Download as pdf or txt
You might also like
- Epidemiology Exam Questions and AnswersDocument107 pagesEpidemiology Exam Questions and Answersdimitrios82% (34)
- Bipolar SOAP NoteDocument8 pagesBipolar SOAP NoteRich Ambrose100% (1)
- Nursing Care Plan For Cesarean SectionDocument5 pagesNursing Care Plan For Cesarean SectionJon Gab Paquit85% (33)
- Krok 2 - 2021 - 26 JulyDocument19 pagesKrok 2 - 2021 - 26 JulyNicole VinnikNo ratings yet
- Essay On Swine FluDocument2 pagesEssay On Swine FluAbhishek Anand100% (1)
- COVID-19 Long Term EffectsDocument22 pagesCOVID-19 Long Term EffectsMcKenzie Stauffer100% (10)
- Anesthesia in Endodontics - Facts & Myths PDFDocument6 pagesAnesthesia in Endodontics - Facts & Myths PDFVioleta BotnariNo ratings yet
- MDER 130314 Bite Force and Dental Implant Treatment - 062717Document8 pagesMDER 130314 Bite Force and Dental Implant Treatment - 062717Joyce GalvezNo ratings yet
- 1 s2.0 S0099239921006488Document8 pages1 s2.0 S0099239921006488Zully Adanely Duron RobledoNo ratings yet
- New Directions in EndodonticsDocument16 pagesNew Directions in Endodontics李潮忠No ratings yet
- Inferior Dental Blocks Versus Infiltration DentistryDocument11 pagesInferior Dental Blocks Versus Infiltration DentistryQurrat-ul-AinNo ratings yet
- Endodontics: Colleagues ExcellenceDocument6 pagesEndodontics: Colleagues Excellenceyoona chanNo ratings yet
- Ecfeacutedentalpain PDFDocument6 pagesEcfeacutedentalpain PDFShikhaNo ratings yet
- Nicanor Reyes Sr. Street 1000 Manila, Philippines S.Y. 2019-2020Document2 pagesNicanor Reyes Sr. Street 1000 Manila, Philippines S.Y. 2019-2020Ritz RamosNo ratings yet
- Postscript: Inconsistencies in The Consensus Facet Joint GuidelinesDocument2 pagesPostscript: Inconsistencies in The Consensus Facet Joint Guidelineswinminoo7581No ratings yet
- Fingertip Injuries PDFDocument12 pagesFingertip Injuries PDFZóélkårnåín PhåntómhívéNo ratings yet
- 09 Concept of Minimally Dent Update 2007 PDFDocument7 pages09 Concept of Minimally Dent Update 2007 PDFGabrielTokićNo ratings yet
- Arthroscopic Surgery For Degenerative Knee Arthritis and Meniscal Tears: A Clinical Practice GuidelineDocument8 pagesArthroscopic Surgery For Degenerative Knee Arthritis and Meniscal Tears: A Clinical Practice Guidelineyehezkiel feriNo ratings yet
- Окклюзионная дизестзияDocument6 pagesОкклюзионная дизестзияАнна ЛужковскаяNo ratings yet
- Renton Forum Implantologicum 9-2 en 1308076Document6 pagesRenton Forum Implantologicum 9-2 en 1308076Franz Willman Chiguala MixanNo ratings yet
- Investor Science Conference Call: American Society of Clinical Oncology Gastrointestinal (ASCO GI) Cancers Symposium 2022Document42 pagesInvestor Science Conference Call: American Society of Clinical Oncology Gastrointestinal (ASCO GI) Cancers Symposium 2022BradGourdoNo ratings yet
- Oral Ulcers ADC JUL 2022Document8 pagesOral Ulcers ADC JUL 2022dragondostNo ratings yet
- Innovations in EndodonticsDocument14 pagesInnovations in EndodonticsLeHoaiNo ratings yet
- Adj 12392Document7 pagesAdj 12392Fahad AliNo ratings yet
- Anxiolysis in Dental Practice - A Report of Three CasesDocument7 pagesAnxiolysis in Dental Practice - A Report of Three CasesAnaMariaCastroNo ratings yet
- The Effect of Occlusal Reduction On Pain After Endodontic InstrumentationDocument5 pagesThe Effect of Occlusal Reduction On Pain After Endodontic InstrumentationDaniela FlorezNo ratings yet
