Download as pdf or txt
You might also like
- Assignment One Human DevelopmentDocument6 pagesAssignment One Human DevelopmentjenNo ratings yet
- Nursing Study Guide Answer KeyDocument176 pagesNursing Study Guide Answer KeyKelsey Browne68% (19)
- Never Sleep With Baby Reprint Current Pe PDFDocument7 pagesNever Sleep With Baby Reprint Current Pe PDFZachNo ratings yet
- Mckenna Why Babies Should NDocument19 pagesMckenna Why Babies Should NSj BernNo ratings yet
- Editorial: Breastmilk: It's Not Just For Breakfast Anymore!Document1 pageEditorial: Breastmilk: It's Not Just For Breakfast Anymore!lila bNo ratings yet
- evolutionary perspectivesDocument19 pagesevolutionary perspectivesPamela LabatutNo ratings yet
- OkayDocument12 pagesOkayCool LyricsNo ratings yet
- Parenting Advice Books About Child Sleep: Cosleeping and Crying It OutDocument8 pagesParenting Advice Books About Child Sleep: Cosleeping and Crying It OutNicole Eileen Almeida MarcosNo ratings yet
- Ex LinkwordsDocument1 pageEx LinkwordsManon HumbertNo ratings yet
- Bedsharing Promotes Breastfeeding: ObjectiveDocument8 pagesBedsharing Promotes Breastfeeding: ObjectiveZachNo ratings yet
- Sleep Medicine Reviews: Sarah L. Blunden, Kirrilly R. Thompson, Drew DawsonDocument8 pagesSleep Medicine Reviews: Sarah L. Blunden, Kirrilly R. Thompson, Drew DawsonNicole Eileen Almeida MarcosNo ratings yet
- Babies in Boxes and The Missing Links On Safe Sleep: Human Evolution and Cultural RevolutionDocument7 pagesBabies in Boxes and The Missing Links On Safe Sleep: Human Evolution and Cultural RevolutionZachNo ratings yet
- Sleep 19 9 685Document6 pagesSleep 19 9 685ZachNo ratings yet
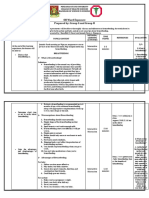
- OB Ward Exposure Prepared By: Group G and Group HDocument10 pagesOB Ward Exposure Prepared By: Group G and Group HJannah Marie A. DimaporoNo ratings yet
- MT101 Bio NurtpdfDocument4 pagesMT101 Bio NurtpdfFilipa PinaNo ratings yet
- Mother Nourish Nurture - Nap So SimpleDocument34 pagesMother Nourish Nurture - Nap So Simplepsych1505No ratings yet
- Healthy Birth Practice 6 - Keep Mother and Baby Together Its Best For Mother Baby and BreastfeedingDocument7 pagesHealthy Birth Practice 6 - Keep Mother and Baby Together Its Best For Mother Baby and BreastfeedingchewychockoNo ratings yet
- (2018) Benefits of A Bedtime Routine in Young ChildrenDocument16 pages(2018) Benefits of A Bedtime Routine in Young ChildrenFabian Opazo DelgadoNo ratings yet
- What Is Breastfeeding? Benefits of Breastfeeding?: Lessens The Risk of SIDSDocument2 pagesWhat Is Breastfeeding? Benefits of Breastfeeding?: Lessens The Risk of SIDSGarmaine ApostolNo ratings yet
- 1 s2.0 S0266613813002192 MainDocument11 pages1 s2.0 S0266613813002192 Mainnengsi susantiNo ratings yet
- NIH Public Access: Author ManuscriptDocument19 pagesNIH Public Access: Author ManuscriptHajrin PajriNo ratings yet
- Associations Between Single-Family RoomDocument10 pagesAssociations Between Single-Family RoomClaudia Rodrigues DiasNo ratings yet
- Adolecent ParentingDocument8 pagesAdolecent ParentingJusna KhanomNo ratings yet
- Controlled CryingDocument2 pagesControlled CryingDana MandrisoruNo ratings yet
- Maria Asuncion Silvestre: Improving Neonatal CareDocument2 pagesMaria Asuncion Silvestre: Improving Neonatal CareGeorge AngelesNo ratings yet
- Apa PaperDocument8 pagesApa Paperapi-301727553No ratings yet
- An Evidence Based Guide To Weaning Preterm Infants - 2009 - Paediatrics and Child Health PDFDocument10 pagesAn Evidence Based Guide To Weaning Preterm Infants - 2009 - Paediatrics and Child Health PDFSofia GkanaNo ratings yet
