
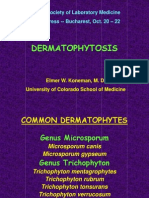
Tinea (Dermatomycosis)
Tinea (Dermatomycosis)
You might also like
- Tureks Orthopaedics - Principles and Their ApplicDocument1 pageTureks Orthopaedics - Principles and Their Applicqu402113No ratings yet
- LSVT Loud Patient Lecture Handout 2014Document12 pagesLSVT Loud Patient Lecture Handout 2014pancho_enNo ratings yet
- Oxford Handbooks Download LinkDocument5 pagesOxford Handbooks Download LinkAdithya Vishwanath43% (7)
- Check Your English Vocabulary For MedicineDocument57 pagesCheck Your English Vocabulary For MedicineМакс Колосов100% (1)
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- IT-11 DERMATOMIKOSIS SUPERFISIALIS Edit 8 OktDocument69 pagesIT-11 DERMATOMIKOSIS SUPERFISIALIS Edit 8 Oktputri.SpANo ratings yet
- Lesson 2 Superficial Cutaneous Mycosis HandoutsDocument8 pagesLesson 2 Superficial Cutaneous Mycosis HandoutsKhay Mae DonascoNo ratings yet
- Defi Nition and NomenclatureDocument4 pagesDefi Nition and NomenclatureintanphNo ratings yet
- Cutaneous Mycoses MikologiDocument10 pagesCutaneous Mycoses MikologisherinaNo ratings yet
- Fungal Infection of The SkinDocument74 pagesFungal Infection of The Skinary_puraNo ratings yet
- Lecture 2 MycologyDocument22 pagesLecture 2 MycologyDragon Gie30No ratings yet
- Dermatophytosis: EtiologyDocument6 pagesDermatophytosis: EtiologyTheresia FalentinaNo ratings yet
- DERMATOMYCOSISDocument114 pagesDERMATOMYCOSISQonita Qurrota AyunNo ratings yet
- DermatomycosesDocument32 pagesDermatomycosesp6hccq6jd7No ratings yet
- Tinea Corporis BologniaDocument4 pagesTinea Corporis BologniaHardiyanti HermanNo ratings yet
- Superficial MycosisDocument8 pagesSuperficial MycosisLuqman Al-Bashir FauziNo ratings yet
- MYCOSESDocument41 pagesMYCOSESDayana PrasanthNo ratings yet
- Tinea Corporis Pedia-1Document11 pagesTinea Corporis Pedia-1Denso Antonius LimNo ratings yet
- Title of The LecDocument22 pagesTitle of The LecWeird BoiNo ratings yet
- DermatophyteDocument8 pagesDermatophyteBhuvana RajNo ratings yet
- Superficial Fungal InfectionsDocument40 pagesSuperficial Fungal InfectionsMarimuthu PrabhakaranNo ratings yet
- Derma-Chronicles-issue 1 - 26-5-16 HiResDocument4 pagesDerma-Chronicles-issue 1 - 26-5-16 HiResParthMairNo ratings yet
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Palmoplantar PustulosisDocument6 pagesPalmoplantar PustulosisputraimanullahNo ratings yet
- Fungal InfectionDocument5 pagesFungal InfectionFiras HamidehNo ratings yet
- The Diagnosis and Management Of: Tinea CapitisDocument4 pagesThe Diagnosis and Management Of: Tinea CapitisQuraisy jamal sahilNo ratings yet
- Tinea Corporis, Tinea Cruris, Tinea Nigra, and Piedra: Dermatologic Clinics August 2003Document7 pagesTinea Corporis, Tinea Cruris, Tinea Nigra, and Piedra: Dermatologic Clinics August 2003Dicky KurniawanNo ratings yet
- Mycology: Clinical FindingsDocument5 pagesMycology: Clinical FindingsLuqman Al-Bashir FauziNo ratings yet
- Fungal Pathogens GroupingsDocument25 pagesFungal Pathogens GroupingsJhade Rio GadinganNo ratings yet
- Tinea Capitis: Audouinii), Which Give A Typical Green Fluorescence. T. Rubrum, The Commonest Cause of TineaDocument10 pagesTinea Capitis: Audouinii), Which Give A Typical Green Fluorescence. T. Rubrum, The Commonest Cause of TineaSyamsul ArifinNo ratings yet
- Super Ficial Fungal Infections: Key PointsDocument4 pagesSuper Ficial Fungal Infections: Key PointsBagus Putra KurniawanNo ratings yet