- Management of AvulsedDocument7 pagesManagement of AvulsedDr.O.R.GANESAMURTHI100% (1)
- Biopsy - An OverviewDocument9 pagesBiopsy - An OverviewNadya AyuNo ratings yet
- EndodonticsDocument34 pagesEndodonticsAnggaHumalaBeltsazarNapitupuluNo ratings yet
- Preventing The Negative Sequelae of Tooth Extraction: DirectionsDocument2 pagesPreventing The Negative Sequelae of Tooth Extraction: DirectionsrizkiNo ratings yet
- Jurnal Resesi 6Document4 pagesJurnal Resesi 6viena mutmainnahNo ratings yet
- Acute Wound Management: Revisiting The Approach To Assessment, Irrigation, and Closure ConsiderationsDocument9 pagesAcute Wound Management: Revisiting The Approach To Assessment, Irrigation, and Closure ConsiderationsOscar Alexis Jiménez ViverosNo ratings yet
- Treating Wound InfectionsDocument12 pagesTreating Wound InfectionsOnSolomonNo ratings yet
- Scarano 2017Document9 pagesScarano 2017Lila karla leon villarNo ratings yet
- Local Anesthesia Drugs CDA 2006 MalamedDocument6 pagesLocal Anesthesia Drugs CDA 2006 MalamedSaj1985100% (2)
- Angle Orthod. 2016 86 4 625-30Document6 pagesAngle Orthod. 2016 86 4 625-30brookortontiaNo ratings yet
- Avoiding Surg ComplicationsDocument13 pagesAvoiding Surg ComplicationsbrendanNo ratings yet
- Complications in Endodontics: Bhavin Bhuva, Omar IkramDocument7 pagesComplications in Endodontics: Bhavin Bhuva, Omar IkramYuliana ChamorroNo ratings yet
- Spotlight On EndodonticsDocument22 pagesSpotlight On EndodonticsLeHoaiNo ratings yet
- TRAUMA ENDO Soft Tissue Response After Trauma-2Document20 pagesTRAUMA ENDO Soft Tissue Response After Trauma-2Prabhjot KaurNo ratings yet
- 2016 Nascimento - AbfractionDocument9 pages2016 Nascimento - AbfractionKAREN ANAIS URGILES ESPINOZANo ratings yet
- Care Plan 1 Complex HealthDocument5 pagesCare Plan 1 Complex HealthMadison OrgillNo ratings yet
- Drug-Study (Open Glaucoma)Document4 pagesDrug-Study (Open Glaucoma)aliannaNo ratings yet
- Admin,+14 jdmfs.v1i2.14+MYRNADocument4 pagesAdmin,+14 jdmfs.v1i2.14+MYRNAChita SintyaNo ratings yet
- Dento Alveolar TraumaDocument10 pagesDento Alveolar TraumaGowriNo ratings yet
- Use of Local Anesthesia For Pediatric DentalDocument6 pagesUse of Local Anesthesia For Pediatric DentalمعتزباللهNo ratings yet
- Pulp Therapy For Primary & Immature TeethDocument9 pagesPulp Therapy For Primary & Immature TeethdrayeshafeezNo ratings yet
- 3 LRA 10237 Epidural Analgesia For Labor 120710Document11 pages3 LRA 10237 Epidural Analgesia For Labor 120710Nur Rissa MaharanyNo ratings yet
- Articaine Vs LignoncaineDocument8 pagesArticaine Vs Lignoncaineisha MehtaNo ratings yet
- Appropriate Dressing For Better Healing WoundDocument58 pagesAppropriate Dressing For Better Healing WoundTania Hidayat100% (1)
- The Potential of Articaine As New Generation Of.18Document5 pagesThe Potential of Articaine As New Generation Of.18Ana Luisa SolísNo ratings yet
- NigerPostgradMedJ244230-2376709 063607Document6 pagesNigerPostgradMedJ244230-2376709 063607Dwiki GumelarNo ratings yet
- Di Abetes Insipidus: Collaboration & Referral - PhysicianDocument1 pageDi Abetes Insipidus: Collaboration & Referral - PhysicianDaisy Jane KoNo ratings yet
- Wound Essentials 8 1 Debridement Consensus Recommendations For PracticeDocument5 pagesWound Essentials 8 1 Debridement Consensus Recommendations For PracticeAndaz MortinNo ratings yet