- API Infant Sleep Safety BrochureDocument2 pagesAPI Infant Sleep Safety BrochureJuliana AndradeNo ratings yet
- Infant and Child Development - 2007 - Germo - Child Sleep Arrangements and Family Life Perspectives From Mothers andDocument24 pagesInfant and Child Development - 2007 - Germo - Child Sleep Arrangements and Family Life Perspectives From Mothers andfetiye.erbilNo ratings yet
- Why Helicopter Parenting Fosters Failure - Psychology Today PDFDocument2 pagesWhy Helicopter Parenting Fosters Failure - Psychology Today PDFSherif Mohamed Abdel KerimNo ratings yet
- Perceived Toddler Sleep Problems, Co Sleeping, And.99340Document8 pagesPerceived Toddler Sleep Problems, Co Sleeping, And.99340Circa NewsNo ratings yet
- Miranda 2017Document3 pagesMiranda 2017saravcosta.psiNo ratings yet
- Intensive Mothering Beliefs Among Full-Time Employed Mothers of InfantsDocument25 pagesIntensive Mothering Beliefs Among Full-Time Employed Mothers of InfantsLetyAlarcónNo ratings yet
- Dr. Fallon Cook Murdoch Children's Research InstituteDocument2 pagesDr. Fallon Cook Murdoch Children's Research InstituteChester Llemos PalmonesNo ratings yet
- Steps To Successfully Breastfeed The Premature InfantDocument10 pagesSteps To Successfully Breastfeed The Premature InfantKholis FaisolNo ratings yet
- 2008 SuccionDocument12 pages2008 SuccionDaniela Belén Sánchez DuarteNo ratings yet
- Dev Dev0000425Document8 pagesDev Dev0000425Hoàng Nguyễn Ngọc GiangNo ratings yet
- Physiologic Infant Care Protocol 37Document10 pagesPhysiologic Infant Care Protocol 37ivana.cantouNo ratings yet
- Protocol Number 6 2019 RevisionDocument12 pagesProtocol Number 6 2019 RevisionclementinaNo ratings yet
- E20160772 FullDocument10 pagesE20160772 FullRaehana AlaydrusNo ratings yet
- Infant Sleep PositioningDocument14 pagesInfant Sleep Positioningapi-675533626No ratings yet
- Fatherhood As Taking The Child To Oneself: A Phenomenological Observation Study After Caesarean BirthDocument9 pagesFatherhood As Taking The Child To Oneself: A Phenomenological Observation Study After Caesarean BirthKissieNo ratings yet
- Culture Carrying and CommunicationDocument45 pagesCulture Carrying and CommunicationtotoksaptantoNo ratings yet
- Ent/115/6/1555.short: Article Tittle:the Impact of School Daily Schedule On Adolescent Sleep Published DateDocument3 pagesEnt/115/6/1555.short: Article Tittle:the Impact of School Daily Schedule On Adolescent Sleep Published DateleonielainecolbornNo ratings yet
- Transicion A La LMDocument10 pagesTransicion A La LMPaula Belén Rojas CunazzaNo ratings yet
- Ethical Considerations For Hospital Based Infant Feeding SupportDocument14 pagesEthical Considerations For Hospital Based Infant Feeding SupportNisarg PatelNo ratings yet
- What Is Tummy Time: Is It Necessary For Newborns?: by Joyce Miller, BSC, DC, PHD, and Sharon Vallone, DC, FiccpDocument3 pagesWhat Is Tummy Time: Is It Necessary For Newborns?: by Joyce Miller, BSC, DC, PHD, and Sharon Vallone, DC, FiccpzikmonNo ratings yet
- Psych 250 Paper FinalDocument8 pagesPsych 250 Paper Finalapi-546733227No ratings yet
- Trastormo Del Sueño en NiñosDocument14 pagesTrastormo Del Sueño en NiñosDra Carolina Escalante Neurologa de AdultosNo ratings yet
- Bounding 2Document11 pagesBounding 2Deliana MonizNo ratings yet
- Babywearing Practicesand EffectsDocument14 pagesBabywearing Practicesand EffectsCata Gomez UbillaNo ratings yet
- 2yr 2nd Sem MCN NotesDocument52 pages2yr 2nd Sem MCN Noteskc bpNo ratings yet
- PEO ModeloDocument9 pagesPEO ModeloSofia Ibarra GonzalezNo ratings yet
- Nresearch PaperDocument14 pagesNresearch Paperapi-400982160No ratings yet