- Tinea CapitisDocument9 pagesTinea CapitisadityakafiberkahsmgNo ratings yet
- Unit 2 MycoDocument11 pagesUnit 2 MycoElyssa VergaraNo ratings yet
- Superficial Fungal Disorders of The SkinDocument121 pagesSuperficial Fungal Disorders of The SkinhaniNo ratings yet
- Classification of Fungal InfectionsDocument26 pagesClassification of Fungal Infectionstev26100% (1)
- Dermatofitosis 2011 1Document35 pagesDermatofitosis 2011 1Carmen Cajina Doña MamiNo ratings yet
- Translate TineaDocument12 pagesTranslate TineaIndah Permata SariNo ratings yet
- Epidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichDocument14 pagesEpidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichRS Tk IV PekanbaruNo ratings yet
- Superficial MycosesDocument26 pagesSuperficial Mycosesdhainey100% (3)
- Medical MycologyDocument14 pagesMedical Mycologyhawkar omerNo ratings yet
- 2003, Vol.21, Issues 3, Antifungal TherapyDocument186 pages2003, Vol.21, Issues 3, Antifungal TherapyRizweta DestinNo ratings yet
- Antifungal DrugsDocument16 pagesAntifungal DrugsAmrinder SagguNo ratings yet
- Dermatology Resident NotesDocument37 pagesDermatology Resident Notesedgar mandengNo ratings yet
- 1f97 PDFDocument8 pages1f97 PDFIqbal AbdillahNo ratings yet
- The Kerion An Angry Tinea Capitis PBDocument7 pagesThe Kerion An Angry Tinea Capitis PBprajnamitaNo ratings yet
- Topical Treatment of Common Superficial Tinea InfectionsDocument8 pagesTopical Treatment of Common Superficial Tinea InfectionsColate LocoNo ratings yet
- Annular Lesions in Dermatology: E Residents' PageDocument4 pagesAnnular Lesions in Dermatology: E Residents' PageAlba RosesNo ratings yet
- Assignment 2 Superficial and Subcutaneous Mycoses IgnacioDocument2 pagesAssignment 2 Superficial and Subcutaneous Mycoses IgnacioManuel LimchuNo ratings yet
- 4 DermatophytesDocument40 pages4 DermatophytesGeoemilia1No ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- BAHAN Tinea CapitisDocument28 pagesBAHAN Tinea CapitisYorika HafelaniNo ratings yet
- The Diagnosis and Management of Tinea CapitisDocument4 pagesThe Diagnosis and Management of Tinea CapitisKeyla Kehara PutriNo ratings yet
- LedesmaDocument6 pagesLedesmaAngela Dimaano SaladaNo ratings yet
- Tinea Pedis1Document7 pagesTinea Pedis1Ryan ChambersNo ratings yet
- Cut MycosesDocument56 pagesCut MycosesHafsa ImranNo ratings yet
- A Case of Tinea Pseudoimbricata by Trichophyton ToDocument4 pagesA Case of Tinea Pseudoimbricata by Trichophyton ToAndrés WunderwaldNo ratings yet
- Cutaneous and Subcataneous MycosesmDocument15 pagesCutaneous and Subcataneous MycosesmMaxamed Faarax XaashiNo ratings yet
- DermatophytesDocument10 pagesDermatophytesRaunaNo ratings yet
- Clase IiiDocument4 pagesClase IiiVictoria FloresNo ratings yet
- Paederus Dermatitis About To PrintDocument3 pagesPaederus Dermatitis About To PrintMinozu AryantiNo ratings yet
- Infectious Dermatosis (Bacterial Skin Infections)Document31 pagesInfectious Dermatosis (Bacterial Skin Infections)Melch PintacNo ratings yet
- Dermatology Atlas for Medical StudentsFrom EverandDermatology Atlas for Medical StudentsRating: 4 out of 5 stars4/5 (6)
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Acquired C1 Inhibitor Deficiencymanagement and PrognosisDocument14 pagesAcquired C1 Inhibitor Deficiencymanagement and PrognosisjalalfaizNo ratings yet
- ACE Inhibitor-Induced AngioedemaDocument14 pagesACE Inhibitor-Induced AngioedemajalalfaizNo ratings yet