- Int Endodontic J - 2022 - Abbott - Present Status and Future Directions Managing Endodontic EmergenciesDocument26 pagesInt Endodontic J - 2022 - Abbott - Present Status and Future Directions Managing Endodontic EmergenciesRazvan UngureanuNo ratings yet
- 3 Extracted Pages From Anna B. Fuks, Benjamin Peretz Eds. Pediatric Endodontics Current Concepts in Pulp Therapy For Primary and Young Permanent TeethDocument32 pages3 Extracted Pages From Anna B. Fuks, Benjamin Peretz Eds. Pediatric Endodontics Current Concepts in Pulp Therapy For Primary and Young Permanent TeethMona CameliaNo ratings yet
- Guarda Nardin 2008Document10 pagesGuarda Nardin 20086mqpjqh2vqNo ratings yet
- Drug-Induced Osteonecrosis of the Jaws: How to Diagnose, Prevent, and Treat ItFrom EverandDrug-Induced Osteonecrosis of the Jaws: How to Diagnose, Prevent, and Treat ItNo ratings yet
- Successful Local Anesthesia for Restorative Dentistry and Endodontics: Second EditionFrom EverandSuccessful Local Anesthesia for Restorative Dentistry and Endodontics: Second EditionNo ratings yet
- Peri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentFrom EverandPeri-Implant Complications: A Clinical Guide to Diagnosis and TreatmentNo ratings yet
- Endodontic Pain: Diagnosis, Causes, Prevention and TreatmentFrom EverandEndodontic Pain: Diagnosis, Causes, Prevention and TreatmentNo ratings yet
- Treating the Dental Patient with a Developmental DisorderFrom EverandTreating the Dental Patient with a Developmental DisorderKaren A. RaposaNo ratings yet
- Suspected Neurological Conditions Recognition and Referral PDF 66141663923653Document76 pagesSuspected Neurological Conditions Recognition and Referral PDF 66141663923653Alex GasnasNo ratings yet
- Orofacial Pain - An Update On Diagnosis and Management: PracticeDocument9 pagesOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasNo ratings yet
- Death PathologyDocument80 pagesDeath PathologyAlex GasnasNo ratings yet
- MITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorDocument25 pagesMITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorAlex GasnasNo ratings yet
- Facial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaDocument6 pagesFacial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaAlex GasnasNo ratings yet
- Hypoglosal Nerve PalsyDocument4 pagesHypoglosal Nerve PalsyAlex GasnasNo ratings yet
- Freemasonry Uncovering FreemasonryDocument113 pagesFreemasonry Uncovering Freemasonrycigsas1719100% (1)
- 2150 FullDocument7 pages2150 FullAlex GasnasNo ratings yet
- Funke Et Al-2011-The Journal of PhysiologyDocument13 pagesFunke Et Al-2011-The Journal of PhysiologyAlex GasnasNo ratings yet
- "Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceDocument4 pages"Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceAlex GasnasNo ratings yet
- Post-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraDocument7 pagesPost-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraAlex GasnasNo ratings yet
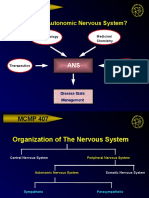
- MCMP 407: Why Study The Autonomic Nervous System?Document15 pagesMCMP 407: Why Study The Autonomic Nervous System?Alex GasnasNo ratings yet
- CNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument70 pagesCNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAlex GasnasNo ratings yet