- Research SeminarDocument27 pagesResearch SeminarAngelyn Adan VisitacionNo ratings yet
- VN - Infant CareDocument9 pagesVN - Infant CareliloNo ratings yet
- Lyceum-Northwestern University College of NursingDocument4 pagesLyceum-Northwestern University College of NursingReyjan ApolonioNo ratings yet
- Pacifier and Bottle Nipples: The Targets For Poor Breastfeeding OutcomesDocument3 pagesPacifier and Bottle Nipples: The Targets For Poor Breastfeeding Outcomesbeleg100% (1)
- Poa05074 33 41Document9 pagesPoa05074 33 41Nikka Caram DomingoNo ratings yet
- Holistic Infant Sleep Booklet: Maternal Health Manuals, #4From EverandHolistic Infant Sleep Booklet: Maternal Health Manuals, #4No ratings yet
- Fce Template Meta AnalysisDocument21 pagesFce Template Meta AnalysisZachNo ratings yet
- Solving Puzzle CachesDocument32 pagesSolving Puzzle CachesZachNo ratings yet
- A Video-Based Measure To Identify Autism Risk in InfancyDocument7 pagesA Video-Based Measure To Identify Autism Risk in InfancyZachNo ratings yet
- Editorial Perspective: Delivering Autism Intervention Through DevelopmentDocument4 pagesEditorial Perspective: Delivering Autism Intervention Through DevelopmentZachNo ratings yet
- Cox2020 Article APilotStudyComparingNewlyLicenDocument11 pagesCox2020 Article APilotStudyComparingNewlyLicenZachNo ratings yet
- Lai, Goh, Oei, Sung 2015Document12 pagesLai, Goh, Oei, Sung 2015ZachNo ratings yet
- DeVerdier2019 Article BlindnessAndAutismParentsPersp PDFDocument10 pagesDeVerdier2019 Article BlindnessAndAutismParentsPersp PDFZachNo ratings yet
- Autism Symptoms, Executive Functioning and Academic Progress in Higher Education StudentsDocument11 pagesAutism Symptoms, Executive Functioning and Academic Progress in Higher Education StudentsZachNo ratings yet
- The Impossibility of "Natural Parentingmfor Modern Mothers: On Social Structure and The Formation of HabitDocument12 pagesThe Impossibility of "Natural Parentingmfor Modern Mothers: On Social Structure and The Formation of HabitZachNo ratings yet
- Bedsharing Promotes Breastfeeding: ObjectiveDocument8 pagesBedsharing Promotes Breastfeeding: ObjectiveZachNo ratings yet
- 246 121 PDFDocument10 pages246 121 PDFZachNo ratings yet
- What's Best For Baby? Co-Sleeping and The Politics of InequalityDocument34 pagesWhat's Best For Baby? Co-Sleeping and The Politics of InequalityZachNo ratings yet
- Early Human Development: Wendy Middlemiss, Douglas A. Granger, Wendy A. Goldberg, Laura NathansDocument6 pagesEarly Human Development: Wendy Middlemiss, Douglas A. Granger, Wendy A. Goldberg, Laura NathansZachNo ratings yet
- Sleep 19 9 685Document6 pagesSleep 19 9 685ZachNo ratings yet
- Relationships Between Breast-Feeding, Co-Sleeping, and Somatic Complaints in Early ChildhoodDocument10 pagesRelationships Between Breast-Feeding, Co-Sleeping, and Somatic Complaints in Early ChildhoodZachNo ratings yet
- Never Sleep With Baby Reprint Current Pe PDFDocument7 pagesNever Sleep With Baby Reprint Current Pe PDFZachNo ratings yet
- HHS Public AccessDocument22 pagesHHS Public AccessZachNo ratings yet
- Parent-Child Bed-Sharing: The Good, The Bad, and The Burden of EvidenceDocument25 pagesParent-Child Bed-Sharing: The Good, The Bad, and The Burden of EvidenceZachNo ratings yet
- Mother Infant CO SLEEPING Understanding The.9Document8 pagesMother Infant CO SLEEPING Understanding The.9ZachNo ratings yet
- Babies in Boxes and The Missing Links On Safe Sleep: Human Evolution and Cultural RevolutionDocument7 pagesBabies in Boxes and The Missing Links On Safe Sleep: Human Evolution and Cultural RevolutionZachNo ratings yet