- Lichen Planus and Its Management An Update and Observation Ijced 18 001Document5 pagesLichen Planus and Its Management An Update and Observation Ijced 18 001jalalfaizNo ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- Pityriasis RoseaDocument2 pagesPityriasis RoseajalalfaizNo ratings yet
- Lichen Planus: Santa Clara Medical Center, Department of Dermatology #472Document2 pagesLichen Planus: Santa Clara Medical Center, Department of Dermatology #472jalalfaizNo ratings yet
- Acne Keloidalis NuchaeDocument16 pagesAcne Keloidalis NuchaejalalfaizNo ratings yet
- Levamisole in L.PDocument5 pagesLevamisole in L.PjalalfaizNo ratings yet
- Pemphigus: Clinical FeaturesDocument7 pagesPemphigus: Clinical FeaturesjalalfaizNo ratings yet
- WartsDocument5 pagesWartsjalalfaizNo ratings yet
- PemphigoidDocument4 pagesPemphigoidjalalfaizNo ratings yet
- Candidiasis: Clinical FeaturesDocument4 pagesCandidiasis: Clinical FeaturesjalalfaizNo ratings yet
- UrticariaDocument5 pagesUrticariajalalfaizNo ratings yet
- Molluscum ContagiosumDocument2 pagesMolluscum ContagiosumjalalfaizNo ratings yet
- Herpes SimplexDocument5 pagesHerpes SimplexjalalfaizNo ratings yet
- 21 Molluscum Contagiosum PDFDocument2 pages21 Molluscum Contagiosum PDFjalalfaizNo ratings yet
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Tinea VersicolorDocument2 pagesTinea VersicolorjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- Acne and Acneiform DermatosesDocument5 pagesAcne and Acneiform DermatosesjalalfaizNo ratings yet
- Lichen Simplex ChronicusDocument3 pagesLichen Simplex ChronicusjalalfaizNo ratings yet
- Meralgia Paresthetica: Case PresentationDocument2 pagesMeralgia Paresthetica: Case PresentationjalalfaizNo ratings yet
- Drug ReactionsDocument11 pagesDrug ReactionsjalalfaizNo ratings yet
- I S D, TC, I S: Mechanisms of DiseaseDocument12 pagesI S D, TC, I S: Mechanisms of DiseasejalalfaizNo ratings yet
- Lupus Vulgaris of External NoseDocument3 pagesLupus Vulgaris of External NosejalalfaizNo ratings yet
- Top 30 Skin DiseasesDocument32 pagesTop 30 Skin DiseasesjalalfaizNo ratings yet
- Musculoskeletal AssessmentDocument69 pagesMusculoskeletal AssessmentWorku Kifle100% (2)
- SANIFECT - High Level DisinfectantDocument3 pagesSANIFECT - High Level DisinfectantHa HoNo ratings yet
- Benefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureDocument8 pagesBenefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureSonia LeeNo ratings yet
- Managing Cervical Spondylosis With Homeopathy TreatmentDocument2 pagesManaging Cervical Spondylosis With Homeopathy TreatmentDocco360No ratings yet
- COVID-19 in Nigeria... Matters ArisingDocument3 pagesCOVID-19 in Nigeria... Matters ArisingGreater K. OYEJOBINo ratings yet
- Bleeding Disorders: Drg. Gita Dwi Jiwanda Sovira, M.KesDocument26 pagesBleeding Disorders: Drg. Gita Dwi Jiwanda Sovira, M.KessaskiakonitaNo ratings yet
- WHO Dementia A Public Health PriorityDocument112 pagesWHO Dementia A Public Health PriorityJuliet Corner100% (1)
- Kolkata The Statesman 11-04-20Document12 pagesKolkata The Statesman 11-04-20Amir KhanNo ratings yet
- Packed Cell Volume (PCV) TestDocument3 pagesPacked Cell Volume (PCV) TestchineduNo ratings yet
- Microbiology: A Systems Approach, 2 Ed.: Chapter 16: Disorders in ImmunityDocument76 pagesMicrobiology: A Systems Approach, 2 Ed.: Chapter 16: Disorders in ImmunityJes OngNo ratings yet
- Data ProcessingDocument7 pagesData ProcessingJeanne ClaireNo ratings yet
- Surgery Sep+Oct+NovDocument122 pagesSurgery Sep+Oct+Novﻋﻤﻴﺪ ﺍﻟﺸﻤﻴﺮﻱNo ratings yet