- F5. Behavioural Syndromes Associated With Physiological Disturbance and Physical FactorsDocument77 pagesF5. Behavioural Syndromes Associated With Physiological Disturbance and Physical FactorsNeuro PsikiNo ratings yet
- MEDROXYPROGESTERONE (Medroxyprogesterone Acetate) : Why Is This Medicine Prescribed To You?Document1 pageMEDROXYPROGESTERONE (Medroxyprogesterone Acetate) : Why Is This Medicine Prescribed To You?Joar BonifacioNo ratings yet
- Treatments:: The Old, The New, and The UpcomingDocument68 pagesTreatments:: The Old, The New, and The UpcomingkarinaNo ratings yet
- Lpe2501 Writing Portfolio Task 3 (Writing Form - Draft)Document4 pagesLpe2501 Writing Portfolio Task 3 (Writing Form - Draft)amin badrulNo ratings yet
- Ang Crocs 2Document59 pagesAng Crocs 2MarufNo ratings yet
- Lecturenote - 2121234844biostatistics and Epidemiology (Stat3101) Handout Chapter-1Document20 pagesLecturenote - 2121234844biostatistics and Epidemiology (Stat3101) Handout Chapter-1McLord SelasiNo ratings yet
- Decee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverDocument5 pagesDecee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverJeff Mac Rae RamosNo ratings yet
- (Mico Biomed) Product Information Latest Version - 0706Document25 pages(Mico Biomed) Product Information Latest Version - 0706George TaoNo ratings yet
- Operation: TOMDocument14 pagesOperation: TOMDanielle PluzsikNo ratings yet
- Emergency Viva (Full)Document48 pagesEmergency Viva (Full)ashokarathnasingheNo ratings yet
- Liver, Biliary Tract and Pancreas PathologyDocument50 pagesLiver, Biliary Tract and Pancreas PathologybonadnadineNo ratings yet
- DR Hengky Chest PainDocument29 pagesDR Hengky Chest PainMohammad AriefNo ratings yet
- Body Temperature Monitoring SystemDocument4 pagesBody Temperature Monitoring Systemابو احمد نوفلNo ratings yet
- Methyldopa, Losartan K, Ascorbic AcidDocument4 pagesMethyldopa, Losartan K, Ascorbic AcidRico Mae ValenciaNo ratings yet
- Microblading Course 2017 PDFDocument67 pagesMicroblading Course 2017 PDFScribdTranslationsNo ratings yet
- CDI Documentation Tips - SurgeryDocument3 pagesCDI Documentation Tips - SurgeryLaluMohan KcNo ratings yet
- kslumuxZRMS2UrMNoJwJ - ADHD PPT SlidesDocument24 pageskslumuxZRMS2UrMNoJwJ - ADHD PPT SlidesKreshnik IdrizajNo ratings yet
- Congenital Cranial Dysinnervation Disorders - EyeWikiDocument3 pagesCongenital Cranial Dysinnervation Disorders - EyeWikitgrrwccj98No ratings yet
- Preventive, Promotive, Curative, RehabilitativeDocument54 pagesPreventive, Promotive, Curative, Rehabilitativetintu100% (1)
- Causes and Risk Factors For Attention-Deficit Hyperactivity DisorderDocument8 pagesCauses and Risk Factors For Attention-Deficit Hyperactivity DisorderFranthesa LayloNo ratings yet
- Successful Treatment of Multiple Common Warts With Intralesional OzoneDocument6 pagesSuccessful Treatment of Multiple Common Warts With Intralesional OzoneRubensNo ratings yet
- MeningitisDocument27 pagesMeningitisVinay SahuNo ratings yet
- Caffeine ADHDDocument7 pagesCaffeine ADHDTim GiordaniNo ratings yet
- C) Accuracy: Alhamdi Bara AspalalDocument6 pagesC) Accuracy: Alhamdi Bara AspalalKervy Jay AgraviadorNo ratings yet
- Pedia Disorders ExamDocument32 pagesPedia Disorders Examjoemer salamatNo ratings yet