomrudolfsteinerbooksNo ratings yet
- Grouped Data Mean, Median, ModeDocument15 pagesGrouped Data Mean, Median, ModeTricia EspañolNo ratings yet
- Module 7 Week 7 Dyadic Relationshp Followershp Delegation L SHIP 7 PDFDocument67 pagesModule 7 Week 7 Dyadic Relationshp Followershp Delegation L SHIP 7 PDFHarshithaNo ratings yet
- Hirschsprung DiseaseDocument14 pagesHirschsprung DiseaseFlordelyn Anuales100% (2)
- Educ - MidtermDocument8 pagesEduc - MidtermAn Jannette AlmodielNo ratings yet
- 5.1 RadioactivityDocument4 pages5.1 RadioactivitypanitiafiziksmkbNo ratings yet
- Mapeh 10 Exam 4th QuarterDocument2 pagesMapeh 10 Exam 4th QuarterMaybelyn de los ReyesNo ratings yet
- Ubd Unit Plan TemplateDocument6 pagesUbd Unit Plan Templateapi-309680087No ratings yet
- Removing Baseline Wander in ECG WaveformsDocument3 pagesRemoving Baseline Wander in ECG WaveformsSohaib AkhterNo ratings yet
- Arema 115REDocument1 pageArema 115REAntonioNo ratings yet
- Emcee Script - ExpertMCDocument14 pagesEmcee Script - ExpertMCHARUN BONCHELNo ratings yet
- Social PhilosophyDocument20 pagesSocial PhilosophyPrincess Diane Gravides100% (1)
- Problem and Solution Electric FieldDocument10 pagesProblem and Solution Electric FieldSansen Diamante Colipano Jr.No ratings yet
- Numerical Grid Generation Techniques - NASADocument563 pagesNumerical Grid Generation Techniques - NASAMárioSilva100% (1)
- Quiz 2Document5 pagesQuiz 2Apples Ermida BanuelosNo ratings yet