- Pathology Bleeding DisordersDocument67 pagesPathology Bleeding DisordersMarcelliaNo ratings yet
- Aadya Mishra - Horoscope AnalysisDocument11 pagesAadya Mishra - Horoscope Analysisastrologylover BanglaNo ratings yet
- Cardiac BiomarkersDocument32 pagesCardiac BiomarkersMaham RehmanNo ratings yet
- Fourteen Home Remedies For Knee PainDocument12 pagesFourteen Home Remedies For Knee PainRatnaPrasadNalamNo ratings yet
- ParrotsDocument5 pagesParrotsNimra TaneemNo ratings yet
- Male Pelvic Floor - Advanced Massage and Bodywork PDFDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodywork PDFpujarze2No ratings yet
- Covid - 19Document12 pagesCovid - 19Prolita PattanayakNo ratings yet
- Organised Past Papers - GPDocument33 pagesOrganised Past Papers - GPgq4jyssrz2No ratings yet
- Revised MFDocument6 pagesRevised MFFrogman AdventuresNo ratings yet
- Vaccinations With Dr. Thomas Cowan 1 PDFDocument5 pagesVaccinations With Dr. Thomas Cowan 1 PDFChiorean Liviu OctavianNo ratings yet
- GR-No.-171127-FACTS of The CaseDocument2 pagesGR-No.-171127-FACTS of The CaseMaricon Bangalan-CanarejoNo ratings yet
- Overview of Sleep and Common Sleep DisordersDocument35 pagesOverview of Sleep and Common Sleep Disordersadamu mohammadNo ratings yet
- Mental Health Research PaperDocument12 pagesMental Health Research Paperapi-549190307No ratings yet
- The Middle Class Guide To Medicaid PlanningDocument9 pagesThe Middle Class Guide To Medicaid PlanningDoug ShannonNo ratings yet
- Health Problems Common in PRESCHOOLDocument15 pagesHealth Problems Common in PRESCHOOLJanelle Lois EscolanoNo ratings yet















































































































Download as pdf or txt
You might also like
- Tureks Orthopaedics - Principles and Their ApplicDocument1 pageTureks Orthopaedics - Principles and Their Applicqu402113No ratings yet
- LSVT Loud Patient Lecture Handout 2014Document12 pagesLSVT Loud Patient Lecture Handout 2014pancho_enNo ratings yet
- Oxford Handbooks Download LinkDocument5 pagesOxford Handbooks Download LinkAdithya Vishwanath43% (7)
- Check Your English Vocabulary For MedicineDocument57 pagesCheck Your English Vocabulary For MedicineМакс Колосов100% (1)
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- IT-11 DERMATOMIKOSIS SUPERFISIALIS Edit 8 OktDocument69 pagesIT-11 DERMATOMIKOSIS SUPERFISIALIS Edit 8 Oktputri.SpANo ratings yet
- Lesson 2 Superficial Cutaneous Mycosis HandoutsDocument8 pagesLesson 2 Superficial Cutaneous Mycosis HandoutsKhay Mae DonascoNo ratings yet
- Defi Nition and NomenclatureDocument4 pagesDefi Nition and NomenclatureintanphNo ratings yet
- Cutaneous Mycoses MikologiDocument10 pagesCutaneous Mycoses MikologisherinaNo ratings yet
- Fungal Infection of The SkinDocument74 pagesFungal Infection of The Skinary_puraNo ratings yet
- Lecture 2 MycologyDocument22 pagesLecture 2 MycologyDragon Gie30No ratings yet
- Dermatophytosis: EtiologyDocument6 pagesDermatophytosis: EtiologyTheresia FalentinaNo ratings yet
- DERMATOMYCOSISDocument114 pagesDERMATOMYCOSISQonita Qurrota AyunNo ratings yet
- DermatomycosesDocument32 pagesDermatomycosesp6hccq6jd7No ratings yet
- Tinea Corporis BologniaDocument4 pagesTinea Corporis BologniaHardiyanti HermanNo ratings yet
- Superficial MycosisDocument8 pagesSuperficial MycosisLuqman Al-Bashir FauziNo ratings yet
- MYCOSESDocument41 pagesMYCOSESDayana PrasanthNo ratings yet
- Tinea Corporis Pedia-1Document11 pagesTinea Corporis Pedia-1Denso Antonius LimNo ratings yet