- Bed-Sharing and The Infant's Thermal Environment in The Home SettingDocument6 pagesBed-Sharing and The Infant's Thermal Environment in The Home SettingZachNo ratings yet
- Alshaban Et Al-2019-Journal of Child Psychology and PsychiatryDocument15 pagesAlshaban Et Al-2019-Journal of Child Psychology and PsychiatryZachNo ratings yet
- Zimbabwean Chiefs' Communique On Child MarriagesDocument3 pagesZimbabwean Chiefs' Communique On Child MarriagesYemurai NyoniNo ratings yet
- CSEC Social Studies Syllabus - Data CollectionDocument73 pagesCSEC Social Studies Syllabus - Data CollectionKenya Lambert100% (1)
- Conservative FeminismDocument26 pagesConservative Feminismirina8082No ratings yet
- A Concept Paper About Abortion Among TeenagersDocument5 pagesA Concept Paper About Abortion Among TeenagersQueennie VellNo ratings yet
- Jjs Midterm Q and ADocument3 pagesJjs Midterm Q and AMayck Jhoenell LomboyNo ratings yet
- FACES IV & The Circumplex Model: David H. Olson & Dean M. GorallDocument20 pagesFACES IV & The Circumplex Model: David H. Olson & Dean M. GorallJan EspinozaNo ratings yet
- NSG 123 Module 2Document128 pagesNSG 123 Module 2rigasanaorayNo ratings yet
- Physical Place and Cyber PlaceDocument20 pagesPhysical Place and Cyber PlaceDAVID MESIASNo ratings yet
- LanguageofsexandaidsinnepalDocument61 pagesLanguageofsexandaidsinnepalsackleyNo ratings yet
- Simpson Vieth Trustchapter 2021Document22 pagesSimpson Vieth Trustchapter 2021Marc DuabeNo ratings yet
- 6 - Chapter 5Document5 pages6 - Chapter 5Just Lynn PanaliganNo ratings yet
- Education and Child Care in ColomboDocument6 pagesEducation and Child Care in ColomboNelumNo ratings yet
- Glimpses From Women in IslamDocument11 pagesGlimpses From Women in IslamgakmailNo ratings yet
- Talley - Monte MonteDocument153 pagesTalley - Monte MontekatmartinsNo ratings yet
- The Functions of The FamilyDocument2 pagesThe Functions of The FamilyIan Adams100% (1)
- Age & Gender IssuesDocument9 pagesAge & Gender Issuesthanesh singhNo ratings yet
- Why Women Still Can't Have It AllDocument35 pagesWhy Women Still Can't Have It AllclaratgreenNo ratings yet
- Argumentative Essay-5Document6 pagesArgumentative Essay-5api-549246097No ratings yet
- LAW 343 Family Law I PDFDocument200 pagesLAW 343 Family Law I PDFLautechPredegree100% (2)
- Describe A Typical Family Unit and The Importance of Family in Your CountryDocument2 pagesDescribe A Typical Family Unit and The Importance of Family in Your CountryYhanna JgaNo ratings yet
- Adoption Rights of A Deserted Hindu WifeDocument16 pagesAdoption Rights of A Deserted Hindu WifeKv SrujanaNo ratings yet
- Chapter-8 Suggestions and ConclusionDocument4 pagesChapter-8 Suggestions and ConclusionAnkita ThakurNo ratings yet
- Measuring Differentiation SelfDocument9 pagesMeasuring Differentiation SelfDeborah NgaNo ratings yet
- 1.Chn Introduction and FamilyDocument7 pages1.Chn Introduction and FamilyLuzie Mae SuanNo ratings yet
- Family Relationships VocabDocument2 pagesFamily Relationships VocabJhonattan Lugo Isaza0% (1)
- Commentary On Mark's GospelDocument90 pagesCommentary On Mark's GospelRev. Raquel S. Lettsome, Ph.D.No ratings yet
- Whether Amendment Made To The Hindu Succession Act Achiving Gender EqualityDocument27 pagesWhether Amendment Made To The Hindu Succession Act Achiving Gender EqualityPriyesh Garg50% (2)
- ALKA - FAMILY - LAW ProjectDocument13 pagesALKA - FAMILY - LAW ProjectBani AroraNo ratings yet
- The Ethical and Religious Directives For Catholic Health Care Services: A Brief TourDocument51 pagesThe Ethical and Religious Directives For Catholic Health Care Services: A Brief TourPSH PMLNo ratings yet