- Title of The LecDocument22 pagesTitle of The LecWeird BoiNo ratings yet
- DermatophyteDocument8 pagesDermatophyteBhuvana RajNo ratings yet
- Superficial Fungal InfectionsDocument40 pagesSuperficial Fungal InfectionsMarimuthu PrabhakaranNo ratings yet
- Derma-Chronicles-issue 1 - 26-5-16 HiResDocument4 pagesDerma-Chronicles-issue 1 - 26-5-16 HiResParthMairNo ratings yet
- Fungal InfectionsDocument9 pagesFungal InfectionsCoral Srinivasa RamaluNo ratings yet
- Palmoplantar PustulosisDocument6 pagesPalmoplantar PustulosisputraimanullahNo ratings yet
- Fungal InfectionDocument5 pagesFungal InfectionFiras HamidehNo ratings yet
- The Diagnosis and Management Of: Tinea CapitisDocument4 pagesThe Diagnosis and Management Of: Tinea CapitisQuraisy jamal sahilNo ratings yet
- Tinea Corporis, Tinea Cruris, Tinea Nigra, and Piedra: Dermatologic Clinics August 2003Document7 pagesTinea Corporis, Tinea Cruris, Tinea Nigra, and Piedra: Dermatologic Clinics August 2003Dicky KurniawanNo ratings yet
- Mycology: Clinical FindingsDocument5 pagesMycology: Clinical FindingsLuqman Al-Bashir FauziNo ratings yet
- Fungal Pathogens GroupingsDocument25 pagesFungal Pathogens GroupingsJhade Rio GadinganNo ratings yet
- Tinea Capitis: Audouinii), Which Give A Typical Green Fluorescence. T. Rubrum, The Commonest Cause of TineaDocument10 pagesTinea Capitis: Audouinii), Which Give A Typical Green Fluorescence. T. Rubrum, The Commonest Cause of TineaSyamsul ArifinNo ratings yet
- Super Ficial Fungal Infections: Key PointsDocument4 pagesSuper Ficial Fungal Infections: Key PointsBagus Putra KurniawanNo ratings yet
- Tinea CapitisDocument9 pagesTinea CapitisadityakafiberkahsmgNo ratings yet
- Unit 2 MycoDocument11 pagesUnit 2 MycoElyssa VergaraNo ratings yet
- Superficial Fungal Disorders of The SkinDocument121 pagesSuperficial Fungal Disorders of The SkinhaniNo ratings yet
- Classification of Fungal InfectionsDocument26 pagesClassification of Fungal Infectionstev26100% (1)
- Dermatofitosis 2011 1Document35 pagesDermatofitosis 2011 1Carmen Cajina Doña MamiNo ratings yet
- Translate TineaDocument12 pagesTranslate TineaIndah Permata SariNo ratings yet
- Epidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichDocument14 pagesEpidemiological Trends in Skin Mycoses Worldwide: Blanka Havlickova, Viktor A. Czaika and Markus FriedrichRS Tk IV PekanbaruNo ratings yet
- Superficial MycosesDocument26 pagesSuperficial Mycosesdhainey100% (3)
- Medical MycologyDocument14 pagesMedical Mycologyhawkar omerNo ratings yet
- 2003, Vol.21, Issues 3, Antifungal TherapyDocument186 pages2003, Vol.21, Issues 3, Antifungal TherapyRizweta DestinNo ratings yet
- Antifungal DrugsDocument16 pagesAntifungal DrugsAmrinder SagguNo ratings yet
- Dermatology Resident NotesDocument37 pagesDermatology Resident Notesedgar mandengNo ratings yet
- 1f97 PDFDocument8 pages1f97 PDFIqbal AbdillahNo ratings yet
- The Kerion An Angry Tinea Capitis PBDocument7 pagesThe Kerion An Angry Tinea Capitis PBprajnamitaNo ratings yet
- Topical Treatment of Common Superficial Tinea InfectionsDocument8 pagesTopical Treatment of Common Superficial Tinea InfectionsColate LocoNo ratings yet
- Annular Lesions in Dermatology: E Residents' PageDocument4 pagesAnnular Lesions in Dermatology: E Residents' PageAlba RosesNo ratings yet
- Assignment 2 Superficial and Subcutaneous Mycoses IgnacioDocument2 pagesAssignment 2 Superficial and Subcutaneous Mycoses IgnacioManuel LimchuNo ratings yet
- 4 DermatophytesDocument40 pages4 DermatophytesGeoemilia1No ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- BAHAN Tinea CapitisDocument28 pagesBAHAN Tinea CapitisYorika HafelaniNo ratings yet
- The Diagnosis and Management of Tinea CapitisDocument4 pagesThe Diagnosis and Management of Tinea CapitisKeyla Kehara PutriNo ratings yet
- LedesmaDocument6 pagesLedesmaAngela Dimaano SaladaNo ratings yet
- Tinea Pedis1Document7 pagesTinea Pedis1Ryan ChambersNo ratings yet
- Cut MycosesDocument56 pagesCut MycosesHafsa ImranNo ratings yet
- A Case of Tinea Pseudoimbricata by Trichophyton ToDocument4 pagesA Case of Tinea Pseudoimbricata by Trichophyton ToAndrés WunderwaldNo ratings yet
- Cutaneous and Subcataneous MycosesmDocument15 pagesCutaneous and Subcataneous MycosesmMaxamed Faarax XaashiNo ratings yet
- DermatophytesDocument10 pagesDermatophytesRaunaNo ratings yet
- Clase IiiDocument4 pagesClase IiiVictoria FloresNo ratings yet
- Paederus Dermatitis About To PrintDocument3 pagesPaederus Dermatitis About To PrintMinozu AryantiNo ratings yet
- Infectious Dermatosis (Bacterial Skin Infections)Document31 pagesInfectious Dermatosis (Bacterial Skin Infections)Melch PintacNo ratings yet
- Dermatology Atlas for Medical StudentsFrom EverandDermatology Atlas for Medical StudentsRating: 4 out of 5 stars4/5 (6)
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Acquired C1 Inhibitor Deficiencymanagement and PrognosisDocument14 pagesAcquired C1 Inhibitor Deficiencymanagement and PrognosisjalalfaizNo ratings yet
- ACE Inhibitor-Induced AngioedemaDocument14 pagesACE Inhibitor-Induced AngioedemajalalfaizNo ratings yet
- Lichen Planus and Its Management An Update and Observation Ijced 18 001Document5 pagesLichen Planus and Its Management An Update and Observation Ijced 18 001jalalfaizNo ratings yet
- Cutaneous TuberculosisDocument10 pagesCutaneous TuberculosisjalalfaizNo ratings yet
- Pityriasis RoseaDocument2 pagesPityriasis RoseajalalfaizNo ratings yet
- Lichen Planus: Santa Clara Medical Center, Department of Dermatology #472Document2 pagesLichen Planus: Santa Clara Medical Center, Department of Dermatology #472jalalfaizNo ratings yet
- Acne Keloidalis NuchaeDocument16 pagesAcne Keloidalis NuchaejalalfaizNo ratings yet
- Levamisole in L.PDocument5 pagesLevamisole in L.PjalalfaizNo ratings yet
- Pemphigus: Clinical FeaturesDocument7 pagesPemphigus: Clinical FeaturesjalalfaizNo ratings yet
- WartsDocument5 pagesWartsjalalfaizNo ratings yet
- PemphigoidDocument4 pagesPemphigoidjalalfaizNo ratings yet
- Candidiasis: Clinical FeaturesDocument4 pagesCandidiasis: Clinical FeaturesjalalfaizNo ratings yet
- UrticariaDocument5 pagesUrticariajalalfaizNo ratings yet
- Molluscum ContagiosumDocument2 pagesMolluscum ContagiosumjalalfaizNo ratings yet
- Herpes SimplexDocument5 pagesHerpes SimplexjalalfaizNo ratings yet
- 21 Molluscum Contagiosum PDFDocument2 pages21 Molluscum Contagiosum PDFjalalfaizNo ratings yet
- PyodermasDocument5 pagesPyodermasjalalfaizNo ratings yet
- Tinea VersicolorDocument2 pagesTinea VersicolorjalalfaizNo ratings yet
- Deep Mycotic InfectionDocument5 pagesDeep Mycotic InfectionjalalfaizNo ratings yet
- Acne and Acneiform DermatosesDocument5 pagesAcne and Acneiform DermatosesjalalfaizNo ratings yet
- Lichen Simplex ChronicusDocument3 pagesLichen Simplex ChronicusjalalfaizNo ratings yet
- Meralgia Paresthetica: Case PresentationDocument2 pagesMeralgia Paresthetica: Case PresentationjalalfaizNo ratings yet
- Drug ReactionsDocument11 pagesDrug ReactionsjalalfaizNo ratings yet
- I S D, TC, I S: Mechanisms of DiseaseDocument12 pagesI S D, TC, I S: Mechanisms of DiseasejalalfaizNo ratings yet
- Lupus Vulgaris of External NoseDocument3 pagesLupus Vulgaris of External NosejalalfaizNo ratings yet
- Top 30 Skin DiseasesDocument32 pagesTop 30 Skin DiseasesjalalfaizNo ratings yet
- Musculoskeletal AssessmentDocument69 pagesMusculoskeletal AssessmentWorku Kifle100% (2)
- SANIFECT - High Level DisinfectantDocument3 pagesSANIFECT - High Level DisinfectantHa HoNo ratings yet
- Benefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureDocument8 pagesBenefits of RPD: Elements and Compromised Function. The Removal of Exostoses and Tori Is Not A Complex ProcedureSonia LeeNo ratings yet
- Managing Cervical Spondylosis With Homeopathy TreatmentDocument2 pagesManaging Cervical Spondylosis With Homeopathy TreatmentDocco360No ratings yet
- COVID-19 in Nigeria... Matters ArisingDocument3 pagesCOVID-19 in Nigeria... Matters ArisingGreater K. OYEJOBINo ratings yet
- Bleeding Disorders: Drg. Gita Dwi Jiwanda Sovira, M.KesDocument26 pagesBleeding Disorders: Drg. Gita Dwi Jiwanda Sovira, M.KessaskiakonitaNo ratings yet
- WHO Dementia A Public Health PriorityDocument112 pagesWHO Dementia A Public Health PriorityJuliet Corner100% (1)
- Kolkata The Statesman 11-04-20Document12 pagesKolkata The Statesman 11-04-20Amir KhanNo ratings yet
- Packed Cell Volume (PCV) TestDocument3 pagesPacked Cell Volume (PCV) TestchineduNo ratings yet
- Microbiology: A Systems Approach, 2 Ed.: Chapter 16: Disorders in ImmunityDocument76 pagesMicrobiology: A Systems Approach, 2 Ed.: Chapter 16: Disorders in ImmunityJes OngNo ratings yet
- Data ProcessingDocument7 pagesData ProcessingJeanne ClaireNo ratings yet
- Surgery Sep+Oct+NovDocument122 pagesSurgery Sep+Oct+Novﻋﻤﻴﺪ ﺍﻟﺸﻤﻴﺮﻱNo ratings yet
- Pathology Bleeding DisordersDocument67 pagesPathology Bleeding DisordersMarcelliaNo ratings yet
- Aadya Mishra - Horoscope AnalysisDocument11 pagesAadya Mishra - Horoscope Analysisastrologylover BanglaNo ratings yet
- Cardiac BiomarkersDocument32 pagesCardiac BiomarkersMaham RehmanNo ratings yet
- Fourteen Home Remedies For Knee PainDocument12 pagesFourteen Home Remedies For Knee PainRatnaPrasadNalamNo ratings yet
- ParrotsDocument5 pagesParrotsNimra TaneemNo ratings yet
- Male Pelvic Floor - Advanced Massage and Bodywork PDFDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodywork PDFpujarze2No ratings yet
- Covid - 19Document12 pagesCovid - 19Prolita PattanayakNo ratings yet
- Organised Past Papers - GPDocument33 pagesOrganised Past Papers - GPgq4jyssrz2No ratings yet
- Revised MFDocument6 pagesRevised MFFrogman AdventuresNo ratings yet
- Vaccinations With Dr. Thomas Cowan 1 PDFDocument5 pagesVaccinations With Dr. Thomas Cowan 1 PDFChiorean Liviu OctavianNo ratings yet
- GR-No.-171127-FACTS of The CaseDocument2 pagesGR-No.-171127-FACTS of The CaseMaricon Bangalan-CanarejoNo ratings yet
- Overview of Sleep and Common Sleep DisordersDocument35 pagesOverview of Sleep and Common Sleep Disordersadamu mohammadNo ratings yet
- Mental Health Research PaperDocument12 pagesMental Health Research Paperapi-549190307No ratings yet
- The Middle Class Guide To Medicaid PlanningDocument9 pagesThe Middle Class Guide To Medicaid PlanningDoug ShannonNo ratings yet
- Health Problems Common in PRESCHOOLDocument15 pagesHealth Problems Common in PRESCHOOLJanelle Lois EscolanoNo ratings yet